 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
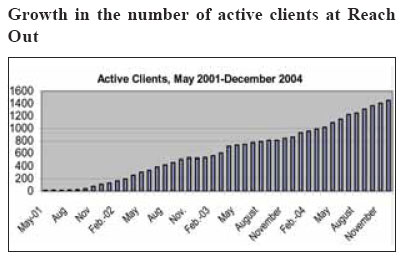
Health Policy and Development Journal, Vol. 3, No. 1, April, 2005, pp. 32-40 REACH OUT - MBUYA PARISH HIV/AIDS INITIATIVE Kamunvi Eric Community Network Coordinator, Reach Out, Mbuya Code Number: hp05006 Abstract Reach Out - Mbuya Parish HIV/AIDS Initiative (Reach Out) is a project under the Catholic parish of Our Lady of Africa Church, Mbuya, Kampala. It was initiated in May 2001 by a physician working in collaboration with the parish priest. The parish is divided into sub-parishes, which are in turn divided into Small Christian Communities (SCC). The operation started with three volunteers who catered to the needs of 14 clients living with HIV/AIDS. Reach Out experienced a rapid growth, and by February 2002, the number of clients served had increased to 109 persons. In response, a health clinic was established on the premises of the Mbuya Parish Church. The increased number of clients necessitated recruitment of staff to care for them. However, given the meagre resources available, the parish managers decided to recruit volunteers instead. The organization currently cares for over 1500 clients with a team of 230 volunteers, 77% of them clients themselves, delivering support through 11 different health and social programs. Introduction
Our mission of the outreach initiative is to curb the further spread of HIV infections in Mbuya Parish by informing all the parish residents about HIV/AIDS, and to enable those who are already living with HIV/AIDS to live a responsible, positive, and dignified life. Reach Out envisages that it will serve as a resource, sharing its knowledge and experience with other communities, in order to ensure that similar independent, community-owned programs are successfully proliferated. Our main objective is to provide free medical care, social, spiritual and emotional support to those living with HIV/AIDS in Mbuya Parish, with a special focus on those for whom such services are out of reach. Adopting a philosophy of holistic health care, the staff and volunteers of Reach Out believe that health service delivery does not end with drug prescription and supply. It must include efforts to break the vicious cycle of ill health and desolation, for we appreciate that medicine could be less helpful without food and food could be of no consequence when patients are not certain of a future. In turn, the future could look bleak when there is nothing to inspire the person to continue living - a hope. Reach Out strives to restore health in its entirety - physical, social, mental, spiritual and even socio-economic - defining each component as necessary in the delivery of the minimum health care package as defined in Uganda's Health Sector Strategic Plan (MOH, 1999). Below is a brief summary of the clients we were serving by December 2004. As mentioned earlier, we had 1,500 clients at the end of December 2004.
Health and Social Services
Reach Out has always recognized that people living with HIV/AIDS need hope and a sense of purpose to continue to live well. Accordingly, programs have been developed with the emotional, social, and economic well being of clients in mind. The Outpatient Clinic
Reach Out treats HIV/AIDS as a chronic disease, managed through regular check-up visits. This started as a mobile project that was treating clients in their homes. The clients to be treated were identified by community volunteers who were leaders in their Small Christian Communities. Each sub-parish was considered as one community, headed by a community coordinator known as a Central Volunteer (CV). The outpatient clinic started in February 2002 with 1.5 medical doctors and 11 volunteers. The 11 volunteers came up after the parish priest and the physician called upon the community for volunteers at the end of a service of Mass. The clinic was only open twice a week, on Mondays at the Mbuya Catholic Church and on Fridays at Banda Catholic Church centre for the satellite clinic. Later, the clinic days were increased to three and, more recently, to four. Currently, there are over 1,500 active clients enrolled in the medical support program. More than 500 clients are on free ARVs. Medical clinic days are currently four times a week, we provide over 500 scheduled consultations weekly and some not on appointment. The treatment provided to clients is free and open to all HIV-positive residents of Mbuya Parish, regardless of social status, religion or creed; but active program participation is required. Once a week, teams of medical staff conduct home-visits to see patients who are too weak to come to the clinic, and additional emergency visits are conducted as requested. This close follow-up is deemed necessary for clients to fully understand and adhere to their medical prescriptions, and thus obtain maximal benefit from their medical protocols. The many people testing HIV-positive have resulted in an increasing number of clients attending the clinic. All active clients are seen at least once a month unless for some special cases where appointments are given at intervals of less than four weeks. Clients are considered inactive and therefore discharged when they spend three consecutive months without coming to the clinic. Over 30 clients drop out of the program every month for various reasons. We have now started a program whereby community volunteers start following up all clients who miss two consecutive months to try and establish their whereabouts and their reasons for absenteeism. The medical program being the entry point for clients in Reach Out, this means that a client