 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
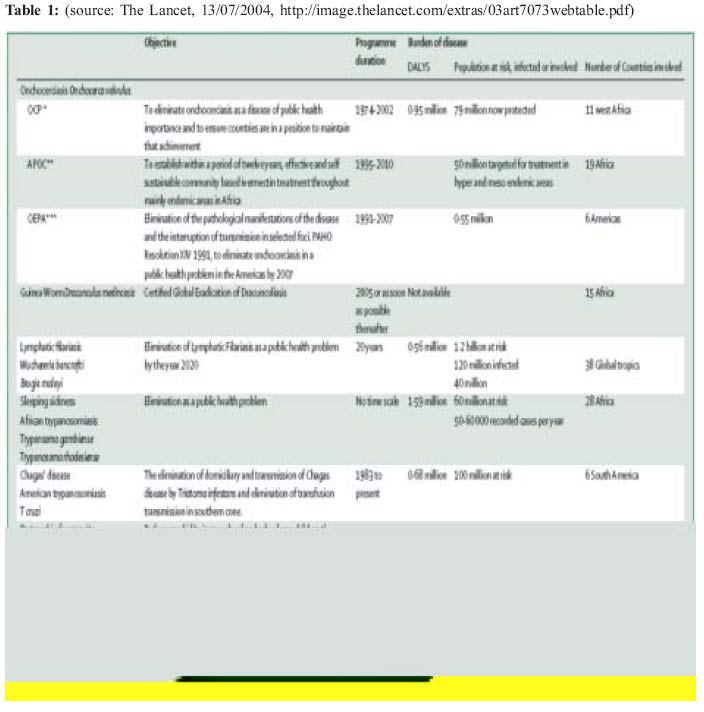
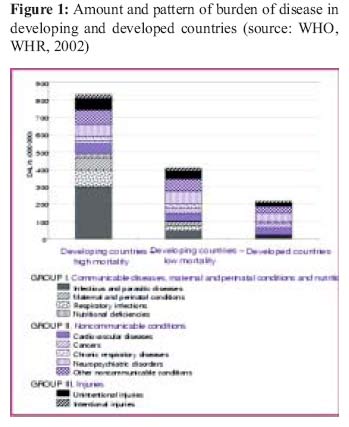
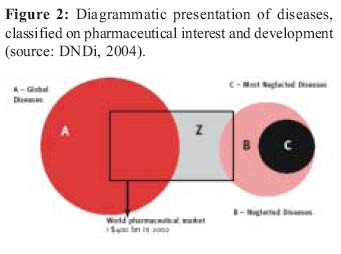
Health Policy and Development Journal, Vol. 2, No. 3, December, 2004, pp.217-226 INEQUITIES IN MEDICAL RESEARCH AND DEVELOPMENT: THE CASE OF NEGLECTED DISEASES Luigi Cicciò, Visiting Lecturer, Uganda Martyrs University Code Number: hp04035 Abstract According to the World Health Report 2002, preventable or treatable infectious and parasitic diseases are the primary causes of death worldwide. The limited availability of appropriate drugs to treat these diseases is a result of many causes, some biological (increasing parasite resistance), some merely economic and political (discontinued production or high cost of drugs, the lack of ongoing Research & Development -R&D- into these diseases). These so called "neglected diseases" are diseases represeningt an enduring medical need as they lack appropriate treatment. Examples of these diseases are, among others: leishmaniasis, Human AfricanTtrypanosomiasis, Chagas disease, and Lymphati cFilariasis. Drugs to treat these diseases have, virtually, no profitable market.Fourteen million people die of infectious diseases each year, 90% of them in poor countries of the Southern hemisphere. Many possible solutions have been proposed to overcome this serious global health problem, the most remarkable being the DNDi, (Drugs for Neglected Diseases Initiative). DNDI is an Médécins Sans Frontières (MSF) driven initiative to promote the development and production of effective, affordable, and easy-to-use drugs. However, there is little doubt that a crucial first step is to define a needs-driven research and to have a development agenda to assist policy makers, funding agencies, and the research community in setting priorities to address effectively the needs of developing countries. Introduction Neglected Diseases are communicable, tropical, and often deadly diseases. What distinguishes them from other diseases is that they are primarily affecting the poor people in developing countries, those with no purchasing power. As a result, the pharmaceutical industry, the major developer of new drugs, has very little or no interest in these diseases (DNDi 2002), which therefore acquire the term of "neglected". Since 2001, Médécins Sans Frontières (MSF) together with the Drugs for Neglected Diseases Working Group, an independent body comprising international health experts from the United Nations Development Programme (UNDP), the World Bank (WB) and the World Health Organisation (WHO) Special Programme for Tropical Diseases Research (TDR), created the not-for-profit Drugs for Neglected Diseases Initiative (DNDi). According to its mission, DNDi " seeks to address the need for research and development of new field-adapted, effective, and affordable drugs for patients suffering from 'neglected diseases". The strategy aims at collaborating mainly with developing countries organisations and governments and consists of several components: "…to harness accumulated knowledge and cutting-edge science and technology, to develop critically needed drugs for neglected diseases, making sure they are suitable for and accessible to the poorer patients of the world"(DNDi 2004a). The organisation is very active: it is starting clinical trials for two fixed-dose drug combinations against malaria, and counts another seven projects in the pipeline for sleeping sickness, visceral leishmaniasis and Chagas disease. In the field of disseminating information and advocating commitment, DNDi succeeded to organise an international" Meeting on a global framework for supporting health research and development in areas of market and public policy failure", held in Geneva in 2003. It also envisaged getting the issue of neglected diseases in the agenda of the forthcoming Ministerial Summit on Health Research that took place in Mexico in November 2004. Presently, the global agenda of the scientific community is very much concerned about the new developments in the field of AIDS, Tuberculosis (TB) and Malaria control respectively: scaling up the anti-retroviral drugs for HIV (WHO 2003a), expanding a community-based Directly Observed Treatment Short course (DOTS) for TB (WHO 2003b; WHO 2004) and introducing new anti-malarial drugs (Barnish et al. 2004; Kremsner & Krishna 2004) seem to be the prioritised areas of global common interest. Several initiatives have been purposely created to sustain it: the United Nations Agency for AIDS (UNAIDS), the International Aids Vaccine Initiative (IAVI), Roll