 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 3, No. 1, April, 2005, pp. 28-31 EVALUATING HIV TESTING ALGORITHMS FOR RESEARCH, DIAGNOSIS AND SURVEILLANCE Massimo Fabiani1, Barbara Nattabi2, Benon Biryahwaho3, Jacob Ouma2, Antonella Ninci2 and Silvia Declich1 1National Centre for Epidemiology, Surveillance and Health Promotion, Istituto Superiore di Sanità, Rome, Italy, 2St. Mary's Hospital Lacor, Gulu, Uganda, 3Laboratory for HIV Reference & Quality Assurance, Ministry of Health, Entebbe, Uganda. Code Number: hp05005 Abstract
The objective of the study was to evaluate the validity of the HIV testing algorithms used at St. Mary's Hospital Lacor (Gulu district, North Uganda) for research, diagnosis and surveillance. The validity of a new testing algorithm based on rapid tests for research and diagnosis was determined by testing 560 samples from the antenatal clinic at Lacor Hospital and using the old ELISA algorithm as a gold standard. The validity of a new testing algorithm for HIV surveillance, assuming the previously used Wellcozyme as a gold standard, was determined using 360 samples from the same antenatal clinic. Using the old ELISA algorithm as a gold standard, the new rapid test algorithm for diagnosis and research has a sensitivity of 90.6% and a specificity of 98.8%, yielding an accuracy rate in correctly classifying the results of 96.6%. In comparison to the Wellcozyme kit, the new testing algorithm for HIV surveillance has a sensitivity of 77.3% and a specificity of 96.8%, with no difference in the prevalence of HIV infection between the two testing schemes.The two testing algorithms evaluated in this study show good performances according to the purposes of their use. It is important that before full introduction of new HIV testing kits and algorithms into a setting, field evaluation studies are carried out to determine their validity. Introduction Testing for HIV infection has been carried out in St Mary's Hospital Lacor, Gulu, since 1993. It is carried out for diagnostic purposes, mainly as part of Voluntary Counselling and Testing (VCT), for HIV surveillance among antenatal attendees and for research purposes. Since 2000, HIV testing has also been provided for pregnant women attending the programme for the Prevention of Mother To Child Transmission (PMTCT). In recent years, the HIV testing process at Lacor Hospital has undergone two changes. First, as in many African health care settings, new diagnostic algorithms based on HIV rapid tests are increasingly used for VCT and other diagnostic purposes. Second, since HIV Wellcozyme ELISA kit used previously for HIV surveillance is no longer commercially available, a new testing algorithm has been used for this activity. This is the same utilised at national level, in accordance with indications by WHO/UNAIDS for HIV-surveillance in areas with prevalence less than 10% (WHO/UNAIDS, 1997). In comparison with the ELISA-based algorithms used in the past, when clients and patients would have to wait up to 3 weeks to receive their results, algorithms based on rapid tests provide test results in a relatively short time. This increases the proportion of patients who receive their results and learn their HIV serostatus, and optimises available resources because it requires little equipment and can be performed on single samples (Respess et al., 2001). However, the diagnostic performance of rapid testing needs to be evaluated in field conditions before it can be considered for diagnostic and research purposes. The performance of the new testing algorithm for HIV surveillance also needs to be evaluated before considering it as a valid alternative to the nowdiscontinued Wellcozyme ELISA kit formerly used for HIV surveillance. In recent years, several studies aimed at evaluating the performance of different HIV diagnostic kits and algorithms have been jointly conducted by the Italian Istituto Superiore di Sanità, the Uganda Laboratory for HIV Reference & Quality Assurance and the Laboratory of Serology of the St. Mary's Hospital, Lacor. The main objective of these studies has been to evaluate the validity of new HIV testing algorithms in order to identify the most reliable and affordable strategy to obtain valid results for research, diagnosis and surveillance. Materials and methods
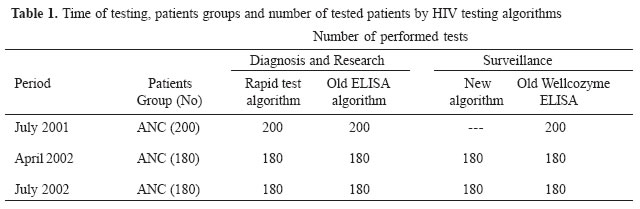
Between July 2001 and September 2002, a total of 560 serum samples collected from the Lacor Hospital's antenatal clinic (ANC) were anonymously tested for the presence of HIV-1 infection with different HIV testing algorithms (Table 1). Left-over sera from the routine syphilis test were used for HIV testing after having removed any identifier. In the old ELISA algorithm used for diagnosis and research all samples testing positive with Wellcozyme HIV-1 EIA were re-tested with the Recombigen HIV- 1/HIV-2 EIA and those testing negative - i.e., when there was a discrepancy between the results of the first two tests -were finally tested with Western Blot. The rapid test algorithm requires that all samples testing positive with Capillus are re-tested with the Serocard rapid test and those testing negative finally tested with the Multispot rapid test. We evaluated the validity of the rapid test algorithm for diagnostic and research purposes by comparing its performance with those of the old ELISA-based algorithm, assumed as gold standard, on 560 samples from the ANC. Until 2001, serum samples selected for HIV surveillance were tested with the Wellcozyme ELISA kit only. The new algorithm for HIV surveillance requires that all samples testing positive with Murex HIV 1.2.0 EIA are re-tested with the Recombigen HIV-1/HIV-2 EIA and those testing negative are finally tested with the SD Bioline rapid test. The validity of the new algorithm for HIV surveillance have been evaluated by comparing its performances with that of the Wellcozyme ELISA test, assumed as a gold standard, on 360 ANC samples. Sensitivity, specificity, positive and negative predictive values, accuracy (percentage of samples correctly classified as positive or negative) and differences in prevalence estimates have been used to evaluate the validity of the newly introduced testing algorithms. Results