who falls out of it falls out of the all the other services. Clinic consultations have increased progressively since 2002. This could be attributed to the high need for and wish to access ART, since few health units around Mbuya Parish give free ART and quality care through the holistic approach. This has called for the accreditation of more ART centers and the initiation of the holistic approach to ARV distribution in all of them. Clients who are too weak to come to the clinic are advised to send a message so that they are seen by a health worker at their homes. They are visited frequently until they are strong enough to resume clinic visits. Five teams of clinicians, together with the community supervisors, conduct scheduled home visits once a week. In addition, emergency home visits are done as needed during the week. On average, outreach teams have been making around 50 home visits per month, but this number is decreasing progressively because more clients are getting on ART and resuming clinic visits on their own. Reach Out has grown very fast but at a steady speed in all its program aspects. However, the medical program, as the entry point for all clients, has grown fastest. We used the following principles in meeting the high demand of the medical services:
Counseling Section
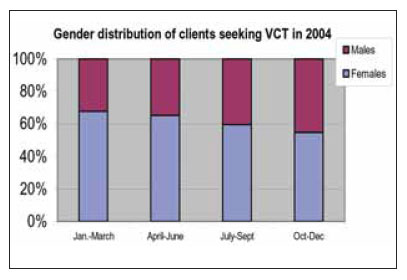
Reach Out offers free voluntary pre- and post-test counseling and HIV/AIDS testing (VCT) to all residents of Mbuya Parish. At the start of our programme, counseling was mainly done by the community volunteers and the doctors in the clients' homes. Then, all those who agreed to go for VCT were referred to neighboring VCT centers for testing and all their expenses on the exercise were paid by Reach Out. We also arranged the follow-up on all those who tested positive. On opening the clinic, professional counselors were recruited and they now work with the assistance of trained community counseling aides. At the beginning of 2004, onsite same-day-results voluntary counseling and testing was started. We instituted this because we observed that in 2003, only 83% of the 1,258 clients who received pre-test counseling actually went for testing. Of these as many as 24% of them, never came back for the results. Onsite testing has also helped us to ensure that the result is from the actual individual presenting it and not a falsification, presented by either unscrupulous individuals or needy persons simply trying to access other services of the programme. With the onsite same-day service, clients come for testing and counseling and if found positive, they are accompanied home by a community volunteer to locate their residence for easier follow-up in the future. In response to demands from the clients, the counseling section has increased its services to address other issues affecting members of the community including depression, alcoholism, drug abuse, domestic violence, and other problems that have devastating effects not only on our clients, but also on the other members of their families. We have conduct this counseling through the on-going counseling sessions and in focal clubs like the Post-Test Club, Alcoholic Anonymous, Couples' Club, Angels of Mbuya Choir and Club for the Adolescents. Whereas the majority of clients coming for VCT at are still women, in 2004 we registered a significant increase in the percentage of men coming for testing from 32.3% to 45.3 % of the clients. We attribute this increase to a number of factors. These include availability of free ARVs, visible effectiveness of the ARVs on other community members and higher community awareness about the entire programme following our community outreach program (Friends for Life). Others include the activities of the community network, the possibility of work opportunities within the programme (including micro-finance loans) as well as advocacy for testing by fellow men, whereby some of the male clients are particularly very active. Overall 56.2 % of all coming for testing were HIV+, showing little variation over the year as compared to 63% in 2003. These figures remain very high, considering that our active clients constitute 4.8% of the adult population of Mbuya Parish. Anti-Retroviral Treatment (ARV) Program
Reach Out launched its anti-retroviral treatment component in June of 2003, through a research program with the Joint Clinical Research Center (JCRC). In the first year, 85 clients were enrolled to receive free ARVs through the partnership with JCRC, and an additional 100 clients were supported through private funding. In March of 2004, funding was secured for 500 additional clients from the US President's Emergency Fund for AIDS Relief (PEPFAR) program through the Centers for Disease Control (CDC) of the US Government. To ensure optimal adherence and follow-up, our TB Treatment Program has been expanded into the Community ARV and TB Treatment Support Network (CATTS), which consists of trained clients who provide follow-up in the community, with coordination executed by the ARV Section based in the Reach Out clinic. Today we have over 550 clients on free ARVs and more are enrolled each day. The health of many of our clients on ARVs has improved and they are now able to support their families. The ARV department also handles our pregnant clients for PMTCT services. We started by referring all our pregnant clients to Mulago Hospital until we received funding from PEPFAR in March 2004. We had registered 49 expectant mothers by December 2004 but only one of them was already on ART. Criteria for starting ART at Reach Out
