 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
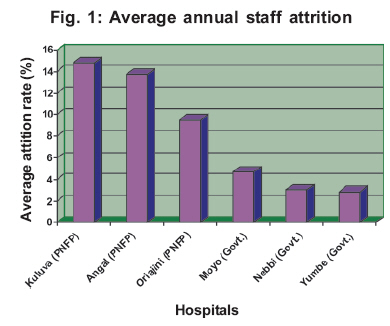
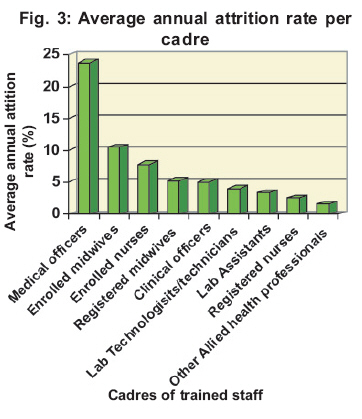
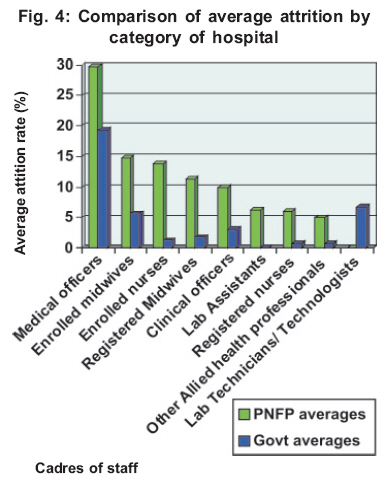
Health Policy and Development Journal, Vol. 5, No. 1, April, 2007, pp. 28-34 TURNOVER OF HEALTH PROFESSIONALS IN THE GENERALHOSPITALS IN WEST NILE REGION Onzubo Paul, Medical Superintendent, Nyapea Hospital- Nebbi District Code Number: hp07004 Abstract The imbalances in Human Resources for Health that result from health professionals crossing borders of districts, countries, and moving from private to public sectors and vice versa or leaving health services to join other non-health related business leads to inequity in delivery of health services, especially in the parts of the world that do not have sufficient incentives to attract these professionals. This Internal and international migration of health professionals has been noted with concern in the developing and more developed world though little information is available on the rates and reasons for the same. The study whose summary is presented here tried to compare the attrition rates in three Private Not For Profit and three Government General Hospitals in West Nile Region over a period of five years. It also examined the destination to which the health professionals were lost, the source of the new staff that replaced those lost by the hospitals, the reasons for attrition as perceived by the existing staff in the hospitals, what kept some of the staff working for longer period than others who chose to leave, and the incentives that were in place for attraction and retention of health professionals in these hospitals. The results and recommendations are as summarised in this article. Introduction “The quality of health services, their effectiveness, efficiency, accessibility and viability depend in the final analysis on the performance of those who deliver the services. The performance of these services is in turn, determined by the policies and practices directed towards guaranteeing that an adequate number of appropriately qualified and motivated staff are in the right place at the right time, at an affordable cost” (WHO, 2002). Many people will agree that human resources are the most important of all the resources needed for delivery of services in any sector, both in the developing and more developed world. The labour intensive nature of the health sector cannot be over emphasized. World Health Organization (2002) equally reaffirmed that Human Resources for Health (HRH) are central to managing and delivering health services. It has also been recognised that insufficient human resources for health in developing countries have been identified as one of the main constraints limiting initiatives for HIV/ AIDS control and the achievement of the Millennium Development Goals (WHO and CDC 2004). Globally, imbalances in the health workforce, partly influenced by the decision by these health professionals to migrate to parts of the world where incentives are better, tend to be influenced by a broad range of political, social, economic and professional factors, several of which are beyond the control of policy makers within the health sector (Vujicic et al, 2004). As a result, the health worker population ratio is better in the urban than the rural areas where health services are needed more in view of the poorer health indicators in the rural than urban areas. Many strategies that are developed and used to ensure equitable distribution of personnel are usually reactionary and in response to crisis. They are usually fragmented, uncoordinated, sometimes inconsistent and irrational, and rarely evaluated systematically (Wibulpolprasert (1999). Study Objectives This study determined the annual attrition rate of health professionals in the general hospitals in West Nile region in the five financial years (1999/2000 to 2003/04), established the destinations to which the health professionals were lost by the hospitals in question in the period under review, established the sources of staff that replaced the ones who left in the years under review, found out the reasons for attrition as perceived by the health professionals in the studied hospitals, established the reasons why some staff managed to serve for long in the hospitals under review and established the incentives in place for attraction and retention of staff in the hospitals under review. Methodology Six hospitals were sampled among the nine general hospitals in West Nile because of resource constraints in terms of time and funds for carrying out the study. Kuluva and Oriajini hospitals were selected purposively