 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 3, No. 1, April, 2005, pp. 46-53 EMERGING THEME: HEALTH INFORMATION SYSTEMS DEVELOPMENT OF HMIS IN POOR COUNTRIES: UGANDA AS A CASE STUDY
Peter Kintu1, Miriam Nanyunja2, Amos Nzabanita3, Ruth Magoola3 1Axios Group; 2WHO Country Office for Uganda; 3Ministry of Health, Uganda Code Number: hp05008 Abstract Planning, monitoring and evaluation of healthcare programmes provides a strong foundation for the realisation of quality health service delivery systems. This involves regular collection, analysis and interpretation of health information to guide proper decision-making and design of appropriate interventions. Therefore, establishment of a robust management information system in any health program is crucial for the efficient delivery of health services to the population. The main challenges are in-patient data collection and processing, regular availability of HMIS tools, data utilisation, and electronic data management. Introduction
In Uganda, a health information system (HIS) was designed in 1985 to capture and analyse morbidity data for selected communicable and non-communicable diseases, and other services like immunization and family planning (MoH, 1985). Information was collected in the health facilities, summarized at the district level and later forwarded to the Ministry of Health at the centre where data analysis would be done. After 7 years of implementation, it was felt that the system was leaving out vital management information, such as staffing levels, infrastructure, health facility management, medical equipment availability, financial information and drug management. A review was therefore commissioned in 1992 with the aim of determining possibilities of collecting management information using the same channel. Based on findings and recommendations of this review, pilot-testing in 2 districts was done for one year and nationwide implementation of the Health Management Information System (HMIS) was initiated in January 1997 (MoH, 1997). The core function of the Uganda HMIS is to establish and maintain a comprehensive source of health and management information for planning, monitoring and evaluation of the health sector strategic plan. It focuses on improving and strengthening: a) Data collection and compilation of health events; b) Timeliness, completeness and accuracy of reported data; c) Analysis, interpretation and utilisation for evidence-based decision making and action; d) Regular dissemination and feedback to all stakeholders; and e) Enhancement of knowledge and skills of health workers in all aspects of data management, analysis and utilisation at all levels of service delivery. HMIS implementation in Uganda Development of HMIS tools
HMIS tools form the back-bone of the system. The 1997 model of Uganda HMIS was based on a multitude of paper tools (reporting forms, registers, databases and manuals), each containing a specific set of programme information (morbidity, family planning, immunisation, equipment inventory, drug availability, etc.). Health workers at the lower levels were supposed to record and compile separately a number of forms before forwarding to the centre. Data on deaths in health facilities and in-patient services was supposed to be compiled and reported on an annual basis. Due to the big number of forms and registers, health workers spent lots of time and effort on tallying and summarising the different data items, and the accuracy of the reports would be jeopardised in the process. The process was labour-intensive. Similarly, reports would take months to move from the health centres to the districts and finally to the several departments within the Ministry of Health. A review of the HMIS data collection and reporting tools was carried out during 2000-2001. Intensive discussions were held with the different stakeholders in order to come up with the crucial data variables for each programme. The main purpose for this review was to integrate the major aspects of the health and management information (data on out-patient morbidity, immunisation services, maternity statistics, drug stock monitoring, financial information, etc.) into one reporting form. This would reduce on the workload of records assistants who previously had to fill several forms, lessen compilation errors and improve on the consistency of the reporting system. This would further facilitate the