 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 3, No. 1, April, 2005, pp. 87-91 THE HEALTH SITUATION AT AWER INTERNALLY DISPLACED PERSONS' CAMP - GULU DISTRICT, UGANDA Komakech Innocent Gulu District, Uganda Code Number: hp05012 Abstract Uganda's close to 2 decades long conflict has led to a humiliating humanitarian situation in the IDP camps created by the government. A senior UN official, Jan Egeland described the humanitarian situation as 'the worst in the world'. An assessment of the public health situation was done in one of the IDP camps (Awer camp) some 15 km West of Gulu town on the Gulu Adjumani highway from 28th may - 18th June 2004. The findings suggested that the sphere standards for humanitarian interventions were not being adhered to by the humanitarian agencies for all the most basic necessities such as water and sanitation, food, shelter, and health services. Introduction
Uganda, described by Winston Churchill as the 'Pearl of Africa' is now home for military conflict. At a little camp around Lamogi Sub county headquarters (Awer camp) in Gulu, 26,592 people (as of 18th May 2004) crowd in huts constructed on a 2000 sq.metres of land squeezed between two swampy streams. A conflict that resulted from suspicion among the defeated soldiers of Uganda National Liberation Army (UNLA) in Acholi following ultimatums on Radio Uganda by the National Resistance Army officials shortly after military take over, is now 19 years old (started in August 1986) (Rapheal, 1998 & Lamwaka, 2002). After ten years of fighting (in 1996).with the rebels in northern Uganda, the government justifying that she wanted to protect the rural villagers from abduction and murder by the LRA rebels initiated a mass civilian displacement into camps. By October 2003, there were 32 designated camps in Gulu alone. At this period WFP estimated that the country had a population of 1.5 million IDPs. The estimates suggested that 439,000 people (91.6%) of Gulu district were living in the IDP camps (WFP, Uganda (1), 2003). Because the conflict is perceived as entirely a domestic affair, humanitarian assistance and protection to IDPs in the camp have continued to face great challenges. The humanitarian agencies are firm that all assistance to IDPs is a domestic affair of the responsible states less the IDPs cross a recognized international border. The countries that harbor IDPs on the other hand, are usually at war and may not be in position or even willing to arrange emergency humanitarian assistance to the IDPs as her government fights the war (Salama, 2001). Public health measures are more difficult to tackle during mass displacement. WHO has advised that, the best option to avoid deterioration of public health in communities of war zones is to prevent population displacement altogether (WHO, 2000). Provision of safe water, hygienic sanitation, adequate nutritious food, and hygienic housing and health services is a hard task during mass displacement of the people. As a result, countries resort to foreign teams that may have little experience or training to work in the developing countries (Toole, 1993). The responses of the foreign teams and governments are also not uniform. Ill responses to humanitarian emergencies are common in areas with limited international interest. World leaders are only willing to justify the availability of enormous resources for displaced persons as 'moral imperative' when such displacements occurs in areas of greater international political interests (Toole, 2002). No equity exists in humanitarian assistance; it's the most vulnerable of the displaced persons who receive lesser humanitarian assistance, protection or even media coverage. The way the world apportions its generosity either in humanitarian aid or in conflict resolution is inconsistent (Toole, 2002). But, the widespread wars in Sub Saharan Africa, home to diseases targeted for eradication will reverse the hope for 'Health for All'. Polio eradication and Malaria control face very disturbing challenges in the war prone Sub Saharan Africa (WHO, 2000). Eradication of wars from Sub Saharan Africa is therefore a pre requisite to instituting effective public health interventions. Materials and methods
