 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 3, No. 1, April, 2005, pp. 1-11 TOPICAL ISSUE: HIV AND AIDS IMPACT OF VOLUNTARY COUNSELLING AND TESTING AND HEALTH EDUCATION ON HIV PREVENTION AMONG SECONDARY SCHOOL STUDENTS IN NORTHERN UGANDA Maria Grazia. Dente1, Massimo Fabiani1, Ronald Okwey2, Natalia Conestà1, Cyprian Opira2 and Silvia Declich1 1 National Centre for Epidemiology Surveillance and Health Promotion,
Istituto Superiore di Sanità,
Rome, Italy; 2St. Mary's Hospital Lacor, Gulu, Uganda. Code Number: hp05002 Abstract
The study aim was to evaluate the impact of Voluntary Counselling and Testing (VCT) and School Health Education (SHE) on HIV/AIDS related knowledge, behaviours and risk perception among secondary school students in Northern Uganda. A post-test only control group study was conducted among 1,312 secondary school students classified as follows: students involved in SHE and VCT (group 1); only in SHE (group 2); in neither VCT nor SHE (group 3, control group). Almost all students are aware of AIDS and condoms and how to prevent HIV infection: abstinence and condom use were the most reported preventive measures. About 60% of those in groups 2 and 3 were sexually active compared to 31% in group 1 (P<0.001). Students of group 3 had earlier sexual debut (median age=15) than those in group 2 (median age=16) (P<0.001). No significant differences in condom use with any type of partner were observed, although students in group 2 were more likely to report consistent condom use. Overall, two-third of the students say they do not feel they are at risk of infection, but almost 70% of them reported no reason. Despite considerable knowledge about AIDS, many students engage in unprotected sex and re thus at risk of infection . Students exposed to VCT and SHE seemed to have safer behaviour, suggesting that these programs should be expanded and further research should be conducted on the effects. SHE could be the appropriate method to reach youth and their families in poor-resources settings, whereas VCT could be the appropriate choice as part of a comprehensive service delivered to the users. Introduction More than twenty years into the pandemic, HIV/AIDS has continued to spread relentlessly in many areas of the world. However, in some countries of the developing world, where the HIV/AIDS epidemic has been present for more than 10 years and is now in its mature stage, stable or even declining HIV prevalence rates have been reported (Fylkesnes et al 2001, Kwesigabo et al 2000, Mbulaiteye et al 2002). Uganda is among the African countries where a severe HIV epidemic was first recognised. Between 1992 and 2001, a decrease in HIV prevalence rates was observed among pregnant women attending antenatal clinics, (STD/AIDS Control Programme 2002). Several studies have shown that this decrease, in Uganda as in other African countries, is largely due to the adoption of safer sexual behaviour (Asiimwe-Okiror et al 1997, Kilian et al 1999, Meda et al 1999, Bloom et al 2000, Stoneburner et al 2004 Changes in sexual behaviours could be explained by increased knowledge as a result of vigorous AIDS information campaigns carried out by government and non-governmental organizations or social "feed back" effects associated with witnessing the deaths of relatives or hearing from peers about such deaths in their own families, or other factors. The concept of personal risk or vulnerability, which underlies the theoretical and practical aspects of behaviour change programmes for HIV/AIDS prevention, deserve further study (Kengeya-Kayondo et al 1999). It should also be noted that the highest number of AIDS cases in Uganda are reported among young adults aged 25-29 years, who were probably infected when teenagers (STD/AIDS Control Programme 2002). Schools represent a potentially effective vehicle for delivering HIV prevention programmes, allowing direct access to adolescents, as well as the involvement of teachers, nurses and counsellors. It is urgent to identify the most effective ways to ensure not only increased knowledge but also the adoption of safer behaviours for both girls and boys in different social and economic circumstances. Young people need to be more aware of both their own personal risk and of risky situations . In particular, young women need communication and negotiation skills to discuss sexual and other AIDS-related issues with their partners (Karim et al 1995, Voluntary HIV-1 Counselling and Testing Efficacy Study Group 2000). This study is aimed at evaluating the impact of Voluntary Counselling and Testing (VCT) and School Health Education (SHE) on HIV/AIDS related knowledge, risk behaviours and risk perception among secondary school students in Northern Uganda. Materials and methods Study design, participants and data collection