smooth running of the central databank at the Ministry of Health since all data for the different programmes would be processed at one location. Among the developments was the introduction of a reporting tool for health facility-based mortality data which was now to be summarised on a monthly basis by all health facilities with in-patient services. This would enable assessment of case management and case fatality ratios, and development of appropriate interventions. During July 2001, a national dissemination workshop to launch the revised HMIS tools was organised. This workshop drew participants from the Ministry of Health and all the 56 districts of Uganda, including Directors of District Health Services, HMIS and surveillance focal persons. The revised tools (MoH, 2001) were then disseminated to all districts in Uganda. HMIS training
Support supervision from the centre, specifically focussing on HMIS, was strengthened at the district level and district programme managers were encouraged to facilitate this process at the health sub-district and lower level health facilities. Technical officers from the centre would visit the districts on a quarterly basis to support HMIS focal persons and records assistants with hands-on training on the HMIS and to practically sort out any problems encountered during the execution of the HMIS. Supervision reports showed improvements in HMIS implementation in a number of districts. However, some districts were reportedly lagging behind in terms of data analysis and utilisation, timeliness and completeness of reporting, and a focused training program was designed. This program was intended to strengthen the data management skills of health workers in order to improve on data analysis and utilisation of data for action at the point of collection, data quality and reporting. With support from WHO and other development partners, the training programme targeting operational-level health workers continues to be implemented in a number of districts and this is yielding positive results. A central HMIS team was constituted from the different front-line departments of the Ministry of Health (Epidemiological Surveillance Division, Health Databank/ Resource Centre, Uganda Virus Research Institute, Expanded Programme on Immunisation and Institute of Public Health). This team selects poorly performing districts and based on a standard curriculum covering all HMIS and data analysis aspects (MoH, 2001; Epidemiological Surveillance Division, 2003) trains core groups at district level composed of in-charges of health subdistricts and health facilities, records assistants, and District HMIS and surveillance focal persons. This district core group then passes on the HMIS improved skills and knowledge to operational-level health workers who are drawn from all health facilities at a formal practical training workshop and during follow-up. HMIS reporting mechanism
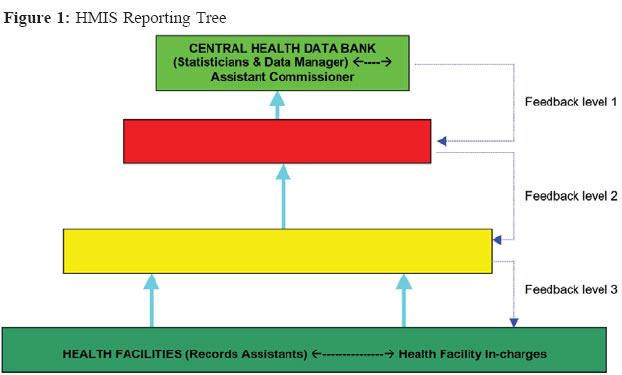
Reporting of HMIS data in Uganda is done through a network of 56 district health offices which collect and summarise health information from 214 health sub-districts and over 2,000 health facilities. These health facilities include government and private-not-for profit units which exist in the districts. Reporting from private practitioners has been very difficult as there has been no sustainable motivation for them to report and therefore information on the patients they administer is in most cases not included in the HMIS system. Summary reports for the districts are then submitted to the Ministry of Health where data is compiled to derive national figures on health and health management indicators (Resource Centre, 2001). A feedback mechanism exists whereby the central health databank provides summary analyses on a monthly basis to all districts, showing their comparative performance in terms of reporting (timeliness and completeness) and a selected list of health sector indicators. The districts with poor indicators are encouraged to review their service delivery strategies and reporting status. Districts are further encouraged to replicate this feedback to the lower health facilities and a format for this purpose has been designed and disseminated for use in all districts (Epidemiological Surveillance Division, 2003). Computerisation