Back Malaria (RBM) and Stop TB, culminating in the establishing of the Global Fund for Aids, TB and Malaria (GFATM). In addition, the United States Presidential Emergency Plan for AIDS Relief (PEPFAR) and many Public-Private Partnership initiatives, have been created to target these three diseases. The Millennium Development Goals (MDG), set at the end of last decade and intended to be achieved by 2015, have also a component on AIDS and malaria containment, as well as on mortality reduction, especially in children (United Nations 2000). Yet very little was set up - and sadly very little is being spent - on diseases whose prevalence is rampant throughout the developing world and that affect annually a large multitude of people, with high degree of mortality and disability and very severe effects on their health status. Onchocerchiasis, filariasis, trypanosomiasis together account for a total of over 3 million of DALYs lost and intestinal parasites, including schistosomiasis, are responsible for over 6 million DALYs lost (see Table 1). Neglected and very neglected diseases According to the World Health Report 2002 (WHO 2002), infectious and parasitic diseases - most of which are preventable or treatable - are still on the brink and they represent the primary causes of death worldwide (Fig. 1). But communicable diseases are not evenly distributed; rather they are concentrated among and are thus most important for the world poor. In developing countries, communicable illnesses are responsible for the majority of deaths (58.6 percent) and DALY loss (63.6 percent). This is a notably higher percentage than for the population of the world as a whole, in which communicable diseases cause 34.2 percent of all deaths and 43.9 percent of DALY loss, and higher still than for the world rich, among whom communicable diseases result in 7.7 percent of all deaths and 10.9 percent of DALY loss (Gwatkin & Guillot 2000). The final report of the WHO Commission on Macroeconomics and Health, released in 2001 (CMH 2001), had already stated that there exist three types of diseases (Fig. 2), classified on the basis of pharmaceutical interests and existing research and development (R&D): Type I: those incident in both rich and poor countries, with large numbers of vulnerable population in each (measles, hepatitis B, diabetes and tobacco-related). For theses diseases, incentives for R&D exist in the rich country markets. Type II: those incident in both rich and poor countries, but with a substantial proportion of the cases in the poor countries (HIV/AIDS, tuberculosis). For these diseases, incentives exist in the rich country markets, but the level of R&D spending on a global basis is not commensurate with disease burden. Type III: those overwhelmingly or exclusively incident in the developing countries (sleeping sickness, river blindness, Chagas disease, leishmaniasis). For these diseases, extremely little incentives for R&D exist, and essentially no commercially based R&D in the rich countries. These are the so-called very neglected diseases. Few drugs and very little research To make things worse, during the last 25 years, the gap between the development of drugs for tropical and non-tropical diseases has grown. Tropical diseases such as human African trypanosomiasis, visceral leishmaniasis (kala-azar), lymphatic filariasis, Chagas disease, dengue and schistosomiasis continue to cause significant morbidity and mortality. But they are neglected by the very mechanisms that ensure research and development of new drugs, as the patients suffering from them do not seem to represent a significant and attractive market (DNDi 2004a). A study published showed that in the last 25 years the pharmaceutical research has developed 1,393 new chemical entities, but only 16 were for tropical diseases and TB (some originating from the veterinary research) (Troullier 2002). In consideration of their usefulness, evidence of efficacy and costeffectiveness, all of the 16 newly developed drugs for those diseases have been included in the latest WHO Essential Drugs List (WHO 2003c), whereas only 21 (a strikingly low percentage of less than 2%) of all other drugs were included in the same list. Another recent study, conducted in the United States drug market, emphasised that from 1989 to 2000, the US Food and Drug Administration (FDA) rated only about one-quarter of new drug approvals to have therapeutic benefit over existing treatments (NIHCM 2002). It means that the remaining drugs did not appear to provide significant clinical improvement over marketed products, but yet they attracted the interest by pharmaceutical industry and absorbed a good share of its financial resources. There is a considerable lack of transparency in pharmaceutical R&D investment. The available data indicate that only about 10% of drug sales go towards R&D on new products. Measured by investment, only about one-fifth of the 10% is invested in innovative products (Hubbard and Love, 2004). A recent report by the Global Forum for Health Research has stated that "despite...