As most other organizations giving ART, Reach Out designed its own selection criteria for clients to start ART but primarily dependant on the clients' CD4 count with the lowest served first. The following 10 selection criteria are strictly followed to ensure close monitoring and to maintain good adherence:
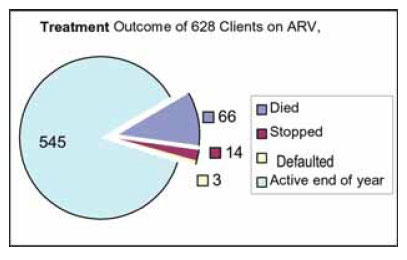
Those who fulfill the above criteria are then screened first by trained clinicians before counseling and starting them on ARVS. Clients receive individual and group counseling where family members or next of kin participate as well, hence the importance of a contract with a relative. All ART candidates are screened for TB with 3 sputum checks and a chest X-ray. Clients with CD4<100 are also screened for Cryptococcal meningitis. We check the Haemoglobin of all clients before starting the treatment. This whole process involves different departments, but with the high level of organisation and teamwork, it is very quick and not tiresome to the clients. Adherence is a very critical factor in provision of the Highly Active Anti-retroviral Therapy (HAART) that we offer. Non-adherence is the main cause of failure in HAART. Achieving optimal adherence is a lot more than simply instructing the patient to take the medication. On the first day of starting ARV the client is assigned a treatment supporter (Community ART and TB Treatment Supporter = CATTS), who lives in their neighborhood for they will walk home together and for the next six months they will be a team to ensure good adherence. We use three main tools for adherence control: first, the Pill Count, done at every visit to the clinic, second, the weekly reports from the CATTS, done after every home visit to the client and, third, the ARV register book. If any of these tools indicate a problem with taking the ARVs, we act immediately and address the issues causing difficulty in taking the drugs. A study of adherence was carried out among 319 clients, who were started on ARVs in 2004. Analysis based on pill count showed that 99.3% of clients were taking their drugs, 126 clients (41.7%) had 100% adherence to the correct dosage and that 5 clients had an adherence of less than 95%. Overall, individual adherence ranged between 90.4% - 100%. This has been made possible and sustained by many factors. These include thorough preparation in the clinic, counseling, continuous monitoring by the CATTS, close follow-up in the clinic, continuous counseling, home visits to clients who are too sick to attend clinic days, psychosocial support, material support with food, micro-finance support and provision of employment. ARVs have improved the lives of the clients and reduced on the death rate. Since we started the ARVs, out of the 628 clients who started the programme, the outcome has been as follows: Our challenge is to ensure that treatment will be continuously available, that it will be provided for all those who need it, that good adherence will be maintained and that once physical health is re-gained people will have a chance to live a good life with respect for themselves and with respect for others. Food Program
At Reach Out, we consider food and nutrition to be an integral part of successful medical treatment, particularly in supporting clients who are very weak or infected with TB. We provide food mainly provided by the World Food Program (WFP). We also receive some food from by private individual sources. In addition to solid food, we also provide milk for patients who cannot eat solid foods or to mothers under the PMTCT program. The food program at Reach Out started on a small scale with needy clients receiving a kilo of maize meal, beans or sugar depending on what was available. Later, in June 2002 WFP through AVSI started providing food to 250 clients mainly those on TB drugs. However, as the number of clients increased, the demand of food also increased. Therefore, in November 2004, Reach Out became an Independent Implementing Partner of WFP. We are now distributing WFP-supplied food commodities to over 1,013 PLWHAs and TB and more than 5,000 of their family members from just 680 clients in 2003. These commodities include maize meal, pulses, CSB, and vegetable oil. We provide the food monthly according to the family size of the client. This expansion in activities led to an increased demand for staff and we increased the volunteers from 2 to 13, who manage the department. They include 10 food monitors who are clients themselves. At first food was received and distributed on the same day. However, this proved to be inconvenient to both the beneficiaries and the program, mainly due to late delivery of the food on the part of WFP until MAERSK, a transport company, donated two containers for food storage. Currently, the food is distributed in groups of family size; 1-5 persons and 5-10 persons, each on a different day at the Mbuya clinic and then one day for the clients of our satellite clinic. During the monthly meetings of all clients receiving food, we discuss the issue of dependency and hence encourage clients to engage in income-generating activities (IGAs) for food security. The importance of food for our clients is proven every day as we continue to get the good results of our medical program. Yoga
At Reach Out, we started Yoga at the beginning of 2002. The beauty of Yoga is the simplicity in promoting health and harmony to all the internal organs and ensuring a natural functioning of all the anatomical and physiological systems of the body including the immune system. It thereby builds stamina and improves on the body posture, much more than physical fitness classes. Each clinic day per week is supplemented with a yoga session conducted by a guest instructor or a community volunteer for 45-60 minutes. Clients are encouraged by the medical staff to participate in these sessions for symptom alleviation and relaxation. All the volunteers also start their day the clinic with a session of Yoga daily, followed by a song, prayer for peace and finally a good laugh to get the day off on a happy note. SOCIAL SUPPORT PROGRAMS Microfinance
