 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 5, No. 1, April, 2007, pp. 35-47 THEME TWO: PUBLIC PRIVATE PARTNERSHIP FUNDING MECHANISMS FOR THE 'PRIVATE-NOT-FOR-PROFIT' HEALTH TRAINING INSTITUTIONS IN UGANDA John F. Mugisha, Everd Maniple - Uganda Martyrs University, Senga K. Pemba, Peter Petit - Developing Human Resources for Health. Code Number: hp07005 Abstract The Health Sector Strategic Plan (HSSP) aims to ensure access to basic health care by the Ugandan population through the delivery of the National Minimum Health Care Package (NMHCP). This requires availability of well-trained health professionals. This study demonstrates that the Private-Not-For-Profit (PNFP) Health Training Institutions - the majority in Uganda - have remained grossly under-funded, which poses a threat to achievement of the HSSP. They are faced with decreasing income from fees, dwindling donor support and over-dependence on government grants which are both uncertain and erratic. Consequently, vital activities for students' training such as field trips, teaching and reading materials are left unsatisfied as a copying mechanism, but not without negative implications for quality. It is recommended that government increases and guarantees its support to these Health Training Institutions as a way of maintaining quality of health worker training. At the same time, the training institutions need to diversify their funding options to include designing short tailor-made courses, mobilizing alumni contributions, research and consultancies, self-help projects like farming, canteens and stationeries as well as fund-raising activities as a way of bridging their funding gap. This should be coupled with more efficiency mechanisms and prudent management to avoid wastage of the already scarce financial resources. Introduction The Uganda National Health Policy (NHP) through its enabling framework, the Health Sector Strategic Plan (HSSP), aims to ensure access to basic health care by the Ugandan population through the delivery of the National Minimum Health Care Package (NMHCP). The HSSP recognises that achievement of this policy goal requires availability of well-trained health professionals. The policy further recognises that the health sector is faced with serious human resource shortage. No wonder, the minimum staffing norms were defined and the target set at 75% by the end of HSSP period 1 in June 2005. Yet, according a human resource inventory undertaken in October 2003, only 67% of the approved posts had been filled (MoH, 2004). One of the seriously required cadres were the nurses. Most of the Nurses’ Training Institutions, however, are Private-Not-For-Profit whose funding mechanisms were not well established. This paper is a result of a study that was commissioned by the Developing Human Resources for Health (DHRH) to assess the funding mechanisms for the PNFP health training institutions in Uganda with a view to proposing alternative funding strategies that could ensure sustainable levels of income needed for continuous production of well trained health workers by the PNFP sub-sector. The paper is divided into four parts. Part one outlines the background information about the PNFP health training schools, the rationale for this study, the study objectives and methodology. Part two analyses the existing funding mechanisms for the PNFP health training schools, areas of expenditure, management of funds and ends by assessing the funding gap. Part three proposes general alternative funding mechanisms for the PNFP health training institutions and discusses their method of operation. Part four summarises the major conclusions from this study and outlines recommendations for action. The Government of Uganda and the European Union under the 8th European Development Fund (EDF) support the Ministry of Health (MoH) and Ministry of Education and Sports (MoES) in the development of human resources for the