A total of 184 household heads and 106 children less than 5 years participated in the descriptive cross-sectional study. Semi-structured questionnaire were used to interview respondents. The study involved; Household heads that was at least one year in the camp and Children under five years of age. Systematic sampling used select respondents using the list of the food distribution records kept by Rwot Kweri. In total, 24 (out of the 42) Rwot Kweri units were selected for the study. Water sources, sanitation, housing situation and the records from the health units that service IDP camp were assessed. Members of Awer camp committee were also interviewed using a questionnaire. Results
The rebel atrocities and indiscriminate government military bombing forced the rural Villagers into Awer camp. Most of the villagers were physically rounded up and collected by the government military in October 1996 to an area which became Awer IDP camp. There were no relief programs in the camp until July 1997 (about 9 months later). Housing situation
The cone-on-cylinder shaped huts are 1-2 metres apart with the roof inclines touching each other in many areas. The huts do not contain any windows or other ventilators. Each IDP occupies an average of 1.8m² per person per hut. Latrine situation
Forty four persons use one pit latrine in the camp. Only 18.2% of the latrines can be used during night hours. Large numbers of cockroaches inhabit the poor pit latrine built by each family. World Vision International (a local NGO) supplies the latrine slaps at a fee of 2000/= per slab. The latrines are built within crowded settlement, are about 2 metres to the huts in many places and are not VIP compliant. Water situation
There are 5 protected springs and 5 boreholes around the camp. A fee of 200/= is levied per household per month to be allowed to fetch water from any of these sources. The per capita water consumption was 4.6 litres per person per day. The queuing time varied from about 10 minutes in the morning hours to 4 hours during peak hours. Health services
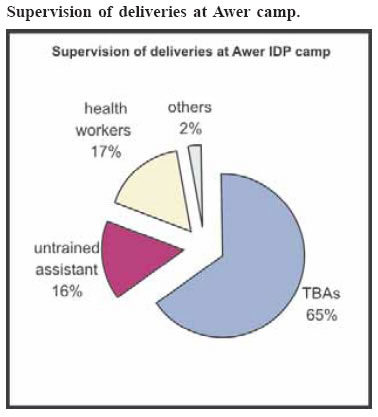
Awer camp had one private for profit medical clinic and four drug shops. Community based health workers and a Nursing Assistant run the drug shops. The drug shops sell both class B and class C drugs. None of the drug shops had evidence of operating license from the National Drug Authority (NDA). The health center II constructed in 1998 is operated by Gulu district local government. The health centre offers general out patient services. The staffing in the health centre included; 1 Enrolled Nurse, 1 Enrolled Midwife, 2 Clinical officers and 2 nursing assistants who commute from Gulu town. The major causes of ill health among the IDPs of Awer Camp
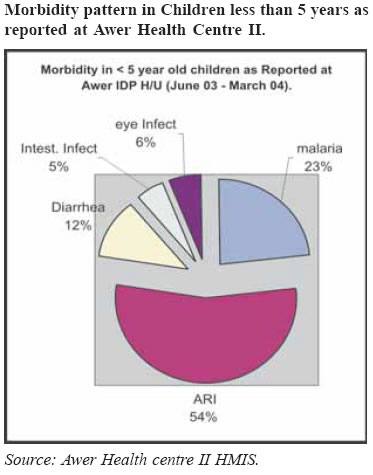
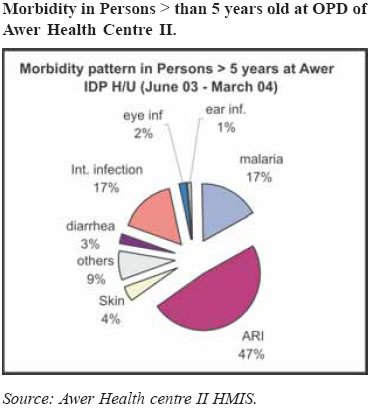
A total of 85.9% of the respondents reported ill health in the past 2 weeks. The above finding suggests that acute respiratory tract infection is the leading cause of morbidity among the under 5 year old IDPs. Amongst the IDPs older than 5 years of age, acute respiratory tract infection is the leading cause of morbidity. Deliveries at the Camp Food supplies
WFP supplies 400 grams of maize per person per day and 60 grams of beans per person day and 4 liters oil for a household of 5 people in 30-40 days cycle. Part of the maize grains is sold to meet the milling costs. One kilogram of maize grains covers the costs of milling 3Kg of maize grains. Nutritional assessment
Nutritional status measured by weight for height Z-scores in children less than 5 years at Awer IDP camp.