Computerisation of the HMIS in Uganda has been a slow process due to financial and technical limitations. The central health databank at the Ministry of Health has been computerised using both MS-Access (19972001) and EpiInfo software (2002 to date). The current plan is to establish electronic data management and analysis at district and health sub-district levels, with a medium-term plan of setting up a district electronic reporting network capable of providing quick and accurate reports to the centre within all districts, and dissemination of prompt feedback to the districts. WHO carried out a computer inventory in 2001 and 70% of the districts were found to have computer equipment which could be upgraded to manage the collected data (WHO Uganda Country Office, 2001). Through donations from development partners (UNFPA, European Union, WHO, USAID, etc.) and other government programmes, most of the district headquarters have acquired at least one computer unit in the past 3 years. It should be emphasized that although 95% of the district headquarters have access to a computer, only about 20% have internet connection (WHO/MoH, 2004). Computer use at health centre level is far below 10%. It would take a huge investment to purchase computer units for all health facilities in Uganda, connect them to e-mail networks and train all health workers to use them. Proposals have been written to solicit for funds to upgrade the district computers, purchase new ones where needed and train health workers on electronic data management, analysis and reporting. Also, a training programme on use of Epiinfo software for district-level health workers has been started in 10 selected districts which received computer units from a WHO/ USAID grant in 2003. A training manual to this effect has been designed (WHO Uganda Country Office, 2003) Personnel
There are limited numbers of records assistants at the health facilities who are the primary data collectors of the HMIS. Their day-to-day work involves registering patients, tallying and compiling reports for transmission to the health sub-district. Most of these records assistants do not have a medical records training or background and are most times high school drop-outs. They are given on-job orientation and support by the health facility in-charges who are normally trained nurses, midwives or clinical officers. Some health units, especially levels 3 and 2, do not have records assistants, in which case one of the few health workers is assigned this work in addition to his/her routine work. This affects timeliness of reports from such health units. At the health sub-district level, there is normally a trained records assistant who takes charge of summarising the data from the health facilities and running some simple analyses. Although some health sub-district records assistants have never had formal training in records management, they have had an extensive degree of exposure through HMIS workshops and support supervision, and have been instrumental in steering HMIS work in the health sub-districts and supervision of the lower health facilities on records management. They are also regularly supported by the health sub-district in-charge who is normally a trained medical doctor. At the district level, there are two officers designated to handle HMIS and surveillance activities. These may have formal training in records management and statistics, or may be trained medical personnel with vast exposure on HMIS implementation. They normally work together to compile reports from the health sub-districts into district summaries, analyse data on health indicators in the district and are responsible for reporting to the Ministry of Health. They are also responsible for coordination of support supervision and training on HMIS issues in the entire districts. At the Ministry of Health, a health databank (Resource Centre) is equipped with two biostatisticians and a data manager who receive the reports from the districts, either by post, fax or hand delivery. They log the date when reports are received and proceed to enter the data into a standardised computer database, based on Epiinfo software. At the end of the month, automated programs are run to produce a number of reports on health sector indicators, including utilisation of out- and in-patient services, coverage rates for immunisation, contraceptive prevalence rates and morbidity levels for priority diseases. This team ensures that feedback to the districts is provided regularly, including requests for clarifications on inconsistencies in the reported information, and disseminates reports to all stakeholders in the health sector within and outside Uganda, both electronically and in hard copies. In collaboration with development partners, this team also coordinates training activities on HMIS issues in the whole country. Results Current reporting levels of the HMIS