(its)...critical role, health research has suffered from an overall lack of funding and from a huge discrepancy between the allocation of research funding and the diseases or conditions that account for the highest global disease burden" (GFfHR 2004). The Report also suggested a way forward: to increase funding for health research by developing countries; to create international research networks and more public-private partnerships; to build up the capacity of health research systems in developing countries. It is notable that a number of middle-income developing countries are already making significant investments in science: but the potential of developing countries researchers will be enhanced if they are integrated into the international research community, overcoming their sense of isolation and having access to the international production of knowledge (Fathalla 2004). Outstanding examples of neglected diseases Some of the neglected diseases which are particularly illustrative of the long-standing crisis in research and development in the pharmaceutical sector are discussed below. 1. Human African Trypanosomiasis (HAT, also known as sleeping sickness) is making a comeback, killing 150,000 people every year, especially in Africa. Drugs to treat HAT are old, scarce, highly toxic, and encounter parasite resistance (Legros 2002). Eflornithine (Ornidylâ) is a drug developed by the American firm Merell Dow in 1985 to which Gambian trypanosomiasis is very sensitive. The 14-day drug regimen proved to be highly effective and the shorter 7-day regimen an acceptable alternative in several African countries (WHO 1998). Given its high price, it was beyond the reach of those most seriously affected and its production was abandoned. Having "inherited" the drug when it took the company over, Hoechst Marion Roussel agreed to transfer marketing rights to the World Health Organisation, which, however, lacked the resources to manufacture it (Bulard 2000). In May 2001, after much pressure from international and non-governmental organizations, representatives of the pharmaceutical giant Aventis (generated by the merge of some companies, including Hoechst) signed an agreement with the WHO to guarantee a free production of eflornithine, as well as of other anti-trypanosomiasis drugs (pentamidine and melarsoprol) for at least 5 years (Barrett et al. 2003). But if it is to continue to be available, a sponsor will have to be found (Microsoft chairman, Bill Gates, is a possible candidate). In this worrying scenario, an encouraging development is the possible application of a newly devised diagnostic test that can make patient detection easier and more straightforward (Papadopoulos 2004). 2. It has been estimated that Chagas Disease, responsible for the loss of approximately 3 million disability-adjusted life years (DALYs) and 50,000 deaths annually, is the largest parasitic disease burden of Latin America and third, on a global scale, after malaria and schistosomiasis. An estimated 18 million people are living with the parasite infection and about 100 million people are at risk of acquiring it. This is about 25% of the whole region's population. Yet, only two drugs are available for its treatment and the R&D of new drugs is virtually non-existent. The available drugs, nifurtimox and benznidazole, are neither effective nor safe, with frequent side effects and subsequently high default rate along the long period of treatment (DNDi 2004b). An effective short course drug, with fewer side effects to improve compliance and successful completion of treatment is badly needed. 3. A useful tool against Meningococcal Meningitis, a disease particularly prevalent in African countries, where it causes recurrent epidemics, is an exemplary situation of neglected production, rather than neglected research. Patient management, especially in difficult settings and during an epidemic, would privilege the utilisation of intra-muscular oily chloramphenicol, as having the advantage of being both cheap and easy to administer. In 1995 the only company producing oily chloramphenicol, Roussel Uclaf (which merged with the Hoechst group in 1997 to form HMR) stopped its production. Initially, the International Development Association got it transferred to a laboratory in Malta. But now the money has run out and the drug is no longer produced. 