A quasi-experimental design was selected in order to measure the effect of two interventions: in particular, a post-test only control group study (Campbell et al 1963) was conducted in the period June-September 2000 in the framework of the programme "Global Support to the National Plan for HIV/AIDS Control in Uganda", which has been implemented since 1994 at St. Mary's Hospital Lacor (Gulu District) by the Italian National Institute of Health (ISS). The study was conducted among 1,312 students attending the third and fourth years (S3 and S4) of 22 secondary schools in the Gulu municipality and surrounding areas and classified according to their receiving VCT and SHE (group 1), only SHE (group 2), or neither VCT nor SHE (group 3, control group). The 432 students of group 1 were those attending the four secondary schools of Gulu municipality involved in an open cohort study during the survey. The students enrolled in the cohort study, which began in 1994 with the aims of evaluating HIV prevalence, incidence and related risk factors, received VCT services (HIV test with pre and post-test counselling) at enrolment and at two follow-up visits, which were conducted approximately every six months. The students involved in the cohort study also received regular SHE on HIV/AIDS. Starting from 1997, SHE was extended to the 10 other secondary schools in Gulu municipality and surrounding areas (within 6 km from Gulu town). The 431 students in group 2 were attending 9 of these municipality schools (one school was closed at the time of the study.) The direct target group of the SHE programme is school teachers. They are trained and supported, in collaboration with the National Teacher Training Programme, both to deliver HIV/AIDS health education sessions to their students and to incorporate health education in the school's curricula. The SHE programme has also organised activities with the direct participation of the students (two one-hour health education sessions and one school art competition with drama, poetry and posters during each year of the project) and provided teaching aids. Finally, the 449 students of group 3, used as a control group for this evaluation study, were those attending nine schools involved in neither VCT nor SHE programme, which were selected because they were similar to the schools attended by the students of group 1 and group 2 with respect to location (all within 6 km of Gulu town) and type of schools (almost all were gender-mixed, non-vocational schools, and there was a similar balance between private and governmental schools). A questionnaire focusing on knowledge of HIV/AIDS, sexual behaviours and knowledge and access to condoms was first self-administered to students of group 1 in June-July 2000. Successively, the questionnaire was expanded with questions related to risk perception and self-administered to students of group 2 and group 3 in September 2000. The questionnaires were pre-tested before starting data-collection and some critical questions were carefully evaluated in order to ensure students would understand them in the local context. Data were collected anonymously, to ensure confidentiality, and consent and ethical approvals for the study were obtained from the schools' headmasters and from the District Education Officer. Statistical analysis
