 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 3, No. 2, August, 2005, pp. 178-183 GENDER ANALYSIS OF HEALTH FACILITY UTILIZATION IN UGANDA Bakeera S, Talisuna A, Murindwa G, and Kirunga C, Ministry of Health, Kampala Code Number: hp05026 Abstract A gender analysis study of health facility utilization rates in Uganda over the period July 2003 to April 2004 was undertaken in four districts of Uganda. The key conclusions are that: (1) Collecting data to analyze for gender and age categories is a possible but tedious in a paper based system and is made more difficult in the absence of the Records Assistants; (2) Despite the limitations of sample size, there are indications that gender and age specific inequities do exist; (3) Although the study makes no firm conclusions as to whether there is gender or age specific inequity in OPD attendance, it does indicate that this information is collected using the current HMIS;(4) In an attempt to provide technical support to ensure that such data will be subsequently easy to retrieve, the team worked with the RA and I/C during the review but the contact was limited and it cannot be guaranteed that the process of data retrieval was improved. The key recommendations are that: (1) Conduct a detailed gender analysis study for the HSSP output indicators such as OPD utilization, immunization rates and some priority diseases such as malaria, and ARI pneumonia especially in childhood. (2) Institutionalize the conduct of gender and age specific analysis of routine HMIS data. A more pragmatic approach would be to conduct such record reviews every year or to routinely report gender disaggregated data in the HMIS monthly report. (3) Improve the capacity for HMIS data management to ease retrieval and analysis at facility level. Introduction In the recent past there has been increased advocacy for gender mainstreaming in the Health sector. (Bantebya, 2001). One of the topical debates is whether there are significant gender differences in utilization of health facilities in Uganda. Despite the latter being a topical issue, there is paucity of studies that have analyzed whether gender indeed has a significant effect on utilization rates in different age groups. The Ministry of Health’s Planning Department (HPD) in June in 2004, in collaboration with its Resource Centre (RC) and the Surveillance Division, undertook a gender analysis study using facility based routine HMIS data in four districts. The specific objectives were: to appreciate the ease of retrieving gender disaggregated data; to provide technical support to ensure that gender disaggregated data is collected at peripheral levels; to share expertise in mechanisms for enabling regular availability of gender disaggregated data using routine HMIS and to undertake analysis of routine data to provide an improved understanding of health services outputs for gender and age. Furthermore, it is expected that the findings from this exploratory study will provide useful information for the preparation of HSSP II. Moreover, there are spin-offs that are anticipated such as exposure of the officers participating in the study to the usefulness of gender and age specific analysis ofroutine HMIS data. We present in this report some insights into the gender differences in health facility utilization in Uganda. Methodology The selection of districts took into consideration regional/geographical representation. Uganda has been previously stratified into four regions (North, South, East and West) and we randomly selected one district from each region by simple random sampling (SRS). Consideration was made of the ranking according to the Annual Health Sector Performance Report (AHSPR) league table (Ministry of Health 2003) with a view of understanding whether health systems performance might have an effect on gender and age specific equity. We did not make a deliberate effort to select districts according to the Human Development Index (HDI), although the latter is presented in the results and analysis is made as to whether it had any effect on gender and age specific equity. In each district, different levels of facilities were selected (hospital, HCIV, HCIII, HCII) by SRS, giving an average of one facility for each level for each of the four districts. The teams reviewed data from the outpatient department registers for the period of July 2003 to April 2004 and 2-3 months per facility were reviewed. OPD attendances were summarized by sex and age categories (<1, 1-4, 5-15, 15-64, >65). In order to provide technical support, ensure easy retrieval of data understand difficulties with data management and encourage improvement in recording, the review team worked with staff responsible for data management. Data were entered and analyzed in excel using proportions and male to female ratios to determine differences in OPD utilization. The male to female (M/F) ratio is presented on a logarithmic scale to highlight the differences in utilization be gender. Findings Coverage and scope of study We visited four districts and a total of 13 health facili-ties (see Tables 1 and 2) Table 1. List of the districts selected with the AHSPR league table and HDI ranking.