4. Although Visceral Leishmaniasis (VL) is not ranked among the leading infectious causes of the global burden of disease, it is a life-threatening disease of great medical, social, and economic importance in its endemic areas. Its incidence is estimated at about 500,000 new cases each year. VL is fatal if left untreated. In 2001 there were 59,000 deaths reportedly due to VL, but the real number is thought to be significantly higher (Davies 2003). Leishmaniasis is also prone to epidemics, especially when previously unexposed populations are forced by conflicts and famine into endemic areas (DNDi 2004b). Good sero-diagnostic tests exist, but many are not suitable for field use, and tissue-invasive tests are necessary to show what is happening to the parasite load: the real needs are for simple tests on urine or saliva, which are known to contain leishmanial antigens. Antimonial drugs require 3-4 weeks hospital admission; the development of resistant strains is frequent especially in relapse cases (as it often happens for low-compliance and low-acceptability therapies). Antimonial drugs are associated to a higher risk of toxicity in HIV patients (Guerin 2002). Oral drugs are needed: currently, two drugs (paromomycin and miltefosine) are under clinical trials in India for assessing their safety and efficacy pattern. It is worth noting that controlling neglected diseases is cost-effective. Achievements in eliminating Chagas disease in Brazil and filariasis in China, controlling onchocerchiasis in West Africa and the ongoing campaign to eradicate Guinea Worm are valid examples. These diseases appear to be biologically more stable, contrasting with the evident difficulties in controlling malaria, TB and HIV/AIDS. In fact, the likelihood of drug resistance and insecticide resistance seem to be small for macro-parasites and macrovectors (Molyneux 2004). The re-emergence of Human African Trypanosomiasis in central Africa looks associated more to conflicts, deteriorated health services and poorly funded vector control programmes. But encouragingly, as soon as security conditions allowed it, sustained interventions resumed in Sudan, Liberia, Sierra Leone and other post conflict environments to control such diseases. A long-term, coordinated and consistent effort is needed, encompassing both, the development of new drugs and the scaling up of control measures. Few drugs and almost no vaccine If for drugs the present situation is rather stagnant and discouraging, for vaccines, where the technical hurdles are much greater than for medicines, the economic situation relating to private sector engagement in products for diseases of poverty, is even worse. Gaps are huge in the R&D of new vaccines: despite major recent breakthrough, the needs in developing countries are not being adequately addressed. The low uptake of new vaccines in developing countries has also been a major disincentive for manufacturers to invest in new vaccine R&D. In addition, the low prices negotiated over the years for traditional vaccines for use in developing countries have deterred manufacturers from developing vaccines for particular use in what are perceived to be "low profit" countries (WHO 2003d). As a matter of fact, today vaccines for neglected diseases are almost inexistent (WHO 2003e). In many fortunate cases, advances in vaccine technology directed for the North has had benefits for the South. But there are cases of vaccine being developed for diseases that had potential for use in the developing world, but not developed for such use for economic reasons: for example, the standard meningitis vaccine for the North does not adequately cover the South-Saharan meningitis belt, because it results from a different strain (Ridley 2004). In particular, a new strain W has recently emerged as a cause of epidemics, first in Burkina Faso, afterwards in other African countries of the so called "meningitis belt". WHO recently reached an agreement with Glaxo-Smith-Kline for the production of 6 million doses of the appropriate triple ACW vaccine at 1 Euro per dose. However, to ensure production, WHO would have to raise the required funds for establishing a revolving emergency stock (WHO 2003f). It has been estimated that less than 10% of global spending on health research is devoted to diseases or conditions that account for 90% of the global disease burden and vice versa (Global Forum for Health Research 