 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
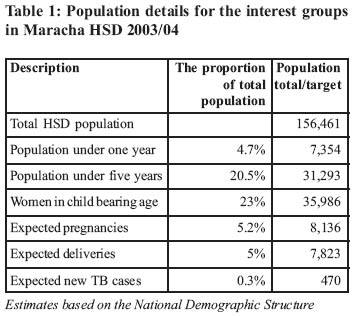
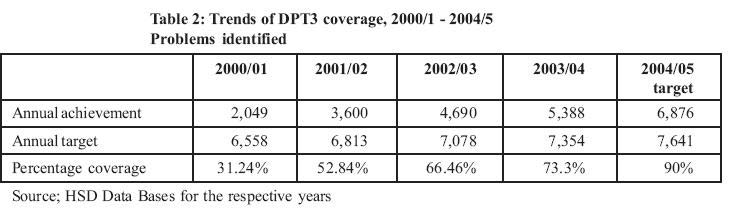
Health Policy and Development Journal, Vol. 2, No. 3, December, 2004, pp.262-270 INNOVATIVE APPROACHES TO COMMUNITY MOBILISATION FORIMMUNISATION IN MARACHA HEALTH SUB DISTRICT, ARUA DISTRICT Alfred Driwale, Deputy District Director of Health Services, Maracha Health Sub District, Arua District Code Number: hp04041 Abstract For years, the vaccination coverage for the indicator doses (DPT3) in Maracha Health Sub-District (HSD) have not reached the 80% target set by the Ministry of health. The Health Sub District management team brainstormed on the reasons for the persistently poor performance and charted the way forward in one of the review meetings. An approach to community mobilisation involving the sub-counties was agreed upon and was found to have improved the vaccination coverage of the HSD by 36% in the last four months of the financial year after the review meeting. The direct financial cost of immunisation per child reduced by 40% for the two periods July-February and February-June of the financial year where different approaches to mobilisation were used. It can be concluded that it is possible to attain and sustain vaccination coverage of children above 80% for all the vaccines by just mobilising the population. HSDs indeed the Health units have to work through and with sub country systems. Introduction Health services have been decentralised to the districts and further to the Health Sub-districts (HSD) at the level of counties. Arua district has 64 functional Health units distributed in seven HSDs. Four of the HSDs are headed by HC IV, two by PNFP Hospitals and one by Arua Regional Referral Hospital. One of the responsibilities of a HSD is to carry out operational research. Maracha HSD, with 10 lower level health units, is headed by Maracha hospital which belongs to Arua diocese and is affiliated to Uganda Catholic Medical Bureau (UCMB). It is a Private Not for Profit (PNFP) hospital that has been mandated to run Maracha HSD by the government. The HSD covers seven subcounties which have 40 parishes and 40 vaccination posts. Each post has two post mobilisers. The post mobilisers are members of the community who are chosen by the community to mobilise mothers to bring their children for vaccination on agreed days to a chosen location (post). These are people with acceptable character and influential in the communities. Most of them were trained with support from UNICEF as members of the Parish Development Committees (PDCs) about four years ago. Others were trained using funds from the Uganda National Expanded Programme on Immunisation (UNEPI) funds about three year ago. A parish has one post which is visited once a month by health workers for vaccination. The health sector mandate is to deliver the Uganda National Minimum Health Care Package (UNMHP). The programme areas are; Control of Communicable Diseases such as Malaria, Sexually Transmitted Infections, HIV/AIDS and Tuberculosis/leprosy; Child health such as immunisation, sexual and reproductive health and rights, mental health, other public health measures like environmental health and epidemic/ disaster preparedness and response, nutrition, clinical care including prevention of disability and rehabilitation. Delivering this package of services is aimed at reducing morbidity and mortality among the population. This package addresses most of the health problems of the country through promotive, preventive and curative activities. The Expanded Programme on Immunisation (EPI) falls under Child Health. The vaccines routinely given to children are: BCG, Polio, Diphtheria-Pertussis-Tetanus (DPT), Hepatitis B, Haemophilus influenza and measles. The Health Sector Strategic Plan (HSSP) indicators for this programme are the vaccination coverage of children under one year with the third and last dose of DPT 3 and measles. The national coverage targets are set at 80% in the HSSP. This is considered a proxy indicator for coverage with the other vaccines. The population of