 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 3, No. 1, April, 2005, pp. 41-45 HIV/AIDS IN AN ESTABLISHED MARKET ECONOMY: THE CASE OF ITALY Vinicio Manfrin1, Marzia Franzetti2 1Infectious and Tropical Diseases Department, S. Bortolo Hospital - Vicenza
Italy Code Number: hp05007 Abstract At the beginning of the HIV/AIDS epidemic in Italy, needle sharing among Intravenous Drug Users (IVDUs) was the principal mechanism of transmission of HIV. After an initial burst of the epidemic, the incidence declined sharply but transmission continues to occur mainly via homo and heterosexual intercourse. A significant number of cases were reported in last year amongst the immigrant population. The Italian Government has responded aggressively to the epidemic: a special commission composed of relevant AIDS clinicians, researchers and persons from NGOs, was set up in 1987 to give technical advice to the Ministry of Health. The first recommendations of the commission were enacted into a law (135/1990) which represents the main frame of the fight against AIDS in Italy. Initially, effective treatment not available, care of AIDS patients mainly involved treating Opportunistic Infections. Innovative care systems (Day care and Hospice Treatment Services) were implemented. The availability since 1996 of highly active antiretroviral treatment changed the life expectancy and care needs of the HIV affected patients. Different priorities have since had to be met: compliance to the treatment, emergence of drug resistant virus strains, management of side effects and treatment of co-morbidities such as chronic Hepatitis C are now the main challenges to be tackled by caregivers. The main drawback of the fight against HIV/AIDS in Italy was the lack of an effective Health Education plan targeted to the reduction of HIV transmission through sexual intercourse. This fact, coupled with unrealistic hopes for the effectiveness of antiretroviral treatment, produced a second wave of the epidemic among the hetero- and homosexual populations that, though less severe than that involving IVDUs, is maintaining the HIV epidemic alive in Italy. The beginning of the Epidemic
The first case of AIDS in Italy was diagnosed in 1982 but most probably, the spread of HIV began, as in other developed countries, in the second half of the seventies. In Italy the epidemic was initially driven by intravenous drug users (IVDUs) through needle sharing; when HIV tests became available at the end of 1985, prevalence in various regions reflected the number of IVDUs resident in the area and their behaviour. Men who have sex with men (MSM) or homosexual men in Italy were part of the epidemic since the very beginning but, as in other southern European areas such as Spain and southern France, they did not represent the main component of the outbreak. From IVDUs, the epidemic spread to the female population via heterosexual exposure. A minority of AIDS cases were registered among blood product recipients: 337cases were reported in haemophiliac persons receiving clotting factors and 417 cases in blood transfusion recipients. In the first phase of the epidemic the proportion of immigrants was negligible, but this has changed. In recent years, up to 30% of new AIDS cases in Italy were immigrants. In recent years new HIV infections are principally due to sexual activities (both homosexual and heterosexual). This epidemiologic pattern bears many consequences. Most IVDUs are well known to the National Health System, where they receive various free services for rehabilitation, psychological support and substitute drugs. It was therefore very easy to reach the majority of the population at risk, provide them HIV counselling and testing and direct them to HIV treatment services. The availability of inexpensive safe injecting equipment was very effective in reducing the first wave of the epidemic. The most important negative consequence of the IVDUS epidemic, besides the impact on the drug users themselves, was that it gave the general population a false sense of security. Many people felt that if they were not drug addicts or MSM, then they were not at risk of infection. This generalized belief, supported also by some political leaders, exacerbated the stigma associated with the disease, and undermined prevention efforts for the general community. Epidemiology of HIV infection/AIDS in Italy
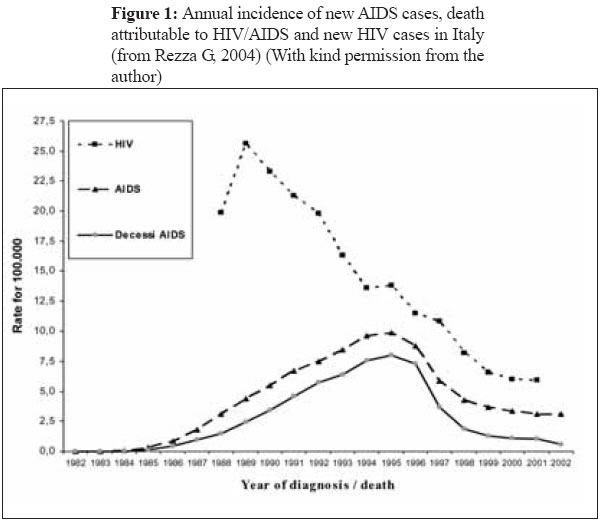
Data collection on HIV/AIDS cases began in Italy in 1982, with a surveillance system implemented in 1984; notification of AIDS cases has been mandatory since 1986. Data collection is carried out by the National Institute of Health (Istituto Superiore di Sanità - ISS) where a specific section for HIV/AIDS (Centro Operativo AIDS - COA) is active. Results of surveillance are frequently published and are publicly available (www.simi.iss.it/bollettini.htm). Trends in HIV incidence, AIDS cases and attributable mortality are given in figure 1. No HIV surveillance system is in place at the National level. However, some regions (Lazio, Veneto, Friuli) have implemented their own surveillance systems of newly diagnosed HIV patients; data from these systems represent about 20% of the expected burden of HIV in Italy (De P et al., 2003). Between 1982 and 2002, 51,172 AIDS cases were reported, and 33,308 people died of the disease (Commissione Nazionale Lotta AIDS, 2002). The majority of notified AIDS cases were men (77.8%) reflecting the large numbers of IVDUs and MSM in the epidemic. However, data suggest a decline in needle sharing as a factor in