We have analysed the distributions of the main socio-demographic characteristics by study group and evaluated the estimated differences using the chi-square test. The distributions of categorical variables related to HIV/ AIDS related knowledge, risk perception, behaviours and attitudes by study groups were reported and the differences evaluated in multivariate analysis by applying the Wald test to the parameters estimated through logistic regression models. The multivariate models were run controlling for the potential confounding effect due to gender, age, living place (i.e. school versus parents or others) and, only for the analysis concerning condom knowledge and access, also controlling for being sexually active. For each variable with more than two categories we have calculated the adjusted odds ratio (AOR) for the category "misconception" with respect to all the other categories combined, always considering the study group as an independent variable in the models and assuming students with neither VCT nor SHE as reference group for AORs. Finally, median values and interquartile ranges (IQR) were used to describe the differences among the study groups with respect to continuous variables, and these differences were evaluated using the non-parametric test H of Kruskal-Wallis. Results
Among the 1,528 students attending S3 and S4 at the 22 schools included in the study, 1,312 (85.9%) were present at school the day of the interview and filled in the questionnaire. No significant differences in inclusion rates were observed among the three study groups. Demographic characteristics
Although all the students included in the study were attending S3 or S4, students of group 1 were significantly younger than those of the other two groups (P<0.001). In fact, 64.1% of students in group 1 were aged less than 18 years compared to 48.0% and 42.9% of students in group 2 and group 3, respectively (Table 1). The gender distribution also shows significant differences among the three groups (P<0.001), females accounting for 64.1% of the students in group 1 and 50.2% and 34.9% of the students in group 2 and group 3, respectively. Most of the students of group 1 attended full-board schools (82.4%) compared to 13.7% and 29.6% of students of group 2 and group 3, respectively (P<0.001). No significant differences in the history of parents dead for AIDS were observed between students of group 2 (6.1%) and group 3 (4.0%), among whom this information was collected. Given the significant differences in age, gender and living place distributions, all the differences in knowledge, behaviours, risk perception and attitudes among the three study groups have been evaluated controlling for the potential confounding effect due to these demographic factors. HIV/AIDS related knowledge
In all the three groups, almost all the students have heard about HIV/AIDS, mainly at school but also at home and other places, and reported sexual intercourse as the principal way of HIV transmission. Abstinence was reported as the most important way of HIV prevention more frequently by students of group 1 (46.9%; AOR=1.4, 95% CI: 1.0-2.0), whereas students of group 2 more frequently reported use of condom (51.2%; AOR=1.6, 95% CI: 1.2-2.1). Analysing data by gender, among students of group 1 and group 2, abstinence and faithfulness have been reported more frequently by females (78.0% and 40.2% in group 1 and group 2, respectively) than males (45.7% and 28.9% in group 1 and group 2, respectively), who, on the other hand, more frequently reported use of condom (50.7% and 59.2% in group 1 and group 2, respectively) than females (26.0% and 43.2% in group 1 and group 2, respectively). No significant differences by gender were observed among students of group 3. Sexual behaviour
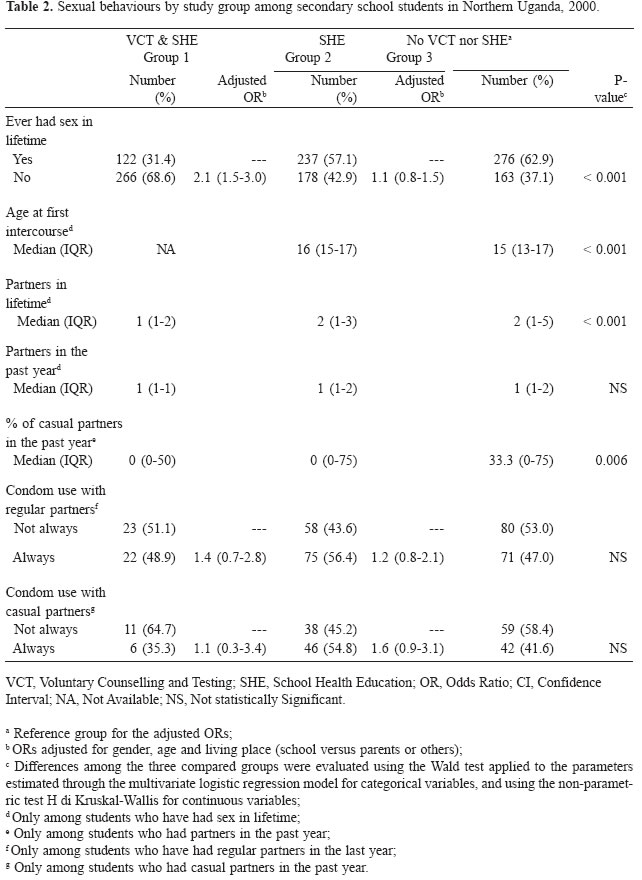
About 70% of the students in group 1 were not yet sexually active compared to about 40% of those in group 2 and group 3 (AOR=2.1, 95% CI: 1.5-3.0) (Table 2). Among sexually active students of group 2 and group 3, the former reported a significantly higher age at first intercourse (median=16 years, IQR: 1517) than the latter (median=15 years, IQR: 13-17). The median number of lifetime partners significantly differs among the three groups (P<0.001). Students of group 1 had had fewer partners than those of group 2 and 3. However, no significant differences were observed in the median number of partners in the past year, although among those who were recently sexually active, students of group 1 and group 2 were less likely to have had intercourse with casual partners than those of group 3 (P=0.006). No significant differences by gender in frequency of intercourse with casual partners were observed, with the exception of students of group 2 (P<0.001), among whom males were more likely to have had intercourse with casual partners (median=50.0%, IQR: 0-100) than females (median=0.0%, IQR: 0-50). No statistically significant differences in condom use with both regular and casual partners were observed among the three groups, although students in group 2 were more likely to report consistent condom use than students in group 1 and group 3. No significant differences in condom use by gender were observed in all the three groups. Condom knowledge and access