Maracha HSD in 2003/04 was 156,461 as projected from the 2002 population census. The target population for the routine vaccination are the children who are below one year of age see the Table 1. Children above one year but below five years may be vaccinated but do not contribute to the achievement of vaccination. Maracha HSD has not achieved the 80% target in the last four years as indicated in the trends in Table 2 below. The trends though improving are still below the national targets. In one of the HSD performance review meetings, the HSD management team, comprising all the staff in charge of peripheral health units in the HSD, health assistants in all the Sub-counties, and the hospital's Community Health Department met to review the situation of immunisation in the HSD. They noted that by February 2004 (3rd quarter) the projected DPT3 coverage of the HSD for the end of 2003/2004 FY would have been about 57% (projection from trends). This would be very far from the target of 80% and below the achievement of the previous year 2002/2003 which was 66.46%. They brainstormed on the factors that lead to poor vaccination coverage in the HSD. These could be summarised as follows:
Following the problems identified, a resolution was made to activate and utilise all the different stakeholders to mobilise the mothers, as a key strategy for improving the vaccination coverage. The goal of the intervention: The agreed goal was to increase the EPI (DPT3) coverage from 66.46% (2002/03) to 80% (2003/2004) and sustain it above 80% in subsequent years by making sub-counties take responsibility for the mobilisation of mothers and caretakers for vaccination. Strategy It was agreed that the best strategy would be to define the roles of the different stakeholders in vaccination, and to develop their capacity to perform their assignments in their respective catchment areas. For instance: mobilisation, vaccination, cold chain maintenance, and coordination had to be separated and performed by different teams. Due to resource constraints in the pilot phase, the strategy was limited to structural or organisational aspects only. Capacity building aspects were not tackled yet; e.g. no volunteer vaccinators were trained. The results that follow are only attributable to better mobilisation of the stakeholders. Objectives of the intervention
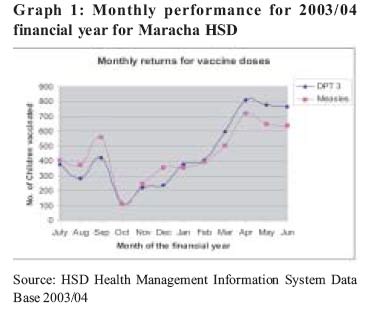
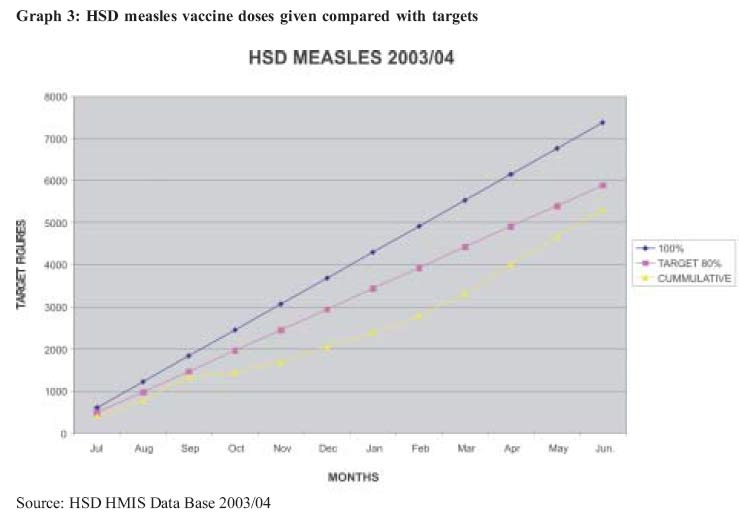
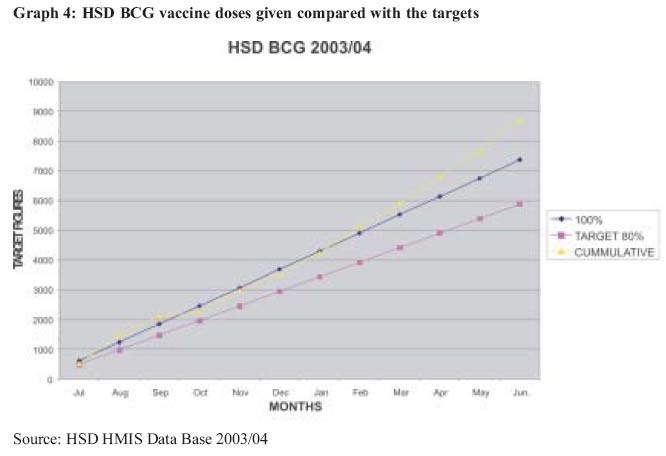
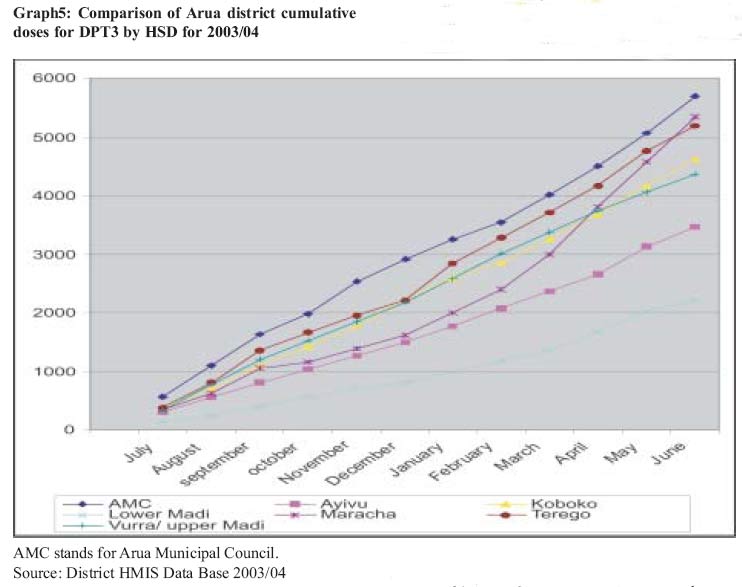
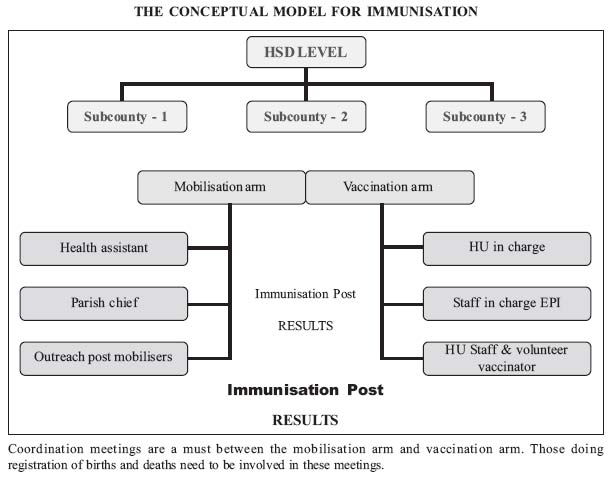
The results of the innovations The implementation of the strategy above gave Maracha HSD a chance to recover from poor performance in vaccination coverage. The graphs below show how the monthly EPI returns changed with the adoption of this approach to mobilisation for vaccination from February 2004. The monthly vaccinations in the HSD increased to more than 600 doses per month, from a monthly average of less than 400 previously. (Note that there was general lack of vaccines and non release of funds in the district whose effects appeared in the lowest vaccination returns for October 2003 in Graph 1). This was meant to pilot the immunisation outreach mobilisation model at HSD level. We now know that it worked from the results we obtained in the last year, and by the willingness of the sub-counties to participate in its implementation. The graphs below show the trends of cumulative performance of DPT3, BCG and Measles against the set HSD targets (80% line) and against total coverage of the whole population of children below 1 year (100% line) for the financial year 2003/2004. It is observable that all the indicators changed from February 2004, the month in which the decision was taken to adopt the new multi-sectoral mobilisation model. (Graph 2) (Graph 3) Within 4 months of the strategy, the HSD DPT3 coverage moved from 36% to 73.1% (5,388/7368). Left without any intervention the HSD would not have achieved more than 57%, projecting from the trend between September and February. (Graph 4) The HSD achieved 72.1% (5311/7368) measles coverage. Without