2002). This is the so called '10/90 gap', whereby the lack of disease-specific research has left with current technical tools no longer sufficient for effective disease control; it has also given rise to a global 'drug gap' (Reich 2000), in which the private sector invests almost exclusively in drugs for the rich world that will be marketable and profitable. The possible causes At least five main hurdles have been identified to pharmaceutical R&D for neglected infectious diseases (Webber & Kremer 2001): The state of the science: The lack of understanding of some diseases, coupled with the complexity of the science and technology involved, makes the prospect of finding new medicines and vaccines uncertain and therefore risky. This lack of understanding would be likely to limit the investment that is prudent for industry to make. But indeed, lack of scientific knowledge is appears to be just an alleged barrier to drug development: much is known about the biology, immunology, and genetics of leishmania, trypanosomes and other parasites (Zumia 2002). Though the genetic composition of these micro-organisms has not yet been coded, these parasites have been studied for long, and they usually show a low tendency to produce mutants. Their interactions with hosts and the environment are also widely known: therefore, the technological gap is not a persuasive reason. Other issues seem to be the main obstacle to the translation of this knowledge into actual benefit for patients. Fear that intellectual property protection will be inadequate Industry continues to be concerned about protection for innovation because of challenges to the principle of intellectual property and the lack of enforcement of international intellectual property rights. Undermining patent protection could discourage innovative activity on the part of industry, while strengthening patent protection could come at the expense of reduced access. Insufficient access: Weaknesses in country-level physical, medical, financial, and political infrastructure mean that many existing products needed by people in developing countries are not being purchased by patients, health care facilities, governments, or nongovernmental organizations. There is a very real danger that even if new products are developed, they will not be purchased and made available to those who need them. Low accessibility to new products is particularly real if the current system of pharmaceutical patent protection does not sufficiently account for affordable prices, generic competition and compulsory licences in cases of public health emergencies (Cicciò 2004). Identifying priorities: Insufficient information about the number of patients, the effectiveness of existing products and patient access makes it difficult for companies to identify priority markets. Good country-level data about the incidence and prevalence of diseases and the prospects of patients seeking and receiving appropriate medical care are important components for establishing viable markets. This argument, too, is fairly weak: though it is true that the majority of poor countries have an insufficient, irregular and incomplete reporting system, whose estimates have to be cautiously considered, still, reasonable baseline information for setting priorities are both locally and internationally available. Poor expected market returns: In the case of neglected infectious diseases, the number of those afflicted is very large, but their individual purchasing power is generally small: the small commercial estimates of market size for some diseases create doubt that returns will cover investments. This looks to be the very reason outweighing all the previous ones. Additional reasons given for the existing stagnant progress against neglected diseases include the belief that investments in basic research alone will automatically lead to successful development of new tools disregarding the difficult translation of health research into policy and practice -. According to some observers, an important aspect is the low priority given to public health and health research by most disease-endemic countries themselves, where military-oriented governments are prone to finance armed conflicts at the expense of the health systems and services to the population (Morel 2003). For sure, wars, insecurity and political instability have largely contributed to the failure in the operating public health interventions for communicable diseases control. Though, this seems to be just a predisposing factor, whereas the pivotal role is being played by the lack of pharmaceutical industry investments. The