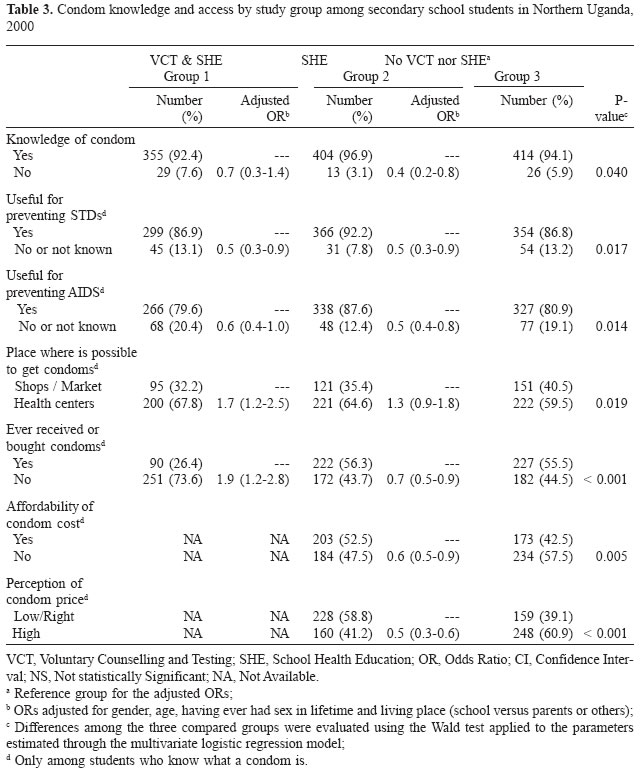
More than 90% of the students in all the three groups knew what a condom is and most of them knew that it is useful for preventing AIDS or other STDs (Table 3). Most students in all the three groups reported health centres as the most accessible place to get condoms, with a higher percentage among those of group 1 and group 2 (P=0.019). Although almost all students know where to get condoms, students of group 1 have more rarely done so (73.6%; AOR=1.9, 95% CI: 1.2-2.8) than those of group 2 (43.7%; AOR=0.7, 95% CI: 0.5-0.9) and group 3 (44.5%), and in all the three groups males obtained condoms more frequently than females (54.2% versus 9.0% in group 1, 70.4% versus 40.9% in group 2 and 66.8% versus 31.7% in group 3). Students of group 2 reported condoms as too expensive (47.5%; AOR=0.6, 95% CI: 0.5-0.9) less frequently than those of group 3 (57.5%) and, as a consequence, also considered its price as high (41.2%; AOR=0.5, 95% CI: 0.3-0.6) less frequently than those of group 2 (60.9%). Risk perception and preventive behaviours in risk contexts
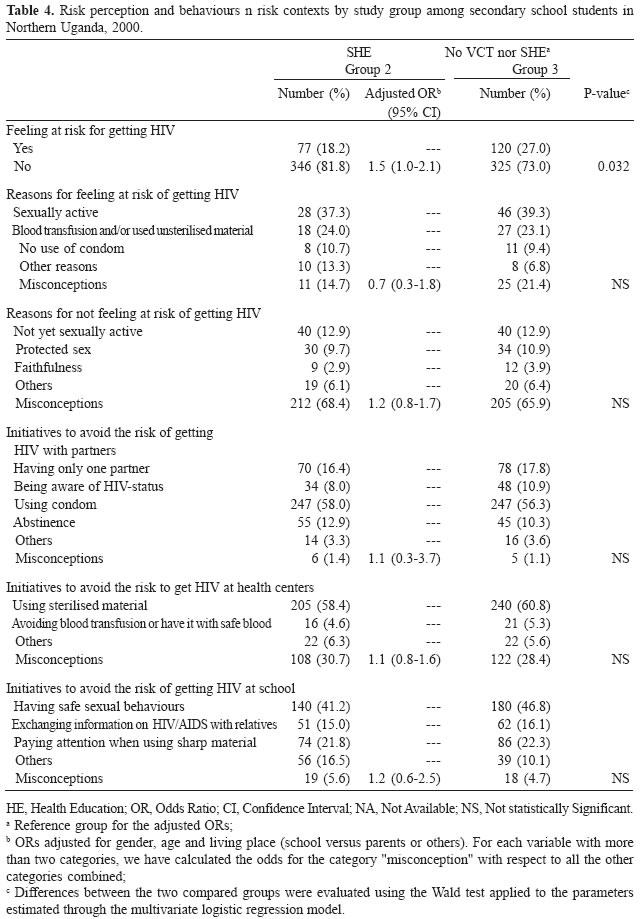
The analysis presented in this section, which was conducted only among students of group 2 and group 3, shows that 81.8% of students in group 2 (AOR=1.5, 95% CI: 1.0-2.1) do not feel at risk for getting HIV compared with 73.0% of students in group 3. There was no difference by gender in either group (Table 4). However, both students of group 2 (68.4%) and students of group 3 (65.9%) reported misconceptions, suggesting that their concepts of risk perception are incorrect. The most frequently reported plausible reasons for not feeling at risk included being not yet sexually active (12.9% in both groups) and having protected sex (9.7% in group 2 and 10.9% in group 3) , the former mainly reported by females (19.9% and 14.2% in group 2 and group 3, respectively) and the latter by males (10.3% and 13.3% in group 2 and group 3, respectively). Among students of group 2, plausible reasons for feeling or not feeling at risk were more frequently reported by students who were not yet sexually active (47.5% compared with 37.3% among sexually active students). In both group 2 and group 3, students who had not consistently used condoms with regular partners in the past year reported plausible reasons for feeling or not feeling at risk more frequently than those who did not use condoms (34.6% versus 27.1% in group 2, and 52.0% versus 46.5% in group 3). Finally, no significant differences between the two groups were found analysing the risk-preventive behaviours listed in Table 4 in specific contexts (with partners, at health centre, and at school Discussion
In our study, all the secondary school students showed good knowledge of HIV/AIDS prevention and transmission, although it is not clear whether this knowledge was acquired through national AIDS campaigns, mass-media or health education. Even so, exposure to VCT and/or SHE does seem to be associated with avoidance of high-risk sexual behaviours (i.e. precocity in sexual debut and high number of casual partners) in this study. Although almost all students reported to know what a condom is and its usefulness in preventing AIDS, fewer than half of them use them consistently with casual partners. These findings show that among young people, as with other population groups, increasing knowledge does not necessarily lead to changes in risk behaviours (Donovan et al 2000). The fact that the students attending VCT and receiving SHE (group 1), as well as those receiving only SHE (group 2), reported less risky behaviour than students of the control group (group 