 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 3, No. 2, August, 2005, pp. 121-128 THEME 1: ISSUES IN SERVICE DELIVERY THE DEVIL IN THE DETAILS: EARLY EVALUATION OF HOME-BASEDMANAGEMENT OF FEVER IN NEBBI DISTRICT, UGANDA Luigi Cicció, Visiting Lecturer, Uganda Martyrs / Technical Advisor CUAMM, Arua and Nebbi Districts Code Number: hp05020 Abstract Every day, 3,000 Africans, mostly pregnant women and children, die of malaria, which in Africa still represents the top disease in both morbidity and mortality. Heads of state of African countries made a commitment, in April 2000 at Abuja, Nigeria, to ensure that at least 60% of those suffering from malaria have prompt access to affordable and appropriate treatment within 24 hours of the onset of symptoms. Prompt access to effective anti-malarial treatment is an essential pillar for reducing the disease burden. One of the strategies to bring treatment as near the home as possible is the Home Based Management of Fever (HBMF), where trained community volunteers use pre-packaged drugs to effectively treat children with fever within 24 hours of onset of illness. This strategy is already being practised on a limited scale in some countries in Africa, and has been scaled up countrywide in Uganda. We illustrate the case of Nebbi District, where implementation started last year in June, trying to identify the strengths, the achievements and the constraints of this programme. In particular, we compare the number of reported cases of malaria in under-5 children before and after the HBMF was introduced. Introduction Malaria by far contributes major share of disease burden in Uganda. In the Financial Year 2003/2004, it was responsible for 52% of all outpatient visits, 30-35% of all inpatient admissions, 9-14% of all inpatient deaths and 20-23% of deaths in children under-5 years (MOH, 2004). In recent years there has been an upward trend in clinically diagnosed malaria cases reported in the Ugandan Health Management Information System (HMIS) with data from both government and non-government health facilities. There was a 230% increase in cases over the 6 year period from 1997 to 2003 (from 5 million in 1997 to 16.5 million in 2003). In 2003 alone, children under 5 years had an incidence rate of 0.98 malaria episodes/ year compared to 0.64 episodes in older patients. The overall estimated case fatality rate in 2001 was 4.1%. Currently, it is estimated that the annual deaths from malaria in Uganda are from 70,000 to 100,000 (CDC, 2005). Malaria disproportionately affects poor people. Rural populations carry the overwhelming burden of the disease. People living in poor quality housing are particularly at risk. In addition, poor people are at greater risk of complications and death, because of a number of factors, including limited ability to access effective treatment. Malaria also contributes to poverty by reducing the productivity of infected people and their caretakers. Households spend significant sums (from US$ 0.39 to US$ 3.84/per capita/per year in Sub-Saharan Africa) to prevent and treat malaria (World Bank, 2001). A multi-country review of the Integrated Management of Childhood Illness (IMCI) initiative that included Uganda indicated that the majority (83%) of fever cases is managed outside the formal health services with shopkeepers, drug stores and private clinics being the predominant sources of care (MOH, 2000). Moreover, 79% of the above "self- medication" group were using the western type of medicine, with drugs given incorrectly, in incomplete doses and, often, in dangerous combinations. Early treatment of malaria is critical, especially in children: the disease progresses rapidly, with a high rate of complications like cerebral malaria, anaemia, and hypoglycaemia, to mention but a few. Most child deaths from malaria occur within 48 hours of onset of illness. Factors such as distance from the nearest health facility, economic constraints, intra-household decision making processes, irregularity of the drug supply at health units, use of traditional remedies and healers, and lack of rapport with health workers can all delay treatment. The Abuja Declaration (2000) In April 2000, forty-four of the fifty (88%) malaria-affected African countries attended a summit in Abuja on Roll Back Malaria (RBM) and signed the Abuja Declaration, which reflected a real convergence of political momentum, institutional synergy and technical consensus. By signing the Declaration, the African leaders committed themselves to an intensive effort for better control of the scourge, through agreed implementing strategies and actions. The Declaration states in part that "…taking note that malaria accounts for about one million deaths annually in Africa, nine out of ten cases of malaria worldwide occur in Africa south of the Sahara, malaria costs Africa more than US$ 12 billion annually, and can be con-trolled for a small fraction of that amount; those who suffer most are some of the continent's most impoverished and that malaria keeps them poor; a poor family living in malaria affected areas may spend up to 25% or more of its annual income on prevention and treatment; malaria has slowed economic growth in African countries by 1.3% per year: as a result of the compounded effect over 35 years, the GDP level for African countries is now up to 32% lower than it would have been in the absence of malaria"…… (Abuja Declaration, 2000). At the