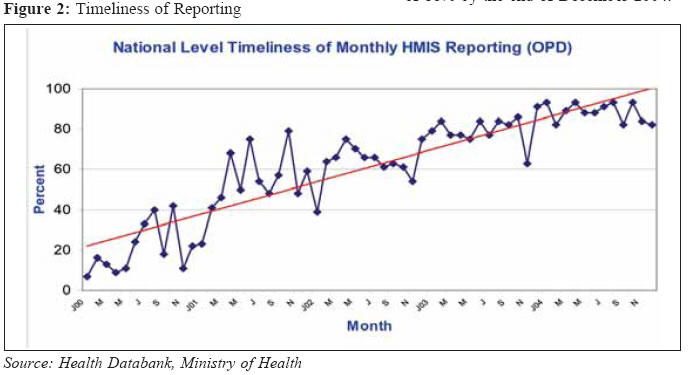
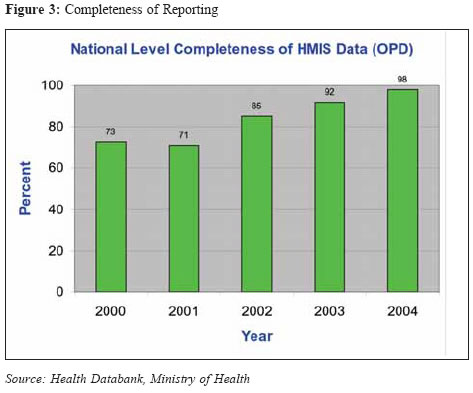
Timeliness and completeness of HMIS reporting has been considered a key process indicator for the implementation of the Health Sector Strategic Plan (2001 - 2005) and the 5-year target set at 80% (Resource Centre, 2001). Timeliness in reporting has been defined as receipt of the monthly report at the Ministry of Health by the 28th day of the following month. These cut-off dates vary from 7th at the health facility to 14th at the health sub-district and 21st at the district level. On the other hand, completeness is defined as the proportion of health facilities reporting out of the total number of units in the districts. This is similarly defined at the district and health sub-district levels. During the past 5 years, timeliness of monthly reporting of out-patient data from the districts to the central level improved markedly from a national average of 21% in 2000, 63% in 2002 and 88% in 2004. The graph below shows the trend in timeliness of monthly HMIS reporting from the districts to the centre. Timeliness at district level had also improved to an average of 88% by the end of December 2004. Similarly, there was also general improvement in completeness of the data reported to the Ministry of Health from 73% in 2000 to 85% in 2002 and 98% in 2004 (Figure 3 below). District-level completeness has also improved in a similar order. It should be noted that data on in-patient information (admissions, bed occupancy, deaths, etc.) has been very scanty due to non-availability of the necessary reporting tools and the limited sensitisation of clinicians. With the on-going feedback provided at all levels, coupled with training workshops and support supervision with a focus on the importance of reporting in-patient information, 38% of the districts reported in-patient data to the Ministry of Health in 2004 compared to as low as 5% in 2001 (Resource Centre, 2004). Discussion During 2000, the number of districts submitting monthly reports in time was very small (<50%). However, with improved feedback from the centre to the districts, reporting improved significantly during most of 2001. This feedback included a summary showing the performance of all districts in terms of HMIS reporting and some graphs of key disease trends. This feedback would not only be sent to the district health team, but would also be copied to the district political leaders (Chief Administrative Officer, District Chairperson and Secretary for Health) and would sometimes be discussed in the district council. During 2002, there was some decline in the level of reporting. This was mainly caused by the limited availability of HMIS reporting tools in most of the districts, which have traditionally been supplied by the Ministry of Health in order to maintain uniformity and standardisation. However, due to increased knowledge and motivation of health workers on the use of HMIS, coupled with funding gaps, the ministry could not cope with the level of utilization of the HMIS tools in the districts. Also, the established reporting process from the districts used to be bogged down by the many focal points in the Ministry of Health which could sometimes lead to late processing or even loss of the forms. Towards the end of 2002, funds were secured to print and disseminate enough HMIS materials, and the result can be seen in the improved levels of reporting during 2003 and 2004. The main health databank has also been equipped with improved communication means (fax, telephone and e-mail) so that all reports from the districts are received and processed at one point. The initial focus of the HMIS in Uganda was on out-patient data. However, since 2003, revised in-patient forms have been introduced for collection and reporting of in-patient and mortality data on a monthly basis. There has been slow uptake of in-patient reporting, however district and regional referral hospitals have been picking up. The rapid implementation of the Integrated Disease Surveillance and Response (IDSR) strategy in Uganda (MoH, 2002) has also contributed greatly to the registered improvements in HMIS reporting. The strategy has strengthened ownership of the HMIS since all programmes plan supervision, monitoring and training together, resulting into an improved integrated reporting system. Use of HMIS data for programme planning and monitoring