3), might be because the latter did not have direct contact either with an educator or a counsellor. The face-to-face contact with trained staff (teachers, counsellors etc.) may facilitate behavioural changes and support constant adoption of safe behaviours, as shown in other studies (De Zoysa et al 1995, Sweat M et al 2000). As the ability of VCT alone to effect behaviour change is far from being proven, a supporting approach should be identified. Having good health education sessions at schools could be one of the tools to promote youth awareness and to facilitate further effective contacts with VCT services. It is possible that direct contact with counsellors might facilitate the adoption of preventive measures more suitable for a student in accordance with his/her specific actual situation, beliefs, power of negotiation etc. For example, lack of power in negotiating condom use with partners barriers in access to condoms could explains the fact that females involved in VCT and SHE or in SHE only were more likely to report abstinence and faithfulness than males (Adamu et al 2002). The fact that no differences by gender were observed in the control group provides further evidences that face-to-face contact with trained staff is able to facilitate the adoption of safe behaviours in accordance with gender differences presently determined by the local context but susceptible to modifications over time. National HIV/AIDS prevention campaigns or generic IEC usually promote abstinence and faithfulness; in addition information about condom use are often delivered although, in reality, the potential opportunity to use it is not equally gender distributed. In fact, it is more likely that men can freely decided to use or not to use condom, while this opportunity of choice is not always granted to women. If the educators or the counsellors are aware of scarce power of women in deciding for condom use with their partners, might consider to mainly promote abstinence and faithfulness during their face-to-face contacts with women. In addition the educators and the counsellors might better modulate the message to be delivered in accordance with the age, needs, perceptions, etc. of the "client". Finally, the local situation in terms of different power of negotiation between sex, perception about different ways of preventing HIV infection etc., might change during time and educators and counsellors might easily register these changes and consequently modulate their education and counselling messages. The discontinuation of condom use in risky situations (i.e. during intercourse with casual partners), reported by most of the students, might be due to several reasons. The erratic availability of condoms (even though in Uganda condoms are available in many health centres and shops) and condom affordability, (about half of the students involved in the study perceived the condom price as high) could be some of the reasons affecting the frequency of condom use. However, the above mentioned reasons almost certainly play only a minor role. As suggested by other studies (Donovan et al 2000, Sahlu 1999), we believe that the accurate perception of personal risk and risk context is vital to making lasting changes in behaviour. In our study, a high proportion of students (almost 80%) reported they didn't think they were at risk of HIV, even though half are sexually active, about one-third of those had sexual intercourses with casual partners in the past year, and of those less than half have always used condoms in those circumstances. This is most likely an underestimation of personal risk and reflects a reluctance to admit possible exposure to HIV (Donovan et al 2000). Findings from our study suggest the need to identify appropriate ways to enable youth to distinguish between risky situations when condoms or avoidance of sex altogether is necessary, and other situations, which should not be source of concern for them. In fact, the purpose of behavioural interventions is to prevent the disease and not simply behavioural changes for their own sake (Aral et al 1998). Furthermore, a conducive and supportive context should be created in order to encourage, rather than frustrate, the self-efficacy of youth (including women) in risk contexts (Sahlu et al 1999, Nshakira et al 2002, Tiendrebeogo et al 2002), and more effort should be made to implement sustainable control measures rather than simply raising awareness. The results from this study should be interpreted with caution. The absence of pre-intervention data does not guarantee that the study groups were similar before the program interventions began. However, no particular selection criteria were used in assigning the schools to VCT service or SHE programme, and the control schools were selected to have the same characteristics of the other schools. Although there were biases due to differences in gender, age and living place in the three groups were taken into account in the analysis. The validity of self-reported behaviours is questionable, especially for adolescents, and they might reflect intentions, desires or expectations, rather than actual behaviours (Asiimwe-Okiror et al 1997). Nevertheless, some studies have shown that reported sexual behaviours are correlated with biological indicators of sexually transmitted diseases and were also consistent over time in repeated surveys (Donovan et al 2000). Moreover, in our study, there was consistency among the data reported by the students (e.g., students reporting condom use as the main way for preventing HIV transmission were also more likely to report having bought, received or used them). To survey risk perception poses additional problems, particularly in African settings, where separating personal risk from general risk is difficult, because the risk may be interpreted loosely as chance and seen as a possibility no matter how small. This disparity between lay and expert understanding of risk, already pointed out in other studies (Kengeya-Kayondo et al 1995, Donovan et al 2000, Adamu et al 2002), might be the reason for the high proportion of students reporting that they do not feel at risk for getting HIV and the high proportion of misconceptions reported as reasons for it. Several studies have speculated that VCT may promoting behavioural change (Voluntary HIV-1 Counselling and Testing Efficacy Study Group 2000, De Zoysa et al 1995, Sweat et al 2000), as well as the efficacy of SHE in increasing knowledge about HIV/ AIDS (Klepp et al 1994, Main et al 1994, Kinsman et al 1999). Some, but by no means all recent studies have also suggested that SHE might facilitate behavioural changes as well (Fawole et al 1999, Shuey 1999), Findings from our study seem to support this conclusion, even though it is difficult to evaluate the extent to which these behavioural changes have been caused by VCT and/or SHE or have been caused by other factors, such as the feed-back effects of social changes. In our study, students who had lost one or both parents to AIDS were more likely to report accurate perceptions of risk, but this was observed only among orphans who received SHE and not among those of the control group, thus suggesting that SHE was able to improve the impact of the social effects on risk perception. In conclusion, VCT services and SHE may be effective ways to promote safe behaviours among youth. Comparing the cost-effectiveness of the two methods and considering some barriers to VCT in the developing world (UNAIDS 1999), we believe that, well conceived SHE programmes that are implemented by trained teachers and supported with community-based activities, could be an appropriate way to reach youth and their families in poor- areas, and VCT should be part of a comprehensive community service (Kasule et al 1997, Abraham et al 1995, Kinsman et al. 2001, Kio-Olayinka 2002). Acknowledgements
We would like to thank the staff and students of the School for Health Assistant Educator at St. Mary's Hospital Lacor, who were involved in all the steps of the study design and implementation. We would also like to thank Alessia Ranghiasci, Alessandro Di Vincenzo, Proscovia Akello, Christine Akongo, Paolo Francesconi and Adrian Gauci for their helpful contribute to the preparation of this manuscript. References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University
The following images related to this document are available:Photo images[hp05002t4.jpg] [hp05002t3.jpg] [hp05002t1.jpg] [hp05002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}