any intervention the target population coverage would have been about 60%, projecting from the trend set between September and February. Although the BCG coverage was already progressing very well without any intervention, the intervention improved the coverage further. As a HSD bordering the Democratic Republic of Congo, although coverage of over 100% could be explained by immunisation of children from across the border, we tend to believe that we reduced on the missed opportunities for children within in the HSD since no mobilisation was conducted in the Congo. Discussion Comparison of the results in Maracha HSD with those from the rest of the HSDs in Arua District will help in understanding the difference made by the intervention. Graph 5 suggests that the performance of Maracha HSD was going to be similar to or worse than that of Ayivu HSD if no action was taken. The intervention made the HSD vaccinate the second largest number of children in the district, in absolute terms. The lesson learnt is that routinely collected data is still useful in decision-making. The monthly returns from the more populous HSDs would be expected to be bigger but the graph shows that this was not the case. For instance Arua Municipal Council (AMC) HSD which has the smallest population was vaccinating the highest number of children. This could be due to higher awareness and relative ease of access in urban areas. It could also be due to the fact that the urban populations in AMC and Koboko seek immunisation at static points as opposed to the rural populations that have to be reached by outreaches. Although comparison of absolute numbers of children vaccinated as above would appear unscientific as the HSDs have different population sizes and therefore different numbers of under-ones, the purpose of this graph is to show trends of the returns. Whereas all the HSDs have fairly straight courses, Maracha HSD had an upward curve coinciding with the start of this mobilisation strategy. Access to health services in the rural areas therefore seems to hinge on the strength of the system than on the will of the people. This seems to be supported by the fact that when there was a shortage of funds in the months of September and October 2003, there was a nosedive in the coverage rates. Given that most of the population leave in rural areas, the outreaches need to be strengthened by adopting mobilisation strategies that are effective as well as guaranteeing the availability of the necessary resource inputs. Health care management structures from the HSD and below are increasingly difficult to manage. This could be explained by the fact that the lower one goes, the more the comprehension of the stakeholders on their roles seems to diminish. The working documents become vaguer and lack detail to guide health care managers at that level. They are deficient on the principles and specifics of operations at the community level. This could also explain the fact that, all along, little attention has been paid to mobilisation for immunisation despite the poor coverage in all the HSDs. The National Immunisation Days (NIDs) have taught us that the success of immunisation rests in mobilisation. During NIDs, the performance is usually above 100%. During routine immunisation, it slumps to less than 40%. The results presented here are an affirmation of the importance of mobilisation and need to be adopted and used to strengthen our systems further. The mobilisation structure needs to be an integral part of the sub county management system. The model adopted by Maracha HSD for EPI mobilisation for vaccination could be summarised as below: (Model) Operation of the model in Maracha HSD The mobilisation strategies for immunisation seem to vary from one HSD to another. Usually, health workers take all the blame for poor immunisation coverage. The local governments need to know the role they are to play in health service delivery. The model above attempts to clarify the roles of the different stakeholders, for more efficient mobilisation for vaccination and, indeed, uptake of any community level intervention. 