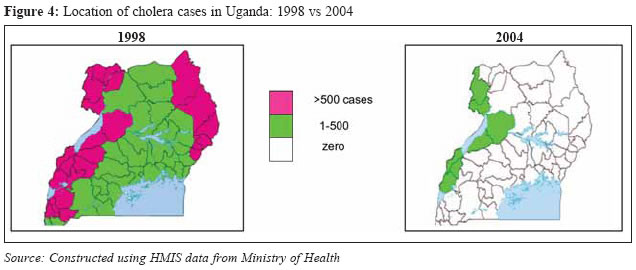
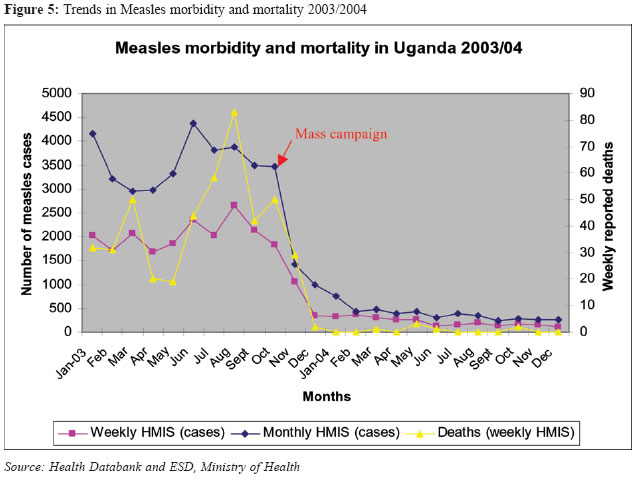
Many programmes in the Ministry of Health use HMIS data for planning and monitoring purposes. A quick example is the Expanded Programme on Immunisation (EPI) which regularly reviews the coverage rates and identifies poorly performing districts for support supervision and more financial help where necessary. All this analysis and assessment is based on the HMIS data reported from the districts to the Ministry of Health. The trends of epidemic-potential diseases (e.g. cholera) in Uganda and the impact of the program interventions can be clearly shown since 1997 using HMIS data. There was a huge cholera epidemic in 1998 which covered the whole country, most probably as a result of the heavy El nino rains. A multi-sectoral intervention programme spearheaded by the Ministry of Health was implemented and within less than a year, HMIS data shows that the epidemic had been brought down in most parts of the country. Since 2001, there have been sporadic cholera cases and HMIS data provides a distribution with districts bordering the Democratic Republic of Congo as affected, probably due to the poor sanitation levels and the recurrent movement of refugees (Figure 4). Interventions to control the spread of cholera are therefore being targeted in these districts. A review of measles epidemiology done in 2002 used HMIS as one of the data sources to determine trends of measles cases over time and the impact of under-five immunisation campaigns on the routine immunisation coverage rates on the trends (Nanyunja et al, 2003). Together with sentinel sites and laboratory data, it was shown that over 90% of the measles cases were in the age group of 6 months to 14 years and this formed the basis for the current 5-year measles control strategy, which included among other activities under-15 mass campaigns to cover the most affected age groups. Furthermore, impact of government programmes can easily be assessed using HMIS-reported data. The government of Uganda has on several occasions implemented programmes to eradicate, eliminate or control a number of health problems. The home-based management of fever strategy, polio eradication, water and sanitation improvement, guinea-worm eradication, measles control and HIV/AIDS control programs are some of the many programs implemented to improve the health status of the Ugandan population. However, it would have been difficult to assess whether or not these interventions are effective without analysing the data reported through HMIS. An example to demonstrate this point is based on the mass measles immunisation campaign which was conducted in all districts in October 2003 targeting all children under 15 years of age. The results, based on data reported in the HMIS, indicate a positive impact of the campaign on reducing measles morbidity and mortality as shown in the graph below. HMIS-reported data has also facilitated the process of assessing districts by constructing league tables that compare achievement in the different health sector indicators (WHO, 2003; MoH, 2004). A selected set of key indicators for monitoring the health sector strategic plan are considered (HMIS reporting, total OPD utilisation per capita, proportion of children under 1 year completing immunisation, proportion of deliveries administered in health facilities, etc.) and data for each district is extracted from the reports on an annual basis. Scores and rankings are then worked out to identify the best, average and worst performing districts. The best performing districts usually get prizes during the annual national health conference. This, in a way, stimulates health workers in the districts to work harder and ensure progressive improvements in the delivery of health services. Challenges