In order to improve the social welfare of clients and volunteers, we started "Bread of Life", a micro-credit program through which we provide small loans for the development of small-scale businesses. The capital for the loans and grants program at the start was obtained through the sale of second hand goods donated to Reach Out on Sundays outside the church. These loans are used to start small businesses, expand existing businesses, or to address personal needs people may have regarding income generation. The program was started in 2002 as a way of creating employment for our clients. At that time, Reach Out was still a small organization with a limited number of clients. Since then the organization has seen rapid growth and volunteers too started to benefit from the loan program. Bread of Life has responded to this growth by increasing the number and size of loans while maintaining a philosophy of serving the very poor of our community. We have strived to keep interest rates low and have consistently sought ways to improve the sustainability of the program so that a maximum number of people might benefit through our services. By the end of 2004, over 650 clients and volunteers had received loans compared to 154 by the end of 2003. Growth of this nature has precipitated a need to change policies, increase staff and develop plans to ensure the success of the program. It has also considerably altered the financial outlay of Bread of Life. We lend out up to 4 million Ush ($2,285) every month and all loans are payable with a 10% interest as a way of sustaining the program. There is over 80% pay back rate. Bread of Life produced a Policy Manual that enables successful implementation of its activities and sharing of knowledge with other organizations. Until we become fully sustainable, new funds will still be necessary from friends. Bread of Life at a Glance - 2002 to 2004
Overall Financial Summary
Sewing workshop and vocational School
Reach Out started the Roses of Mbuya sewing workshop in September 2002 with 4 sewing machines and 12 ladies. Only one of the 12 was a trained seamstress and she was the main trainer at the workshop. The workshop grew with time and, as all the 12 became expert tailors, more sewing machines were donated. This enabled the workshop to expand to 60 ladies with 80 sewing machines. Currently, the Sewing Workshop employs 25 clients, many of whom have been trained as tailors by Reach Out volunteers. The majority of the ladies after acquiring the tailoring skills were loaned a sewing machine and encouraged to start their own businesses. When the workshop gets too much contract work, they outsource the work to these ladies. The workshop handles a lot of contractual work including making school uniforms, a wide range of clothes for women, men and children, including household and educational items. The workshop has made considerable progress towards the goal of becoming fully sustainable, and in the future, external funding will only be necessary for large investments. Vocational School
As the workshop was growing and improving the social lives of many of the tailors, many clients requested to join. So in order for the workshop to benefit more clients who are living a new life, a vocational training program as initiated in September 2004 with 8 ladies. The objective of the school is to expand benefits of the Roses initiative to a greater number of clients. The school will provide comprehensive tailoring skills to the unskilled clients of Reach Out enabling them to generate their own income as tailors after they graduate. The trainees have already started to produce items for the Roses shop as their skills develop. Operation School Fees (OSF) Department
Keeping the children in school reduces a child's vulnerability to HIV/AIDS, stimulates hope for the future both for the child and the parent, fights poverty and lessens the parents' worries. This program offers educational and scholastic support to the children of clients. It ensures that they have school uniforms, basic school supplies, and at least one hot meal a day. Reach Out has partnered with five primary schools and three secondary schools within Mbuya Parish to ensure that students receive high quality education. The majority of the beneficiaries are primary school pupils, with a few secondary school students who are also clients of the programme. All clients of Reach Out still in school automatically qualify for school fees support. The department started in 2001 with 69 pupils and today it as over 350 children in school (52% are girls). Because of the department's good follow-up of children, it is now also working with AVSI (an Italian NGO) in following up other orphans in the parish under the AVSI program. The unique thing with this department is that most of its funding is from private individuals, though Reach Out is also trying to mobilize funds for the department in a number of creative ways like sale of bead necklaces made of old magazines by our clients and sale of the Angels of Mbuya Christmas music CD-ROM. Adult Literacy and Health Education