HIV transmission: IVDUs accounted for 70% of AIDS cases before 1993, but only 39.2% in 2001. A more pronounced trend is evident in the surveillance of new HIV cases: in the same period, IVDUs accounted respectively for 62.3% and 17.7% of all the cases, while sexual transmission (both MSM and heterosexual) went from 23.6% to 58.5% of total cases. AIDS and AIDS-related mortality peaked in the mid 90s. Since 1995, the curve dropped sharply as a result of the introduction of potent antiretroviral drugs. HIV incidence has been decreasing steadily since the beginning of the epidemic, although in the last few years a substantial flattening of the downward slope is evident. The spread of HIV in Italy is increasingly concentrated among immigrants. New HIV cases in immigrants rose from 8.8% in 1991 to 30% in 2000. Because IVDUS were the main group affected by the epidemic, a substantial part of the HIV positive population (though not the predominant one) was female. Many of these women were either partners of male IVDUs (roughly 40%) or IVDUs themselves (27%). One consequence of the fairly high number of females was a relatively high number of paediatric HIV cases, resulting from mother to child transmission. Since 1982, some 6.500 babies were born to HIV infected mothers in Italy. Of these, 1.310 (20.1%) contracted HIV and about 50% of them have so far developed AIDS (725 Paediatric AIDS cases reported between 1982 and 2002). As expected, many of these children were born in difficult circumstances. Many had parents who were IVDUs, or were severely ill or died because of AIDS; many families had economic problems too. For these reasons the Italian National Health system (mainly the paediatric services) had to address not only medical problems, but also social and psychological issues. The response of the Health System
In 1987 the National Commission for the Fight against AIDS was created by ministerial decree. Its members are medical personnel specialising in AIDS including scientists and AIDS NGO personnel. The main objective of the commission is to advise the Ministry of Health and the Government on relevant actions to fight AIDS. The first recommendations of the commission were accepted by parliament and were enacted into law N° 135 in 1990. The most relevant points of the law are: a) Care and treatment of AIDS patients was to be entirely delegated to the Infectious Diseases Department of the National Health System. As these units were considered insufficient in absolute number and staffing, a plan for upgrading existing facilities, creating new-ones and ensuring adequate staffing was developed. Funds for continuous training of all health personnel working with AIDS were earmarked. b) New and innovative treatment and support strategies were instituted to limit the need for hospital care (i.e. day care centres, hospices for indigent people, home care). c) Special attention was devoted to the rights of HIV patients, to avoid stigma and to preserve confidentiality. The basic principles of voluntary counselling and testing were introduced in the law and measures to eliminate discrimination in the work place, schools, sport activities etc were to be enforced. d) Health education was encouraged, but no specific and relevant guidelines or strategies were identified. The response of the civil society
Though some negative sentiments including denial, discrimination, stigma and fear were evident in part of the population, many actions in favour of HIV infected people were undertaken by individuals and groups. HIV infected patients established support groups to provide psychological and practical support among peers. Volunteers, including relatives and friends of HIV positive patients established non profit organizations to assist HIV patients in need and even collaborate with government institutions in home or hospice care programmes. A variety of different activities (theatre shows, school activities etc) were carried out around the country to raise awareness about HIV, to give prevention messages and to eradicate stigma and fear. Treatment and care
In Italy hospital care is free of charge for all Italian citizens and legal immigrants. Home or outpatient care is co-paid by users. However, HIV patients are exempted from any charge both for clinical investigations (laboratory tests, instrumental examinations, doctor consultations etc) and treatment. At the beginning of the epidemic, when no specific HIV treatment was available, the main aim of caregivers was to treat opportunistic infections, alleviate suffering and improve quality of life. The cost of care was quite high especially for the advanced stages of the disease, due to the high burden of hospital care. In the USA for example, care for each HIV positive patient was estimated to cost more than 135,000 USD over 8 years (Moore RD, Chaisson RE, 1997). The advent of anti-retroviral therapy, or HAART (Highly Active Anti Retroviral Treatment) in 1996 dramatically changed the outlook for people with HIV. The need for hospital care was reduced, and patients came to be seen as chronic patients, in need only of outpatient care. In the USA the death rate per 100 patient years fell from 23.4 in 1995 to 8.8 in 1998 (Palella FJ et al., 1998), while in a European study, which included data from Italy, mortality per 100 patient years fell from 23.5 in 1995 to 4.1 in 1997 (Mocroft A et al., 2003). The estimated risk of death of HIV patients fell by 64% between 1986 and 1998 (CASCADE Collaboration, 2003). Finally, HAART was also cost-effective. The price of regimens including a Protease Inhibitor (PI) is around 8.000 USD per year. In fact cost per quality adjusted year of life (QUALY) gained ranges between 13,000 to 23,000 USD and is in the range of other health interventions (table 1) [Reedberg KAF et al., 2001]. Table 1: Cost-effectiveness of selected medical interventions