to represent hospitals that fall under the UPMB and UMMB respectively. Nebbi and Angal hospitals were also selected purposively for making a comparison of the turnover in a PNFP and a Govt hospital in the same district. Simple random sampling was applied to the other three Govt owned general hospitals of Yumbe, Moyo and Adjumani in order to get the remaining two hospitals to be studied. This resulted into Moyo and Yumbe hospitals being added to the other four hospitals that were purposively selected. Staff records covering a period of five years from 2000/2001 to 2004/2005 were reviewed in order to determine attrition rates, destinations to which the staff were lost and the sources of the new staff. A total of 184 respondents were interviewed in the sampled hospitals. Probability proportional to size sampling was used to obtain the number per cadre in each of the studied hospitals. Hospital core managers and representatives of staff that had served for at least ten years in the studied hospitals were interviewed as key informants. Results The annual attrition rate was found to be higher in the PNFP than the Govt hospitals as shown in figure 1 below. It can be seen in figure 1 that Kuluva had the highest average annual attrition rate among the PNFP hospitals, while Moyo had the highest among the Govt hospitals. Figure 2 shows that the attrition rates of health professionals were higher among the PNFP hospitals than the Govt ones and fluctuated over the years. The peaks of attrition were related with the existence of job opportunities with Central Govt, Districts and operating NGOs within and outside the region of West Nile. Analysis of the data also showed the highest rate of attrition to be among medical officers (doctors). The average annual attrition rates of the different cadres of staff are shown in figures 3 and 4 below. The above graph (fig.3) shows that the average annual attrition rate was highest among the medical officers, followed by the enrolled midwives. The lowest attrition rate was among the other allied health professionals. Figure 4 shows that the average annual attrition rates were highest among medical officers, both in the PNFP and Govt hospitals. It also looks clear that with exception of Lab Technicians/technologists, the average annual attrition rates were higher among PNFP hospital staff than the Govt ones. Moreover, further analysis showed that the losses of the lab staff in the Govt hospitals were mainly due to retirement. Destinations to which the staff were lost: The data showed that 85 trained staff left the PNFP hospitals compared with 31 in government hospitals during the period under review. The losses to the different destinations are shown in table 5 below. The data show that most staff were lost to government units either for better pay (PNFP staff) or transfer (Government staff). Sources of the replacements The PNFP hospitals lost more staff but attracted fewer replacements over the reviewed period than the Govt hospitals as shown in table 6. Table 6: Comparison of losses and replacement in the PNFP and Govt. hospitals in the five-year period:
It can be seen from the table above that the resultant effect of staff turnover was a reduction in numbers in the PNFP hospitals, while the Govt hospitals had a rise in staff numbers. Sources of the new staff The numbers and the percentages of staff obtained from various institutions as replacements are as presented in table 7. Table 5: Destinations to which the staff were lost:
Table 7: Sources of the new staff
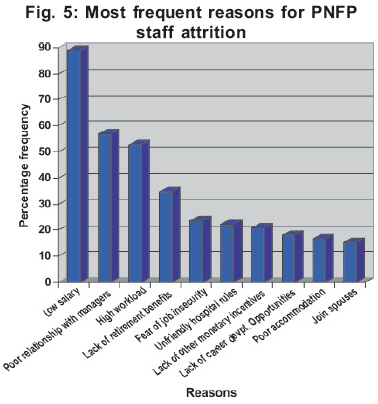
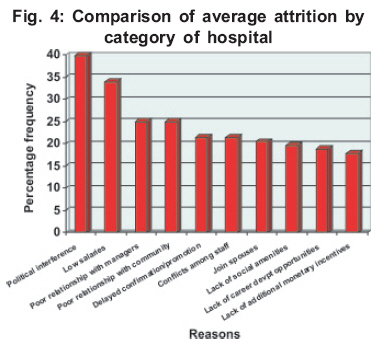
The PNFP hospital replacements from Govt were secondments by the Local Governments or Central Govt. The other NGOs from which replacements were obtained were mainly private pharmacies, drug shops and clinics that offer less attractive terms and conditions of service than even the PNFP hospitals. Reasons for attrition The ten most frequent reasons given for attrition are as shown in figures 5 and 6. Figure 5 shows that the most frequent reasons for attrition are related to poor conditions of service, especially remuneration and poor relationship between the staff and the managers. As an example, 88.9% of respondents in the PNFP hospitals gave low salaries as one of the reasons why staff tend to leave. Many other reasons were given for attrition that did not feature frequently and are not mentioned in this article. Much as in the Govt hospitals the reasons for attrition were slightly different from those in the PNFP hospitals as shown in figure 6 above, the majority of the issues reflect poor human resource management by either the