end of the summit, all Heads of State and their representatives took the resolution to set some targets in fighting malaria, to be achieved in the next five to ten years, consistent with the United Nations Millennium Development Goals (MDG). Some of the most MDG-relevant objectives related to malaria were the following: a) to halve the malaria mortality for Africa's people by 2010; b) to ensure that by the year 2005, at least 60% of those suffering from malaria have prompt access to and are able to use correct, affordable and appropriate treatment within 24 hours of the onset of symptoms; c) that at least 60% of those at risk of malaria particularly pregnant women and children below five years of age, could benefit from the most suitable combination of personal and community protective measures such as insecticide treated mosquito nets and other interventions which are accessible and affordable to prevent infection and suffering; d) that at least 60% of all pregnant women who are at risk of malaria, especially those in their first pregnancies have access to intermittent presumptive treatment. Malaria Control Programme in Uganda Based on the Uganda National Malaria Control Policy and the first Health Strategic Sector Plan (HSSP I) and the Minimum Health Care Package, the Uganda Malaria Control Strategic Plan FY 2001/2-2004/5 states four main elements of the strategy for malaria control:
This package of interventions is also consistent with the four pillars of the Roll Back Malaria advocated by the World Health Organisation (WHO). Some efforts have been undertaken by the National Program to improve health workers' knowledge and skills in the management of uncomplicated as well as severe malaria. This has been done in close collaboration with the Integrated Management of Childhood Illnesses Program. It is recognized, however, that further interventions have to target the treatment-seeking behaviour at the household level and in the private sector, since all evidence shows that a large share of fever episodes are treated at home with drugs purchased mainly from the private sector (such as drug shops). Other experiences In Africa, where the mortality burden from malaria is greatest, the majority of children die before they reach health facilities. Poverty, distance from home, financial constraints, the demands of domestic life, perceived poor quality of service, drug stock-outs, and negative health workers' attitudes and behaviour all act concurrently, making the would-be users by-pass recognised health care facilities in favour of the private or informal sector (often with inadequate, in-appropriate or poor-quality drugs). The availability of adequate and effective treatment near to or in the home is therefore very important and could be a major strat-egy for the African region. The (HBMF) strategy was shown to be both feasible and effective in ensuring prompt access to appropriate treatment in the African region (Kidane, 2000), though some studies have cast some doubts about the ability of mothers to recognise fever signs in their children (Bailo Diallo, 2001). One of the most comprehensive documents by the WHO regarding this strategy recognises that some issues are crucial in the process of its scaling up and they have to be fully taken into consideration by both policy-makers and implementers (WHO, 2004). The following are some of them:
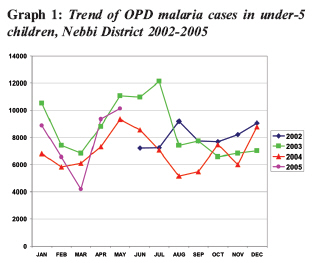
In summary, scaling up HBMF is both feasible and effective - and is already being implemented on a limited scale in some African countries, like Burkina Faso, Ghana, Kenya, Nigeria, and Zambia. Research experience and demonstration projects have provided guidance on how HBMF can be scaled up to reach the majority of populations. Uganda has been one of the first African countries to extensively scale it up (Wendo, 2002). Home-Based Management of Fever (HBMF) Strategy in Uganda In response to increasing drug resistance to first-line single antimalarial treatment (either chloroquine or sulfadoxine-pyrimethamine), the Ugandan Ministry of Health shifted to a combination of both as the first line of treatment. To address the problems of access and timeliness of treatment, the Government of Uganda adopted the Home-Based Management of Fever/ Malaria (HBMF) strategy to improve the recognition, management, and treatment of fever/malaria among children less than five years of age at the community and household levels. It was supported by the World Health Organization (WHO) in line with the Roll Back Malaria programme. Under HBMF, all children under 5 years of age are treated as malaria presumptively in order to improve the chances of early correct treatment and reduce the chances of complications arising from delayed treatment. By treating the patients from their home or community, it also helps to avoid some of the barriers that stop people from bringing their children to health facilities e.g. distance, health worker attitudes, money etc. On Africa Malaria Day in April 2002, Uganda started to implement the rolled-out large-scale programme. This is currently the nation's official malaria treatment policy. Every participating community has at least two volunteer drug distributors trained to recognize the symptoms of malaria and provide appropriate drugs free of charge to children under-five. The volunteers are expected to be available 24 hours a day and the patients can therefore be served