Table 2: Facilities Selected
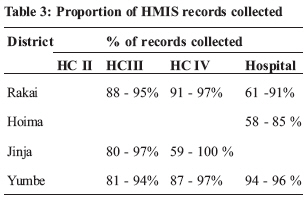
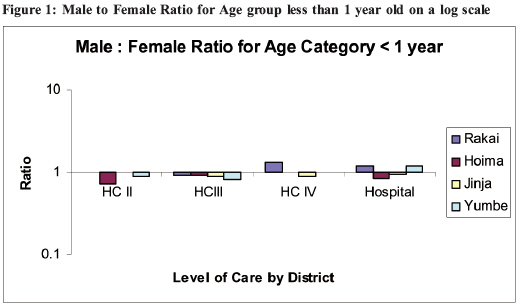
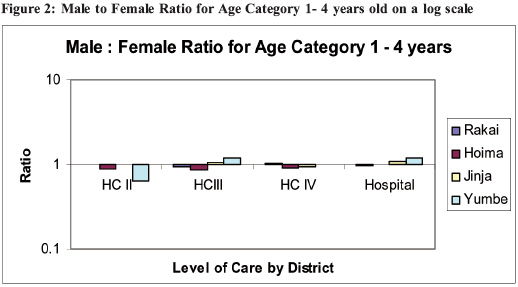
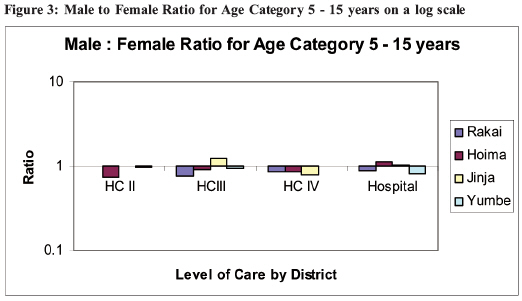
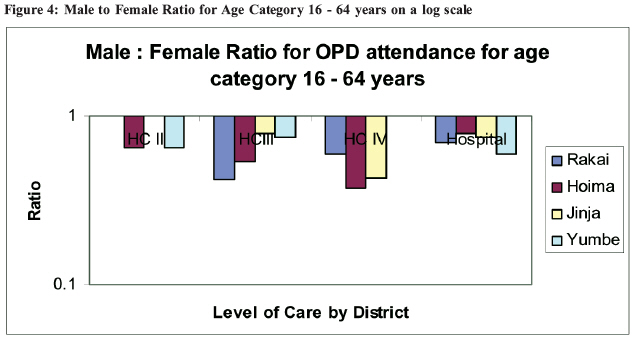
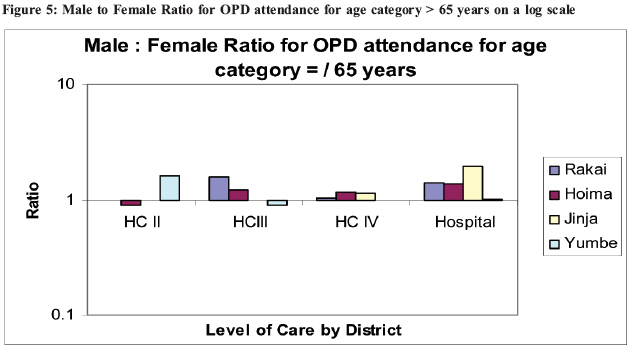
The data were easy to retrieve but the process was tedious and required at least one person day to collect information for a month in large facilities where monthly attendances exceed 6000. Retrieval required the presence of the records assistant and in facilities where these were not available at the time of the visit it was difficult for even the in charge of the facility to access records. Proportion of records analyzed out of those reviewed Records were available in all the facilities visited with the highest percentage of records that could be analyzed observed at HC IV level (Table 3). Overall, hospitals had the lowest records analyzed and the reasons cited for not analyzing all selected records included: absence of age and sex data and illegibility of hand-writing. Male to Female utilization ratio by age group This analysis was undertaken to determine the ratio of OPD attendance for male to female in the various age categories. The utilization rate for the age groups less than 1, 1-4 and 5-15 years was not different for males and females for all levels of health care (Figure 1, 2, 3). However, for the 16 - 64 age groups, more females than males attended health care services for all levels of care (Figures 4). In contrast for the age group above 65 years the utilization of health facilities for males was two fold higher than that for females at hospital level (Figure 5). Proportion of attendance compared to proportion in population (<1 and 1-4) The proportions in the general population for the age categories <1 and all those <5 are 5% and 23% respectively... In view of the fact that more morbidity is expected in these age categories compared to other age groups, each child should on average attend a health facility at least once a year. The purpose of this analysis was to understand whether there could be inequity in OPD attendance for the <5 age category. At all the levels the utilization rate per capita was above one in the age category, less that 1 year old, implying that at least each infant attended OPD more than once in a year. This does not rule out inequity given that the burden of illness could be higher i.e. each infant can be expected to have more than one episode requiring an OPD contact per year. Similarly, the OPD utiliza-tion per capita was approximately 1 in the 1-4 age categories and again as for the under-1 category might not rule out inequity. Table 3: Proportion of OPD attendance compared to % in population at HC III
Table 4: Proportion of OPD attendance compared to % in population at HC IV
Table 5: Proportion of OPD attendance compared to % in population at Hospital
Discussion In this exploratory study, we observed that females utilized health services more than males for the age group 15-64 years. This probably reflects the greater burden of morbidity that women in this age category face. The latter observation might not be conclusive that this is equitable since proportionally more women may be in need and not be accessing. On the other hand at very older age groups we observed that males were more likely to utilize health services, suggesting higher morbidity risk in males at old age. Surprisingly, there were no gender differences in utilization rates for the other age groups, suggesting equal risk of morbidity. A major limitation of our study is the small sample size, which should be taken into consideration when interpreting our findings. A priori we did not expect that the study would find conclusive evidence for gen-der and age specific inequity. Rather we postulated that the study would indicate the feasibility and usefulness of conducting such an analysis. We believe that this exploratory study has provided some lessons as to how gender analysis might be undertaken on a more regular basis and wider scale. Conclusions Based on our observations, we can make four conclusions.
Recommendations We recommend the following to be undertaken by the Ministry of Health
We acknowledge the contribution of Mr. Alex Mukundi for data collection and compilation, and Dr. Sarah Asiimwe and Mr. Amos Nzabanita for reviewing earlier drafts. Reference
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp05026f1.jpg] [hp05026f4.jpg] [hp05026t6.jpg] [hp05026t3.jpg] [hp05026f3.jpg] [hp05026t5.jpg] [hp05026t1.jpg] [hp05026f2.jpg] [hp05026t2.jpg] [hp05026t4.jpg] [hp05026f5.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}