hospital managers or the district leaders. Respondents that gave persecution by district leaders and community members as a reason for attrition were mainly from two of the studied Govt Hospitals. The issue of witchcraft was unique to one hospital. The ‘son of the soil’ syndrome (where local leaders prefer to employ staff born in that particular area) was also reported in the two hospitals in which persecution was of concern. Religion as a factor featured prominently in two PNFP hospitals and one Govt hospital. In the affected hospitals it seemed that other religious denomination members felt unsafe and would be denied key positions irrespective of their qualifications and performance. The issue of poor relationship with the hospital managers was reported in all hospitals. Reasons for long service The respondents who had served the hospitals in question for at least four years gave varied reasons for not having left, as shown in figure 7 below in order of frequency. A part from limited access to transfer of services from one district to another that was specific to Govt hospitals the rest of the reasons for long service indicated in figure 7 were similar in the PNFP and Govt hospitals. From the graph it can be seen that the majority of the reasons are family and social reasons as opposed to those related to health systems organization. The minimum flexibility in transfer of service in the decentralised system of governance reduced the attrition of staff in the Govt hospitals. This factor together with lack of other job opportunities contributed greatly to the reduced attrition of staff in the Govt hospitals. Incentives in place for attraction and retention of staff The commonly reported list of incentives included the free accommodation, payment of rent for workers not accommodated in the hospitals quarters, free water, free electricity, free treatment for the staff, their spouses, young children and very close relatives, access to institutional transport facilities, sponsorship for further training, meeting of burial expenses of very close relatives, and salary top ups especially for Medical Officers. Both the PNFP and Govt hospital managers mentioned the above listed incentives. The difference was that the PNFP hospitals were able to pay rent for staff not accommodated in the staff quarters, a situation not practised in the Govt hospitals. Results from Key Informant Interviews Most of the key informants agreed with what the respondents had said except that some of the managers disagreed with the presence of poor relationship with staff though the key informants who were staff members reaffirmed this.
Conclusions The attrition rates of health professionals are high especially in the PNFP hospitals, and tend to worsen with Public Service job advertisements. The peaks of attrition occur during periods of job advertisements by the Central and Local Governments as well as the NGOs and tend to be highest among the medical officers. Govt hospitals lose less staff but attract more and the converse tends to happen in the PNFP hospitals. Both categories of hospitals get replacements mainly from training institutions and this impacts on the quality of services in terms of the skills needed for service delivery. The reasons for attrition are diverse and can be political, social, economic or professional varying from one hospital to another. However, the reasons for PNFP hospital staff attrition mainly look economic, relating to the low payment, while the issues in Govt hospitals are mainly political and managerial. Better human resource management by the hospital managers and the district leaders could offer solutions to many of the reasons that generate intentions to migrate. Many employees would love to leave to go and work elsewhere if only job opportunities exist or there is ease of transfer of service from one district to another. The management of the hospitals seem not to see value in communicating to the employees about the monetary value of what the hospitals provide as additional incentives. Recommendations The Ministry of Health together with the Relevant Line Ministries need to do the following:
The Umbrella Organizations (UCMB, UPMB and UMMB) and the Boards of Governors of the PNFP hospitals need to do the following if the attrition rates are to reduce in the hospitals in question:
The District leadership could do the following in order to reduce attrition:
References
Copyright 2007 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp07004f7.jpg] [hp07004f1.jpg] [hp07004f6.jpg] [hp07004f5.jpg] [hp07004f3.jpg] [hp07004f4.jpg] [hp07004f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}