promptly. The community-based drug distributors were taught to counsel the caregivers to ensure they administer complete treatment with Homapak even when the child seems to have recovered and to refer children with signs of severe illness to the nearest health unit for treatment by qualified health workers. The health system contributes to building community capacity through training of volunteers. It also provides IEC materials, ensures a constant supply of anti-malarial drugs and provides support for data collection, monitoring and supervision. Unit-dose, pre-packed Chloroquine (CQ) and sulfadoxine-pyrimethamine (SP) tablets or Homapak are distributed within the community by trained drug distributors. (There is a pun in the name of the combi-nation because the drugs are distributed at home, and fever is called 'homa' in the Kiswahili language under-stood by a large number of people in Uganda. There-fore, it may be understood to be a home pack or, indeed, a pack for treating 'homa'). It was agreed to pack the treatment in packs of two different colours according to the strength for easy identification in the community since most rural Ugandan mothers cannot read or write. They are colour-coded: a red packet with lower strength drugs (Red Homapak) is used for children aged 6 months to 2 years and a green packet with higher strength drugs (Green Homapak) is used for those from 2 to 5 years. The drugs are distributed through community-based volunteers and public health units in 10 selected districts (see Fig. 1). The DD give the child the first dose of Homapak. They then explain to the caregivers how to give the remaining tablets and the possible side effects. They emphasize the importance of adherence to the specified course of treatment and finally, record basic data about the children treated. The results in other districts A recent study of the programme in the three districts of Kiboga, Kanungu and Kumi found out that the odds of receiving appropriate treatment for fever (CQ-SP combination) are nearly five times greater in intervention districts than in control districts. In addition to that, parents received better counseling on the importance of early treatment, fever management, and the signs and symptoms of severe malaria (MACIS, 2004). However, one challenge may be represented by the growing resistance to chloroquine and sulfadoxine-pyrimethamine in some parts of Uganda. Besides, supervision of the DD by the District staff is being constrained by lack of facilitation and travel funds, maintaining a constant supply of Homapak at the community level and the entire referral system needs to be strengthened (Batega, 2004). Involvement of and support from lower local government officials and local leaders are vital for ownership and sustainability of the program at the local level and community selection of DD is crucial and enhances community members' commitment to the HBMF strategy and utilization of HBMF activities. As a recent survey conducted in six Districts has revealed that community capacity building can enable communities to appropriately manage malaria cases among under-five children. Absence of a formal process for training and induction of replacement of DD may affect both the motivation of the DD and their acceptance by the community. The provision of IEC materials such as job aids for the DD is essential in sustaining their performance, and the supervision of DD can lead to enhancing their performance, confidence, and skills (Fapohunda, 2004). However, Homapak stock outs affect both the commitment of DD and the confidence of community members in the HBMF strategy and need to be minimised. Integration of HBMF activities into other health services within the district and sub-county enhances the supervision levels for the DD and also increases the sustainability of the HBMF program. Background of HBMF in Nebbi District Nebbi District has 54 operational health facilities. Currently, 47 ((87%) of them are directly involved in the implementation of HBMF strategy, which started in the District in June 2004 (though for most units it took off in July 2004). Malaria accounted for 37% of all OPD attendances and 45% of all consultations by children under-5 years in FY 2003/2004 (Nebbi DDHS Office, 2004). The training of an initial lot of five Village Health Team (VHT) members per village started in early 2004 throughout the district. Two of these were selected to be DD in each village, both sharing a single HBMF village register (which has sometimes contributed to incomplete or delayed reporting). Packets of red and green Homapak were distributed to all implementing Health Facilities, which, in turn, allocated them to the villages in their respective catchment area according to population figures. Each Sub-county had three health workers acting as supervisors, actively engaged both in the training activity and in monitoring the DD. However, initially the rate of submission of monthly reports was extremely low and very rarely attached to the submis-sion of the Health Unit Monthly Report, as envisaged. It took a comprehensive round of supervision of all units by a District team to strengthen the concept and to re-emphasise the importance of receiving the returns, for ordering more drugs from the centre. All implementing health units are supposed to compile three copies of the HBMF summary form. However, shortage of pre-printed forms and of stationery in