Source: Modified from CASCADE Collaboration, 2003 Parent-to-child transmission
Before 1995, some 20% of children born to HIV positive mothers in western nations contracted the virus. Since then, the chances of transmission have been reduced to approximately 2% when the mother is treated with ARVs from the 12th week of gestation, an elective caesarean section is performed and newborns are treated with a combination drug regimen for 4 weeks (Coovadia H,, 2002). This extraordinary low probability of mother to child HIV transmission, combined with the increase in life expectancy and quality of life for HIV infected people, has brought about the need for special counselling and assistance for HIV positive women considering pregnancy. In recent years we also observed an increasing number of female immigrants from Eastern Europe, Africa and South America where HIV prevalence is higher than it is in Italy. Often, these women discover they are HIV positive during pregnancy or at delivery, when it is too late for them to receive the entire package of Prevention of Mother to Child Transmission interventions. Thus, most new paediatric HIV cases in Italy occur in the non-Italian infant population. HAART: the other side of the coin
HAART cannot cure HIV and patients on treatment may develop resistant strains of the virus that can hasten progression of the disease (Kulkosky J, Pomerantz RJ, 2002). Moreover, antiretroviral drugs can be toxic [9] and drug treatment, combined with other predisposing factors such as liver disease, can cause illness and even death (Fleischer R et al, 2004). Hepatitis C virus is prevalent in IVDUs. Hepatitis C is frequent in HIV positive IVDUs population (Tedaldi EM et al., 2003). Increased life expectancy in these patients (due to ART) leads to a greater risk of developing HCV-related liver cirrhosis. In a cohort of HIV infected patients enrolled in Switzerland, failure of treatment was common (Ledergerber B et al., 1999). Viral load rebound and/ or CD4 count decrease occurred in 27% of patients treated for the first time, and 58% of the people taking second or third line treatment. Clinical progression, meaning a new AIDS defining event, or death, occurred in 20% of the patients defined as laboratory failure subjects and in 7% of those whose lab tests suggested good response to treatment. Moreover, most of the patients on treatment harbour resistant virus; resistant strains were also found in many newly infected patients. Resistance limits the clinician's choice in selecting appropriate drug regimens, hampers the outcome of treatment and may have serious public health impact if the resistant strains spread. In Taiwan, availability of HAART contributed to the containment of the HIV epidemic (Fang CT et al, 2004); however, in Italy, as well as in other Emerging Economies (EMECs) of Europe, after a huge decline of incidence, a flattening of the slope is now evident. Recent epidemics of other STDs like Syphilis (Cusini M et al., 2004; Hopkins S et al., 2004; D'Souza G et al., 2003), Gonorrhoea (De P et al., 2003; Xia M et al, 2000), Lymphogranuloma Venereum (Nieuwenhuis RF et al., 2004) in the USA and Europe, suggest that safe or protected sex is less widely practiced than in the past. It is possible that, especially in some communities, the perception that ARVs are a "magic bullet", may have given some people a false sense of security. Conclusion
The HIV epidemic in Italy posed a great challenge to the National Health System. The response of the Italian Government was mainly in the curative field. Infectious diseases departments, identified as the Units in charge of assisting HIV patients, were empowered, properly staffed and equipped to fulfil their duty. New strategies including day care centres, hospice and home care programs were successfully implemented. The advent of HAART dramatically changed the outlook for HIV affected patients. New challenges include the management of the side effects of treatment and drug resistance. The health of HIV positive women is also an area of concern. However prevention programs have lagged behind. The initial decline in incidence was mainly due to the availability of inexpensive injecting material and the willingness of IVDUs to use it. This was principally the effect of the open market, rather than harm reduction programmes. Very little, if anything has been done to prevent sexual transmission of HIV, which is responsible for most new infections today. No specific education programme in schools, or via mass media has so far been implemented, except sporadic and controversial television spots. Moreover government officials and others have made statements which have increased stigma and created confusion about sexual transmission preventive strategies. Finally, media emphasis on medical advances, especially new drugs, may have contributed to a false sense of security which led to an increase in risky sexual behaviour. Recent epidemics of STDS in many emerging economies (EMECs) may foretell what we can expect for the HIV epidemic in the years to come. References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University
The following images related to this document are available:Photo images[hp05007f1.jpg] |
| |||||||||

{kind=link}