pharmaceutical industry only enters into public-private partnerships when it sees at least some potential market for its products. For example, although people with malaria in the world's poorest countries cannot afford to pay for new malaria drugs, Western travellers can. Similarly, patients with tuberculosis or HIV in Africa or India cannot afford to purchase new treatments. However, many patients in the United States or Europe, whose health expenditure is covered by government run health sector or social health insurance programmes, can pay for these treatments. When the pharmaceutical industry sees enough of a market, the public sector then has sufficient leverage, or bargaining power, to persuade the private sector into a partnership. The bargaining power involves creating favourable conditions that make it attractive for industry to invest in drug development (grants, tax credits, public support for clinical trials, etc), or creating a purchase fund for buying the new drug once it is developed (Yamey 2002). When it comes to the world's most neglected diseases, however, these present absolutely no market opportunities. Without such opportunities, there is no incentive for the pharmaceutical industry to invest in drug research and development. The patients have no purchasing power, no vocal advocacy group is pleading for their needs, and no strategic interests - military or security - are driving concern about these conditions. This is why no public-private partnerships exist specifically for the most neglected diseases. At times, other external factors prevail. Melarsoprol is the most commonly used
drug for trypanosomiasis. It is an arsenic-containing product whose production
is technically difficult and financially unprofitable. To make decisions more
complicated, environmentalists in Germany have been seeking a ban on the production
of the arsenical molecule on the basis of rivers and subterranean waters contamination
by its toxic by-products (McMichael 1997).
In today's market-driven global economy, national governments have increasingly withdrawn to the sidelines, and the health sector is by no means an exception: over the last 30 years governments have largely relinquished control of drug development, supply and pricing decisions to the private sector, whose interests lie in maximising profits and growth, not in identifying and filling health needs. And yet world spending on R&D was never so high, reaching an estimated amount of US$ 70-75 billion for 2000, with the private sector as the biggest investor (Pecoul 2003). In most Western countries, the impact of this change has been ameliorated by health insurance systems, public subsidies or expensive initiatives (like the Orphan Drug Act in the USA, whereby government bears the costs of drug production for rare diseases of public health priority). However, this is not the case in developing countries, where governments are often too poor to shield patients from the impact of industry production and pricing strategies (Moran 2003). Drug companies have increasingly narrowed their research to focus on money-spinner drugs and diseases. The 10 best-selling drugs worldwide are: 4 for depression, 2 for cholesterol, 2 for hypertension, 1 for peptic ulcers and 1 for fever (Pharmaceutical Executive 2000). Proposed solutions Governments could expand direct funding for drug development, either through the existing academic institutions or through funding of existing companies to carry out specific drug R&D. Such directed drug development funding could be similar to existing non-profit development projects, such as those currently resourced to address treatments for previously neglected diseases like malaria and tuberculosis (Hubbard & Love 2004). Examples of such projects are the Medicines for Malaria Venture, the Global Alliance for TB Drug Development, the International AIDS Vaccine Initiative. The vast majority of these organisations owe their existence to funding from a limited number of foundations and government donors. If the donors decide to phase out for any reason, it would be likely to expect an irreversible and dramatic reduction of funds and activities. Many government proposals have supported the introduction of "push and pull" mechanisms to stimulate R&D of neglected diseases. "Push mechanisms" attempt to reduce the cost of R&D through incentives for the pharmaceutical industry (direct public funding for R&D in form of research grants, tax credits for R&D, investment in clinical trial infrastructure and fast tracking). On the other hand, "pull mechanisms" are used to enhance the