general has been claimed as a reason for irregular submission or no reporting at all. Of recent, the reporting system has become more regular and consistent, even though not all DD's reports are usually incorporated in the monthly summaries submitted to the District. Between March and May 2005, the second phase of training for Village Health Team members took place, with a total number of nine members per village trained. Results of HBMF in Nebbi District From the time the programme started in June 2004 up to the end of May 2005, a total of 105,166 doses were given out (see Table 2), a ratio of 1.2 packs per under-5 child. Of these, 65.3% were given within 24 hours from the onset of the fever. Almost 95% of all the children treated recovered and only 0.5% of the children were reported to have died. Slightly more than 6% of the children treated at home with Homapak were eventually referred to the health units, due to treatment ineffectiveness. The HBMF summary forms do not provide adequate information to allow any comparison in the final outcome between the group of those promptly treated and the other group. The average number of children treated in a month is lower than 10,000, but this should take into account that in June 2004 few units had started implementing the programme. In addition, in December 2004, a shortage of Homapak packs affected the entire District, a situation compounded by the incomplete reporting by some DD. There are no data available about possible adverse reactions either. However, anecdotal reports by the DD seem to rate them as very rare in general. HBMF was expected to reduce the out-patient attendances by children due to malaria, since they were being treated at home. Graph 1 shows the trends of OPD malaria cases in under-5 children by month from June 2002 until May 2005 in the whole District, overlapped to cater for seasonal variations. Since the start of HBMF implementation (June 2004 - May 2005), the number of cases has dropped by about 4,000 (88,000 compared to over 92,000 cases during the same period in 2003/2004). The increase recorded in December 2004 could be attributed to the shortage of Homapak in almost all District Health Units and communities, and the subsequent sharp decline could be attributed to the arrival of the drugs, until the usual peak malaria season in May. Table 1: Homapak Drug Distribution in Nebbi District, June 2004 - May 2005
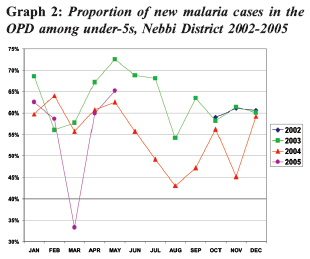
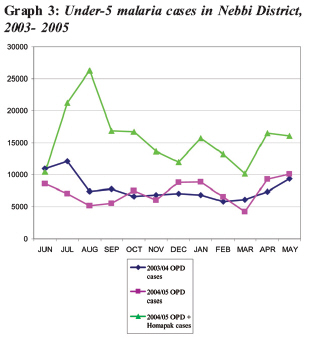
*Projected from the 2002 Census Data (Source: UBOS, 2002) assuming exponential growth. While there seems to have been a relatively minor reduction in the number of under-5 children attending the OPD for malaria, the devil is in the details, as they say. The proportion of malaria cases among all under-5 OPD attendances fell very significantly. The total number of OPD visits in children under-5 in the period June 2004-May 2005 rose by about 11,000 (from about 152,000 during the same period in 2003/2004 to over 163,000 cases). Therefore, the proportion of malaria cases out of the total number of OPD encounters in under-5 children fell from 61% in 2003/2004 to 54% in 2004/2005. This is a 7% fall compared to a 4% fall in the total number of cases (see Graph 2 ). However, the interpretation of these results needs to be cautious. The decline in OPD malaria cases may not be simply explained as a result of the administra-tion of Homapak. In fact, adding the total number of children treated by DD to the number of children taken to the health units and diagnosed having malaria gives almost double the figure of malaria diagnoses in children for the previous year (see Graph 3). Some other problems appeared immediately evident when we tried to analyse the data. The number of DD regularly reporting was lower than the number trained, though it has not been possible to establish their exact attrition rate. Some reports carried significant inconsistencies which could have affected the quality of the data in future. In a few villages, drugs and registers were either distributed very late or never distributed at all, leaving those areas underserved. Very few DD received any form of support from their community or local leaders, making some of them reluctant to continue with the distribution work. Some sub-county supervisors have been transferred from their original stations, thus reducing the necessary support and assistance to the DD. In some units the role of compiling the monthly return for Homapak is the responsibility of one health worker, whose absence may cause delayed submission of the data. It was observed that in most health units all the Homapak received from the district is issued out to the DD as soon as it is received, creating an immediate stock-out in the unit and inhibiting stock replenishment for those communities whose consumption is higher. In addition, it was found out that of recent, some boxes of Homapak near their expiry date were delivered to the district in large quantities. Discussion It is probably too early to start evaluating the effect of the HBMF strategy on the malaria situation in Nebbi District. However, these early results show a trend in the desirable direction. In particular, the 60% target set in Abuja concerning the children U-5 accessing to an appropriate treatment for malaria within 24 hours has been constantly fulfilled throughout the period considered. However, the data are available