It can be observed that 54.5% of the children less than 5 years that were assessed had some form of malnutrition. Discussions
The findings suggest that both the Ugandan military and the rebels of the Lord's Resistance Army (LRA) actively participated in the forceful displacement of the rural villagers into Awer camp. The attempts by the civilians to maintain neutrality in the conflict led to their displacement into camps; since this position created dissatisfaction to both the government military and the rebels. As rebels looted, abducted children and murdered the people of Lamogi, the government military indiscriminately launched bombs into the villages and physically gathered the rural villagers to their military detach at Lamogi Sub county headquarters (which later became Awer IDP camp). In 1996 alone, the Government of Uganda forcefully displaced 300,000 rural villagers homeless to the camps in northern Uganda (Brown and Sayre, 2002). The rebels annoyed that the civilians allowed to be taken to the camp continued to attack the civilian positions in the camp to loot and kill. Because of the competitive nature of the act, the government military did not arrange for the welfare of the IDPs while at camp. The relief program of the World Food Program pioneered only 9 months later, in July 1997. The government military was then faced with a complex emergency which they had no capacity, knowledge and/or willingness to manage. The military was for sure not prepared to tackle the humanitarian crisis which they created. Contrary to Sphere standards to settle IDPs at locations that minimize their exposure to mosquitoes (Sphere Project, 2004), the IDPs are damped in an area surrounded by 2 swampy streams each barely 50 metres away on either side of the settlement. As the mosquitoes rejoice, the incidence of malaria is up. In 2004, it was report by the WFP that 80% of the IDPs had malaria in the past 2 weeks (WFP & UNICEF, 2004). The camp position is therefore a great hazard to the IDPs; but who cares? Only 4.6 litres of water is available for each person in 24 hours for all activities that require water. The Sphere project guidelines for minimal humanitarian standards recommend at least 15 litres per person per day (Sphere Project, 2004). Activities of daily living such washing and personal hygiene maintenance are negatively affected when there is water scarcity (UNHCR, 1992) Forty four people shared one latrine stance compared to the recommended maximum of 20 persons per latrine in the Sphere standards. Diarrheal diseases were reported by 50% of the IDPs in the past 2 weeks alone (WFP and UNICEF Uganda, 2004).Inaccessibility of most latrines during night has led to in indiscriminate faecal disposal in the camp with the resulting consequences. Each person occupies a hut space of about 1.8 m2 compared to 3.5 m2; per person prescribed in the Sphere standards (Sphere Project, 2004).Respiratory tract infections is the leading cause of ill health in this camp partly due to high congestion in the huts. High congestion and crowding is a great risk especially in areas of high prevalence of tuberculosis http:// www.memo.ru/eng/hr/return02e.htm as of 4th July 2004). The appropriateness of operating a health centre II in the congested Awer camp is debatable. During emergency medical assistance, the health care delivery structure should allow referral of patients by the health visitors at village level to curative health centre that caters for 3000-5000 people. Accordingly, populations of greater than 5000 should be served by a curative health centre with beds and nutritional feeding centre (equivalent to health centre III in Uganda) that can refer to a hospital (Wim, Wim and Beolart, 2002). Applying this model could mean, the camp would be served by at least 5 health centre IIIs. Displacement of people is not cheap either as this result in frequent ill health and many deaths if very poor, inaccessible health service and/or inadequate facilities and interventions that determine health are all that is available. Although the health centre II offers services free-of-charge for the patients, long waiting of up to 4 hours before being seen by a health worker is common. One elderly woman complained that "at that health centre, we pay with our buttocks" meaning that the patients have to sit for long hours waiting before receiving care. The staffs live in Gulu town, resulting in patients being seen only between 12 noon - 3pm. The WFP supplies is calculated to provide about 1129.7 Kcal of energy per