health sector in Uganda. To achieve this goal a five-year project targeted towards developing human resources for health (DHRH) was established in November 2003 to oversee the implementation of various HRH related issues. The goal of the DHRH project is to contribute to improved status of the Ugandan population by supporting the development and maintenance of a well-trained, motivated health sector workforce deployed and managed to meet the needs of Uganda. To achieve this objective the project has endeavoured to develop HRH planning, management and training capacity to meet the needs of Uganda within the health sector resource envelope in line with the National Health Policy and the Health Sector Strategic Plan (HSSP). Some of the results which the Project aims to achieve include having a strengthened capacity for HRH policy development, planning and management at various levels, a developed HRH Training and Management capacity in line with health policy requirements and Up-graded physical infrastructure and equipment in selected health training schools to enable PHC staff to deliver the minimum health care package in line with health policies and strategies. It was against this background that the DHRH project commissioned this study. PNFP health training institutions The PNFP health training institutions, a majority of which are nurse training schools (NTS), were started by PNFP Hospital Boards to help in the fulfillment of hospitals’ mission to provide the necessary professional profile of human resources and to secure a practice-oriented professional education. The PNFP hospitals actually pioneered the training for professional nursing in Uganda when in 1918; Mengo hospital opened a school of nursing and midwifery (MoES, MoH 2002). Like the majority of the PNFP hospitals, most PNFP NTS are located in remote areas. With their mission of providing quality services to all, but preferentially targeting the poor, the religious faiths located their hospitals in rural and remote areas. Later, they were faced with the need for qualified nursing staff ready to serve in these remote and rural areas. The hospitals therefore established their own nurse training schools. Today, the PNFP nurse training schools remain the majority in professional nurse training in Uganda (18 out of a total of 30 schools). Over 60% of the annual output of new nurses and midwives come from PNFP schools. Most recent studies also indicate that their students have better performance in terms of final examination results compared to government institutions, which are usually better resourced (MoH, 2004). The mission of the PNFP health training institutions has been summarized by the health commission task force of the Uganda Episcopal Conference thus: To train an optimal range of health care staff of high moral and professional standard for the PNFP and national health care institutions (UEC Health commission, 2005). The PNFP health training institutions have a different organisational structure from their government-owned counterparts. Unlike the latter, which have separate boards, the PNFP NTS share the same boards with their mother hospitals. Indeed, they also share the management. Training is inherent in the mission of the PNFP hospitals therefore PNFP NTS have always been part and parcel of the hospitals. Rationale for the study The pattern of demand for Human Resource in the Health Sector in Uganda has dramatically changed over the years. This has necessitated a review of how training of human resources for health can effectively be financed. Currently, resources on the part of government to finance health-training institutions have remained unconvincingly insufficient and biased to public training institutions only. At the same time, the emergent public/private partnership has not been representative in financing training in the private sector. This situation has led to visible inadequacies in the