1. Mobilisation; This is the responsibility of the sub-counties. The Health committees and the executive of Local councils still need to be trained to monitor the performance of vaccination activities. The results will be publicly displayed to stimulate competition by parish and among the sub-counties in the HSD. Quarterly evaluation meetings are encouraged and this is also an occasion for discussing other health related issues e.g. Family planning, clean and safe deliveries etc. 2. Vaccination This should be the responsibility of the health workers. The number of health workers in the health facilities is very few; therefore there is the need to boost their numbers with volunteer vaccinators. Indeed, two of the health centres in the HSD have only one trained health worker each. These volunteers should be selected by the communities on the basis of socially accepted criteria and the level of education. The module for training nursing assistants in EPI will be used. 3. Cold Chain and logistics management This remains the responsibility of the health units, Health Sub District, and District Directorate of Health Services. 4. The health assistant at sub county level The health assistants have the responsibility to coordinate the out reaches to the posts in the sub county. For every post, the parish chief and the two post mobilisers mobilise the population on the outreach day. The health assistant links up with the health units to ensure that immunisation activities take place as planned. The mobilisers should be trained to work together with the teams for birth and death registration. They will keep registers of children in their area and monitor their status of immunisation before the day for immunisation. This will enable pro-active tracing of children who have defaulted once. 5. The EPI focal person Has the central responsibility to support and supervise the implementation, analyse the data for feedback of progress and advise on remedial measures to be taken. S/he has responsibility for the logistical support to the activities. Why do we need a mobilisation model? 1. For effectiveness An effective immunisation model should be able to reach the targeted children as measured by good immunisation coverage. The numbers of children immunised per month went above 600 as soon as the model was introduced; achieving what you what to achieve. This means the approach guarantees access; one of the guiding principles of the health policy. 2. For efficiency To complete the circuit the model needs to be efficient. This means that the model should allow more children to be immunised at the same cost or the same numbers of children at a lower cost. Comparing the period before the adoption of the model (July-February)and after (February-June) the direct financial cost per out reach was 14,000/= and was increased to 22,000/= per out reach afterwards. (See the table below for details). The adoption of the model meant increasing the number of mobilisers by two E.g. health assistant and the parish chief became mobilisers too. This was an additional cost of 8,000/= per out reach (5,000/= for health assistant and 3000/= for the parish chief). The additional cost incurred paid off in that more children were vaccinated in the period February- June (2,947). The results above show that despite this increase in cost per out reach it became cheaper to immunise one child (1,583/=): this defines efficiency; doing the same thing with less resources. The cost per child immunised reduced by 35% following the adoption of the model. This 35% reduction is the efficiency gain due to change of approach. The lesson learned is that money spent on mobilisation is not money wasted. In some districts in Uganda mobilisers are not budgeted for under PHC funds. Some HSDs in Arua use one mobiliser for a post yet most of the parishes are too large to be mobilised by one person. The money spent on the vaccination arm may end up being wasted if mobilisation is poor and children are not brought to the posts. Health worker costs are fixed. They will still be paid for having gone out of their duty stations, even