For the success of any programme, human resources play a crucial part. There is a small number of trained data managers at the Ministry of Health to process the huge volumes of data generated from the districts and be able to produce outputs timely. The districts, health sub-districts and health centres also lack trained data managers and records assistants. Although tools for capturing in-patient data were designed and disseminated to all districts, the response in terms of reporting has been minimal. For instance, during 2004, only 21 (38%) out of the 56 districts reported in-patient data to the Ministry of Health. Out of these, only 6 had reported in-patient data every month. Some of the factors contributing to this include the little sensitisation that was given to the clinicians in the health facilities on the importance of reporting in-patient data. Also, the reporting form appears too big as it requires data on admissions and deaths for about 70 different diseases and conditions, and computation of some indicators (e.g. number of patient days, average bed occupancy, etc.) on a monthly basis. The availability of HMIS tools (forms, patient cards, databases and manuals) needs further streamlining. Provision of these tools by the Ministry of Health seems not to be sustainable as there are frequent shortages. Data analysis practice has taken root in most of the health facilities. Graphs of disease trends and key indicator levels are regularly plotted and displayed in many health facilities. There is, however, little evidence to show how this data is utilised, especially at the district, health sub-district and health facility levels. Electronic data management and reporting is still lacking. There is a big challenge of acquiring the necessary financial resources to upgrade computer units in the districts and purchase new ones, install the appropriate data management software, train users and connectivity to the electronic network. Recommendations
There is need to establish and train the appropriate cadre of staff in order to have a good quality HMIS. This calls for additional training and support supervision, focusing on data analysis and utilisation of the outputs for planning, forecasting drug or vaccine needs and response to disease outbreaks. There is need to simplify the in-patient reporting tool and to sensitize more health workers in hospitals and health centres with in-patient services on the advantages and use of in-patient data. The on-going discussions of revising the HMIS tools should further be supported and the training program supported by development partners like WHO, UNICEF and UPHOLD should put a substantial focus on in-patient data collection, analysis and utilisation. Since districts are now decentralised and manage f unds for primary health care, it will be necessary to empower districts and health sub-districts to purchase HMIS tools from a standardised source. The challenge then will be on the districts to purchase all the required forms. The implication is that the Ministry of Health funds that are earmarked for HMIS forms thus must be distributed to the districts. It is necessary to do more advocacy to development partners in order to realise the HMIS computerisation project. This will improve on the reporting and feedback to and from districts to Ministry of Health, reduce on errors in reported data and improve on the data analysis culture by health workers. Conclusion
Although there are bottlenecks, the HMIS is established and functioning in Uganda. Even with limited resources, it has been proven that HMIS can be implemented to provide the basic information required for planning, monitoring and evaluation of health programs. Significant progress has so far been registered in regular reporting through a network of districts, health sub-districts and health facilities, linked to the central Ministry of Health. The data processing machinery is in place at the centre and a regular feedback mechanism has been established. If the main challenges of human resource capacity, in-patient data collection and processing, regular availability of HMIS tools, data utilisation and electronic data management are adequately addressed, a robust and high quality HMIS will be fully operational in Uganda. Mr Amos Nzabanita can be contacted at the Ministry of Health, P.O. Box 7272, Kampala, Uganda. References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University
The following images related to this document are available:Photo images[hp05008f4.jpg] [hp05008f2.jpg] [hp05008f3.jpg] [hp05008f1.jpg] [hp05008f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}