training institutions under the PNFP sub-sector. For instance, most PNFP health training institutions had reported that they were finding it difficult to effectively implement their training curricula especially the field-work component. The impact of this inefficiency was greatly felt by the students and ultimately the community. This study was deemed necessary to help identify key financing issues and propose alternative and complimentary financing options for the PNFP Health training institutions in Uganda. Objectives of the study The overall objective of this study was to identify the funding options for the PNFP health training institutions in Uganda, establish their funding gaps and develop a proposal for their alternative funding mechanisms. Specifically, the study sought to:
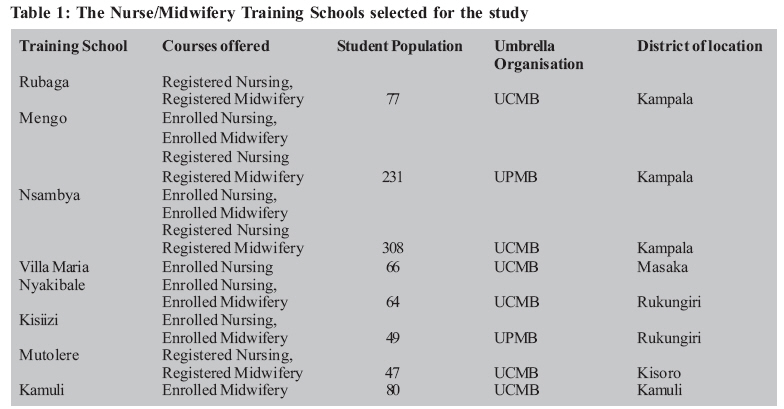
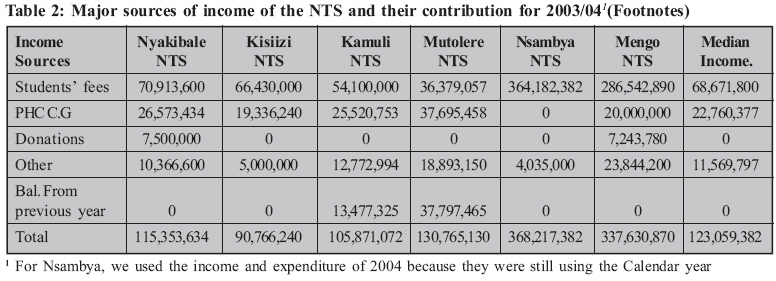
Methodology and design It was a cross-sectional survey, which utilized both qualitative and quantitative research methods. Through a highly consultative process, qualitative methods were used to conduct key-informant interviews with various key stakeholders. Quantitative techniques were also used to collect data on funding sources and expenditures and to determine the variance between budget estimates and actual revenue. Data was collected through review of documents such as budgets, receipt books, payment vouchers and other source documents that verify transactions, major books of accounts – cash book, ledger and vote book, financial and annual reports, staff lists, and students’ enrolment registers. A checklist was used to get the data on variables such as sources of funds, trends in the flow of funding, expenditure items, staff on the school and hospital pay rolls, variance between income budgeted for and actually realised and the planned activities that suffer when the needed revenue was not all realised. Interviews were also conducted with the main stakeholders - officials from the religious medical bureaus, MoES, MoH and the management teams of the hospitals and the training schools themselves. Semi-structured, interviewer-administered questionnaires were used to obtain data on problems related to the current financing options, suggestions on possible solutions, cost containment strategies, proposals for alternative sources of financing and opinions on the merits and demerits of keeping separate school accounts. Observation of things like school library, students’ hostels, learning materials, income generating projects, machinery and equipment for information and communication – computers, beamers, photocopiers, projectors etc. was done to corroborate the information got through documents and interviewing. The sample was picked only from the nursing schools because they form majority (75%) of the PNFP health training institutions in Uganda. In all, there are 24 PNFP health-training institutions (MoH, 2004). The rest of the PNFP HTI which are medical laboratory, theatre and ultra-sound technology schools were reported to be so financially fused with the hospitals that it would be hard to tease out their separate income sources and expenditure which would make it difficult to achieve the objectives of this study. Eight Nurses/ midwifery training schools which form 44% of all the PNFP NTS in Uganda were purposively selected. These were the schools with known separate financial records from their parent hospitals. Pre-contacts with schools and the umbrella organisations were made to determine this. The selected Nurse training schools are shown in the following table 1: The table shows variability in students’ enrolment among the different schools. We did not do a correlation but prima-facie observation of the table suggests i) a relationship between students’ enrolment and proximity to Kampala city and ii) a relationship between enrolment and the number of courses offered by a school. Existing Funding Structure