if they waited for the children in vain. This is an absolute loss of money without service outputs. Immunisation performance can be influenced by external factors like delayed release of funds by the central government and bureaucracy in the district. This model was protected from this influence by making sure the finances for the following months were requested in advance. Difficult decisions had to be made to reach the end. No doubt some services had to be starved to make the funds available to EPI. For instance all activities of the HSD that were budgeted for but were not carried for one reason or another were used to finance this initiative since this was a decision taken in the middle of the financial year. This involved a strict and efficient financial management to ensure that money was only spend on outreach activities that could by verified through the outreach register. This is allocative efficiency 3. For Epidemic prevention/ control It is known that vaccines protect individuals who are immunised. It's also known that high immunisation coverage of the target population protects the community members who are not immunised (herd immunity). It is therefore desirable to have effective modules that can increase vaccination coverage. 4. To consolidate the elimination strategies for Polio, Measles and Maternal and Neonatal Tetanus. Mass immunisations are a common strategy adopted in refugee situations to prevent outbreaks of epidemics among the refugee populations. This is on the premises that the health systems in their countries have not been functioning due to war and mass movement patterns might have disrupted any herd immunity there was. At that time, it therefore makes sense to update the immunisation status of the vulnerable groups. It is also understandable that some diseases can be eliminated by mass immunisation of the population coupled with other interventions. E.g Polio, measles, small pox etc. This is especially so in countries where the routine immunisation system is not well established or ineffective and with poor immunisation coverage. The question is "When will mass immunisations stop?" What efforts are we making to improve our routine immunisation systems so that mass immunisations do not become the norm? These questions call for development of systems that are effective. It's time to strengthen our routine systems as more diseases get on the elimination agenda. In fact the algorithm for tetanus 'Elimination' declaration, among other parameters, depends on the coverage with Tetanus Toxoid. It is also important to note that the results achieved in mass immunisations are only sustained when the routine systems are doing well. Not only that; mass immunisation is very expensive and disrupts routine immunisation activities planned with the meagre resources at the HSD or unit level. For example, the money available for mass vaccinations (from training to implementation in weeks) is much more than what the HSDs can plan for, for routine immunisation for the whole financial year with the resources available to them. 5. To strengthen our health system for community health interventions This model can be adapted for any community level intervention. It gives the local governments their position in health service delivery. Conclusion It can be concluded that to attain and sustain vaccination coverage of children above 80% for all vaccines at an affordable cost to our health care system and resources, HSDs and the health centres have to work through and with sub-county administrations especially for mobilisation. Recommendations
Acknowledgements We would like to thank the staff of Maracha Hospital and the office of the DDHS Arua who helped me with collection and verification of data, proof-reading and encouragement at various stages: M/s Tiko Florence, Mr. Onzima Richard, Mr. Sunday Cadri'bo, Mr. Dramadri Sunday, Mr Alioni Joel, Mr Aloro Samuel, Mr Ayoma Alfred, Dr. Marina Anghileri , Dr Anguzu Patrick References
Copyright 2004 - Department of Health Sciences of Uganda Martyrs University |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}