More than 15 % of our clients are illiterate and 67% of all clients have education less or to level of Primary 7. Adult literacy is a new program in the project's activities which was started in March 2004 to help our people especially the clients learn how to express themselves in society, avoid being cheated in some areas, take their drugs well and live comfortably in the society. Since then, the number of learners has increased from 19 to 55 under ten trained facilitators, 2 of whom are professional teachers. The subjects taught include reading and writing (English), mathematics, Swahili and Health Education. The department has expanded and in September 2004, it opened a branch in Banda clinic with 12 learners under 3 facilitators. The idea is to decentralize the department's activities to all the communities where we operate so that it is more accessible to both clients and non-clients. Those who learn how to read and write will be encouraged to join the vocational school of the Roses of Mbuya for survival skills. The department has now set up a library for both its students and external readers. COMMUNITY PROGRAMS Community network of care
In preparation to distribute ARVs and TB drugs to all our clients who needed them, Reach Out gave birth to the Community Network of Care in March 2004. This network was started to handle the expanding ARV section and cater for our TB clients as the national TB program had approved us a distribution center. It was built on the already established and well functioning TB community supporters' program. We selected some cadres and formed the Community ARV and TB Treatment Supporters (CATTS), who got further training to enable them take on this task. The training takes 3 weeks and comprises of treatment support, supply and monitoring of ARVs and anti-TB treatment, counseling and home based care. After training each CATTS is assigned ten clients on ARV and/or TB treatment that they support and monitor in their homes. The CATTS have to visit their clients at least once a week, and provide reports at the weekly network meetings about the clients they visited so that complicated cases are discussed. This cadre works in the community where they provide support to all our clients that were to receive ARVs and TB drugs. They are the "on-the-ground activists" in a network which includes the Community Supervisors (community coordinators - one in each village), the ARV team and the overall medical team. The community network has four meetings per week - one per village where the weekly reports of the CATTS are submitted, problems reviewed and new ARV clients are assigned their individual CATTS. They also have a monthly general meeting for all the four networks where ideas are exchanged and new strategies developed. The network has trained 41 CATTS and 10 community supporters, all under the supervision of 5 community supervisors. The CATTS have proven themselves to be an incredible asset for successful ART. Each client started on ARVs will have a treatment supporter for at least the first 6 months. Today we have 38 trained CATTS taking care of 370 clients, 178 on ARVs, 75 on both ARV and TB medication and 117 on TB medication. As more people go on ARVs we shall expand the number of supporters as needed. In addition to the CATTS, the network also has 'community supporters', who are trained for one day in addition to the training they receive by the CATTS in the communities. They are there to assist the very weak clients who need extra support like cleaning, cooking, and bathing. They have proved to be wonderful especially with clients who live alone in the house when they become helpless. Because of the intimate contact between CATTS/ community supporter/ clients/clinic the community network is now also a key point for the social activities in the community as well as other social support programs such as Bread of Life and Operation School Fees. The people living in the community know the real situation on the ground and are in an excellent situation to counsel and find solutions. The social support department, now fully under the community network, gives grants, material support and psychosocial counseling to clients in poor destitute conditions. It is run now by the community supervisors, CATTS and a social worker as the team that does the household assessment and the home visits. Material support is in form of blankets, small mattresses, second hand clothes, and household items all donated by individuals and organizations. The social network of care was established in the community to improve the monitoring and response to the social needs of our clients. Each of the CATTS is assigned a specific zone in which they work as central volunteers coordinating all activities. After six months of weekly support and monitoring of clients on ARVs, all those who are really doing well and conversant with ARVs are graduated. So far 80, CATTS have been graduated. Community TB Program
TB is widespread amongst the poor in Mbuya, and is the most frequent and serious opportunistic infection observed amongst clients. Continuous screening and treatment for TB is extended to all new clients of the program. The TB program at Reach Out, supported by a network of TB Treatment Supporters, has achieved excellent results, with a success rate well above 90% for completion of treatment. In recognition of our quality work and follow up of clients, the National TB and Leprosy Program recognized Reach Out as a distribution center for TB drugs. In March 2004, we received our first direct consignment of TB drugs. Since the first consignment, we have treated a total of 464 clients as shown below:
The department is to striving to maintain its low default rate through monthly training for those clients who started TB medication and among clients started on TB treatment, as well as requesting clients started on TB treatment to bring a treatment supporter of their own preferably a relative for TB education. This is in order to have more people with TB knowledge in the communities, hence improving prevention too. Community Outreach
'Friends for Life' is the community outreach/mobilization program of the project that operates in Mbuya local schools and neighborhoods, focusing on sensitization about HIV/AIDS and developing life skills. It has an active community program involving youth, school dropouts and adults in the communities. Activities carried out by the program include workshops, participatory seminars, drama, games, songs and plays, gardening and training in other income generating activities. Today, activities are carried out in seven communities and thirteen schools. The three major areas of Friends for Life activities are school program, community program and youth groups. In the school program, schools are visited on a weekly basis, equipping students with life skills, good morals, and spiritual values. Children are helped on how to make self-made informed decisions. A total of 1,526 children have benefited. The community program has 12 community mobilizers who organize the seven community groups for health education, drama, self-help issues like gardening, etc. A total number of 1,056 adults (910 females and 146 males) have been reached. The youth groups were started after a behavior change seminar and a total of 617 youths are participating in the clubs. Program development and support Training
At the beginning, volunteering did not require any special qualifications apart from an interest to serve others. This enabled many young people and active parishioners to come up and volunteer at Reach Out. Many were students, others jobless and others school dropouts. These volunteers proved to be a great asset to the program as it was growing day by day. There was a lot of on-job training and skills development by learning from each other every time the team came together. As the training seemed to be a great inspiration for many volunteers, this caused the birth of the training department in Reach Out. The department ensures both external and internal training of volunteers, other NGOs and any other group that may be interested in what Reach Out does. Today the training department is very busy as many organizations are initiating the holistic approach Reach Out uses and the nurse-based approach we are using. Moreover it has to meet the needs of the increasing number of volunteers and external health workers who come up for training at Reach Out. Training remains our priority to ensure quality care and support. Moreover, training provides the volunteers with the valuable skills they can use wherever they are. Training materials
Currently, Reach Out has embarked on developing training materials that can be used by other organizations and individuals who would be interested in doing the kind of work done in Reach Out. This has been slow because we have been trying to develop independent programs but all under one holistic circle. Some of our publications include:
Students from universities in Uganda and abroad are welcome to conduct small-scale research as part of their requirements for a degree. Conclusion
Reach Out has worked hard to keep its low cost, holistic model. Wherever possible we use existing resources and facilities. We use the church for the clinic, we have no fancy offices or cars. We are therefore able to provide all the services described in this paper for an average cost of UGX 45,600 (US$ 24) per client per month. Our funding is from grants and many private donations, however the greatest source of Reach Out Mbuya's income and donations come from the over 230 volunteers who work so hard for so little financial reward. It is their hope, energy, and hard work that enable us to keep the costs low and the quality of service high. Over 77% of our volunteers are clients themselves and this makes them so much more effective as they help to educate and provide support and treatment for their fellow clients. Many of the volunteers could find much better paying positions elsewhere but have chosen to put their efforts into serving their sisters and brothers at Reach Out. It is their direct contributions of service that enable us to remain at the forefront of providing holistic treatment for persons living with HIV/AIDS. Reach Out - Mbuya Parish has seen a growth from 14 clients to 1,500 clients in less than 4 years, volunteers have increased from 3 to 230 in the same period. The community has taken ownership of Reach Out - and through the work carried out together within the community we are all benefiting. At the end of 2004 Reach Out made a calendar - the title is "A New Life" and the ongoing theme is "We have a second chance and that chance is now". In this calendar there is a testimony from a client or a volunteer as the weekly theme for reflection. We called our calendar a New Life - because this is exactly what we are experiencing these days: A New Life -not only for our clients, but for all of us at Reach Out. For further information please contact us at:
Reach Out - Mbuya parish HIV/AIDS Initiative Our Lady of Africa Church Box 6562, Kampala - Uganda E-mail: reachout@utlonline.co.ug or usdanes@utlonline.co.ug Phone: +256 41 222 630 or +256 71 259 899 Or check our website: www.reachoutmbuya.org References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp05006f3.jpg] [hp05006f2.jpg] [hp05006f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}