are still too few to enable us to comment reliably on the impact of Homapak on the burden of malaria cases in the OPD. Nevertheless, the data from eight other Districts show the same trend (MOH, 2004). It is not easy to tease out the effect of a general increase in utilisation of the services (due to a better link between the communities and the health units) or to a better coverage of the rural population served after the opening of new health centres (as the total increase of OPD encounters in under-5 would suggest), both of which would probably lead to a reduction of cases. It is also not possible to tease out the specific details of a possible radical shift from informal health care (self-treatment, drug shops, private health care providers etc) to the village-based Homapak by the hard-to-reach populations who are rarely seen in the health services. The informal health sector does not provide or even keep data on their clientele, to enable us to monitor a shift in their utilisation. We take into account the possible contribution of malaria over-diagnosis, especially at the lower level of service provision, which has been already demonstrated (Reyburn 2004), but also keep in mind that this bias would have affected the figures both before and after implementation of the Homapak strategy. An interesting - and probably more accurate -perspective to evaluate the association between the HBMF programme and the magnitude of malaria in under-5 children could have been to look at the data of under-5 admissions. This would give a better indication of the real impact of Homapak on the burden and the severity of malaria in children. Unfortunately, in-patient data were found to be too erratic and incomplete to allow any possible aggrega-tion and comparison between the different years. A crucial aspect is presented by the expected voluntarism from the DD. Studies have shown that even where people initially agree to volunteer, later "they will still possess high (hidden) expectations, which if not met, will gradually affect their performance. They tend to perceive such opportunities as those of employment not a community service" (MOH, 2001). In short, the risk of non-sustainability of the entire programme in the long-run is concrete, unless a system of incentive for DD is devised. Conclusions and future developments The availability of Homapak seems to influence the utilisation of formal health services. In order to sustain the HBMF strategy and achieve its objectives, the district needs to ensure a regular and reliable supply to avoid eroding the community's confidence in the system. The chain from quantification of needs, procurement and distribution still leaves much to be desired even at central level. In Nebbi District, some of the soon-to-expire boxes, though destined for the village DD, have been given back for use in the health units' OPD in order to minimise the wastage of drugs. Data collection is still requires serious improvement, through further training, supervision and facilitation of the DD. As suggested in previous evaluating exercises (Batega, 2004), some motivation factor to the DD, in form of identifying badges, certificate of appreciation or other facilities, could be useful for maintaining their interest and commitment to the programme. Another helpful tool could be organising regular meetings of DD at sub-county or health unit level, for collecting returns, replenishing supplies and giving technical support. Funds for this activity would have to be planned for and lobbied for by district or sub-district focal persons. While the case management is being improved at community level, the other alternative preventive strategies should not be neglected. Availability and use of Insecticide-Treated Mosquito Nets (ITMN) remain still negligible and, even then, most mosquito nets in use by the community are not treated with insecticides. The percentage of under-five children sleeping under ITMN is still unacceptably low (UBOS, 2001). It would be advisable for the ITMN promotion in the communities to be possibly integrated within the HBMF programme. The challenges ahead are still quite many. The change in malaria treatment regimen to Artesunate Combination Therapy (ACT) which is expected soon will also require even closer monitoring of the HBMF strategy to avoid the emergence of resistance. Cost implications and the risk of misusing the new drugs are strong reasons for planning additional support to the programme early enough. Many health workers managing children at health facilities are not well competent in IMCI and severe malaria case management, therefore lacking the requisite skills for managing, supervising, and supporting DD in communities, or for managing referrals from the community. A comprehensive training for health workers on the coming malaria drug regimen combined with an evaluative summary of the HBMF programme results is a key step for a successful outcome of the whole national malaria control programme. Acknowledgments I wish to acknowledge the valuable assistance of Mr Ponsiano Ondoga, the Malaria F.P. for Nebbi District and Dr Enrico Tagliaferri, the CUAMM M.O. in Nebbi District, whose contributions have been essential for writing this article. References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp05020g2.jpg] [hp05020f1.jpg] [hp05020t1.jpg] [hp05020g3.jpg] [hp05020g1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}