attractiveness of the market to firm entry through enhanced intellectual property rights (longer patents on certain products), tax credits on sales, and advance purchase funds. Although all these possible solutions looked attractive in other fields (providing drugs for rare diseases, for instance), careful consideration must be given to whether such incentives would actually be effective, and more importantly, whether they could create any undesirable or perverse incentives (Mrazek & Mossialos 2003). An alternative (and rather provocative) proposal considers the huge different existing in available funds and asks as provisional solution to allocate a small fraction of the Global Fund resources to overcome the impasse in neglected diseases research and control (Molyneux 2004). Other proposed solutions include a full exploration of the potential of modern science and technology; new arrangements and conditions so that the best use is made of research for policy-making; serious engagement of disease-endemic countries in a new, international pharmaceutical policy for all neglected diseases (Morel 2003). Capacity building networks in developing countries is often advocated (MSF 2002), in conjunction with governmental and inter-governmental involvement in the sector of drug development, in order to proactively stimulate discovery of easy-to-use, affordable and effective drugs. Progress in research is also driven by free exchange of information, which cannot be expected in the case of competition-driven industries. This is the reason why some authors have advocated a complete openness with intermediate research outputs, in order to enhance the yield of a final successful product, as well as a radical modification of existing pharmaceutical trade rules based only on intellectual property and monopoly incentives (Hubbard & Love 2004). Conclusion
The entire issue of neglected diseases needs to be looked at in a broader framework, where inequities in global health care, unavailability of the needed drugs for an increasing disease burden, uneven public allocations for health and the dictating demands of the pharmaceutical industry are all related elements, together with the ethical aspects of health research. In fact, a further contribution to the unequal and asymmetric relation between poor countries and the medical research, particularly in the field of HIV/AIDS, consists of a sort of perverse attraction for developing countries shown by researchers. It is remarkable that scientific trials conducted in populations with a high incidence of new HIV infections have multiplied in recent years: primarily, the reason is for producing valid and meaningful results, otherwise difficult to achieve; and the genetic variability of HIV requires that candidate vaccines be tested in different areas where different strains are present. However, we should not forget that research in Africa is easier to perform due to weak regulatory systems, pervasive poverty, endemic diseases, and inadequate health care systems. These factors affect both the ease of performing trials and the selection of trials that can potentially benefit the populations of the countries under study. Moreover, there are other questionable incentives for carrying out studies in Africa: lower risks of litigation, less stringent ethical review, and populations prepared to cooperate with almost any study that appears curative in nature. As regulations at home become more restrictive and funding for studies abroad increases, research in the developing world looks relatively attractive (Silverio 2002). The Helsinki Declaration and the following revisions (WMA 1964) are expected to rule and provide guidelines to health research, though there were instances where application of a double standard for studies conducted in developed and developing countries was reported (Raja 2002). Ethical Review Committees in some developing countries are likely to be most vulnerable to unethical or exploitative clinical research. Even more important, researchers in developing nations derive substantial individual and institutional benefits from sponsored research, which may represent a conflict of interests. To alleviate suffering, to show respect for persons, to be sensitive to cultural differences, and not to exploit the vulnerable, should be the governing values of any serious health research (Nuffield Council on Bioethics 2002). It is an undisputed mandatory task for any committed challenge against neglected diseases and for any positive support directed to all neglected people. References:
|

{kind=link}
{kind=link}
{kind=link}