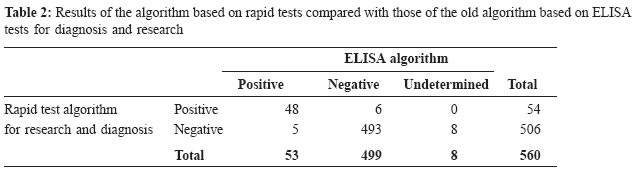
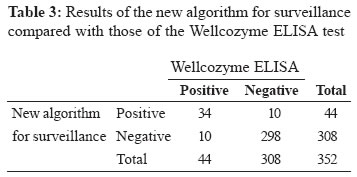
Table 2 shows the comparison between the old ELISA and the new rapid test HIV algorithms used for research, VCT and other diagnostic purposes. The HIV prevalence according to the ELISA algorithm is 9.6% [95% confidence interval (CI): 7.3-12.4] and the HIV prevalence according to the rapid test algorithm is exactly the same [9.6% (95% CI: 7.3-12.4)], with a relative difference of 0.0%. Using the ELISA algorithm as a gold standard, the sensitivity of the rapid test algorithm is 90.6% (95% CI: 78.6-96.5) and its specificity is 98.8% (95% CI: 97.3-99.5). The positive predictive value is 88.9% (95% CI: 76.7-95.4) and the negative predictive value is 99.0% (95% CI: 97.5-99.6). The accuracy in correctly classifying the results is 96.6% (95% CI: 94.8-97.9). The comparison between Wellcozyme ELISA and the new testing algorithm used for HIV surveillance purposes is summarized in table 3. The HIV prevalence according to the Wellcozyme ELISA was 12.5% (95% CI: 9.2-16.4), and the HIV prevalence according to the new algorithm was 12.5% (95% CI: 9.2-16.4), with a relative difference of 0.0%. The sensitivity was 77.3% (95% CI: 61.8-88.0), the specificity was 96.8% (95% CI: 93.9-98.3), the positive predictive value was 77.3% (95% CI: 61.8-88.0) and the negative predictive value was 96.8% (95% CI: 93.9-98.3). The accuracy in correctly classifying the results was 94.3% (95% CI: 91.4-96.5). Discussion The rapid test algorithm versus the ELISA algorithm provides valid results when samples tested as undetermined with the ELISA algorithm (gold standard) are excluded from the calculation of sensitivity, specificity and positive and negative predictive values. The accuracy of the rapid test algorithm is about 97% in correctly classifying the samples. As shown in other studies, HIV testing based on rapid tests is able to increase the proportion of individuals receiving their HIV test results, so improving the performances of programmes aimed at promoting VCT and access to PMTCT programmes (Malonza et al., 2003; Kassler et al., 1998; McKenna et al., 1997). The rapid test algorithm provides a good alternative to the ELISA algorithm because it is possible to process a small number of tests at a time and to obtain HIV results is a short time. Rapid tests are also easier to use than ELISA kits, which require training, power supply, and more elaborate equipment like microplate readers. Thus the HIV testing algorithm based on rapid tests performed well compared to the ELISA-based algorithm, suggesting that it could be used for both diagnostic and research purposes in this setting. In our knowledge, there are no other studies that have evaluated the performance of the specific HIV testing algorithm considered in our study. However, several field studies have shown that rapid test kits and algorithms are valuable methods for HIV testing, especially in resource-constrained settings, where the access to laboratory infrastructures and trained laboratory staff is limited (Rouet et al., 2004; Phili et al., 2002; Kassler et al., 1998; Andersson et al., 1997). The new algorithm used for HIV surveillance since the year 2002, which is mainly based on ELISA tests, yielded a prevalence estimate that is identical to that obtained with the Wellcozyme test alone. Although the sensitivity of the new algorithm is only 77.3%, thus making it as no appropriate for diagnostic purposes, this does not affect the prevalence estimate, which is the outcome measure of interest of HIV surveillance. In general, using ELISA tests for HIV surveillance is more convenient than using rapid tests when the local infrastructures allows for it. This is mainly because testing with the ELISA-system is less time-consuming than testing with rapid tests when, as usually happens for HIV surveillance, a high number of samples are processed at the same time. Furthermore, the advantage of having the test results available few hours after blood drawing has not a sense in this context, where testing is usually anonymous and test results are not returned to clients. In conclusion, as this and other studies show and as recommended by UNAIDS/WHO, it is important to have field evaluations of different kits and algorithms (Aghokeng et al., 2004; WHO/UNAIDS, 2001). This makes it possible to determine the most reliable and affordable testing strategies for the context into which the kits are introduced. References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp05005t1.jpg] [hp05005t3.jpg] [hp05005t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}