day (if 1 kg of maize grains provide 2.8 kcal of energy - (computed from FAO table of calories obtained from maize grains for rural Kenyans; FAO, 1992 at http://www.fao.org/docrep/ To395E/T0395E00.htm ). Applying the same formula and adjusting for losses due to sale of maize grains to cover milling costs, reduces calorie value to 847.3 K cal. Men in rural poor communities may consume about 600 grams of maize compared to the women's 400 grams (FAO, 1992 as at http://www.fao.org/ docrep/To395E/T0395E00.htm).The children require about ¾ of the adult ration when 2 - 5 years of age (FAO, 1992), raising serious gender concerns on the nutrition of the displaced women and children especially when equal quantities are supplied irrespective of gender and age. The Sphere standards recommend a daily calorie intake of 2,100 Kcal per person per day be used in computing for food supply quantities if the population is not being disaggregated by age and sex (Sphere Project, 2004). The finding suggests Acute Global Malnutrition was as high as 20.5% in the children of 6-59 months in Awer. This could be worsening trends in nutritional status of the IDPs Awer camp. Action Against Hunger found in April/May 2003 that, the AGM was 10.2% (but aggregated for various camps). WFP & UNICEF reported in Sept/Oct 2003 AGM of 16.8% at Awer camp (WFP & UNICEF, 2003). The impression could be that either rates of malnutrition are increasing in the IDP camp or there are methodological differences in the assessment; but likely worsening given the large number of children with mild malnutrition who could be deteriorating to other severe forms of malnutrition. Food inadequacy is the most likely cause of the observed malnutrition due to supply losses and inadequate quantities supplied. Recommendations
The humanitarian agencies could consider the following: 1) Mobilize additional resources for the construction of water and sanitation facilities; 2) WFP could consider providing additional resources to the implementing agents such a Norwegian Refugee council so that she may process the maize grains into maize flour prior to distribution to the IDPs; 3) An agency with capacity and experience could also consider an intensive vector control program primarily targeting Mosquitoes and cockroaches; 4) Save the Children - Uganda could also scale up their nutritional feeding program to include at least children less than 5 years with mild malnutrition; and 5) World vision International could reconsider their policy on the latrine slabs to encourage the IDPs build more latrines. The agency could consider supplying the slabs free of charge to the IDPs. Gulu district directorate of health services could consider: 1) Upgrading Awer health center II to health center III so the unit can provide more comprehensive health services including some in patient care; 2) Further strengthening supervision of Awer health center so the staffs are more encouraged to produce their required output; and 3) Strengthening its supervision of the drug shops in the camps to reduce on irrational use of antibiotics. Conclusions
The findings demonstrate that state sovereignty has been taken too far. The Geographical land mark, 'a recognized international border' is the sole criterion on which the IDPs are starved to their bones, as states that displace the rural villagers are absolutely free to provide no assistance. Defusing of responsibilities by international community has resulted in no assistance to IDPs and to the camps being managed by the government military; and not the implementing agencies of a humanitarian organisation as for refugees. Displacement of people should not be solely viewed in terms of physical protection from human rights abuses. Inadequate site planning and humanitarian interventions have resulting negative public health consequences that are long term and possibly more disastrous to the displaced population than human right abuses per se. If the current HIV pandemic does not provide an impulse for the international community to upgrade Public health systems during situations of internal displacement, then nothing will do. The author is a nursing officer working in Gulu District. He has recvently completed a Masters degree in Health Services fManagement at Uganda Martyrs University, Nkozi, Uganda. He can be contacted at innocentkomakech@yahoo.com. References
The following images related to this document are available:Photo images[hp05012g3.jpg] [hp05012g2.jpg] [hp05012g1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}