of the NT Schools The sources of funds for the schools The schools generally were found to have limited sources of funding. We categorised them into four -Students’ fees, Primary Health Care Conditional Grant (PHC C.G), External donations, Balance from previous year and Others (which includes revenues from activities like school canteen, photocopying services, hospital contributions etc. The contributions from these sources are summarised in the following table. (Table 2) The above table shows wide variations in the amounts collected by the schools from the afore-mentioned categories of sources. For the 2003/04 financial year, the range in income from students’ fees was very big, amounting to Ush. 327, 804,325 while for the PHC C.G, the range was Ush. 37,695,458. It should be noted that the PHC C.G. meant for some NTS had been used by the hospitals because of the fused financial management system and lack of a visible, clear-cut boundary between the two institutions administratively. If one excluded Nsambya and Mengo NTS, the range for income from the students’ fees would narrow down to Ush. 34,534,543 only. Because of this variability, we calculated the median to get figures with a more central tendency in the contributions from different sources. Hence, generally, the median contribution of students’ fees was Ush. 68,671,800, from the PHC C.G it was Ush. 22,760,377 while from other sources, it was Ush. 11,569,797. It is interesting to note that external donations and the balance from the previous year disappear completely when you look at medians. This is because they apply to only two hospitals and have no statistical significance to the bigger picture, as their median percentage contribution is zero. However, they have a financial significance to the extent that they expose the limitedness of the scope of the funding sources for the PNFP nurse training schools. Only 2 out of 8 schools had received external donations that were valued in money terms. The table above clearly shows that students’ fees were the dominant income source for the NTS, followed by the PHC C.G. What appears as balance from the previous year was not in any way a surplus but fees paid in advance by students who were admitted in May, close to the end of the financial year which ends in June every year. A few sponsored students also had paid fees for the whole course of two and a half years which had all been recorded as income for one year. This exaggerated the income for 2003/04 financial year to appear higher than expenditure. Our main observations about the income sources of various schools were that:
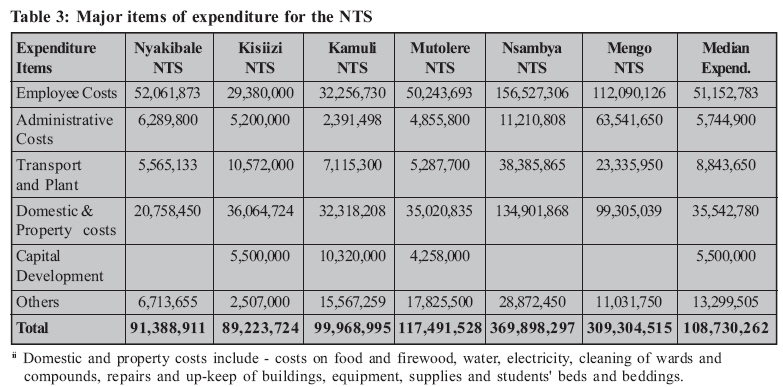
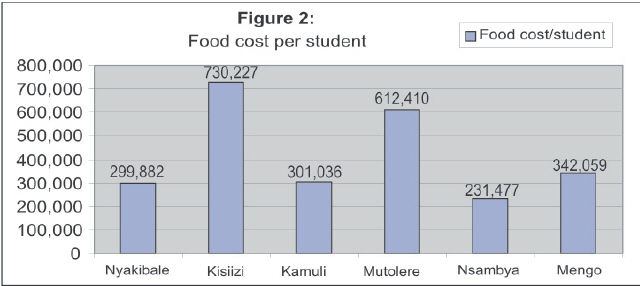
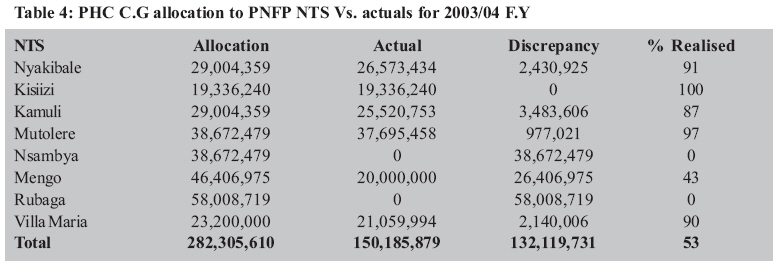
Major items of expenditure We categorized expenditure of the schools into 5 main items - employee costs, administrative costs, transport and plant costs, domestic and property costs, capital development costs and others. The following table shows details of each expenditure item for the financial year 2003/04 and for Nsambya 2004, since they still used the calendar year as their financial year. (Table 3) Like their income, the schools’ expenditure also indicated variability in the costs incurred by different schools. The range was widest for the employee costs at Ush. 127,147,306 followed by domestic and property costs2 at Ush. 114,143,418. This range would narrow down to only Ush. 23,861,873 for employee costs and 15,306,274 for domestic and property costs if we excluded Nsambya and Mengo, which are outliers. The median expenditure was highest for the employee costs at Ush. 51,152,783 and lowest for capital development costs at Ush. 5,500,000 only. We investigated the reasons for wide variation in employee costs and established that schools with lower costs relied more on relatively less qualified staff. They benefited more from staff volunteers working in the hospitals who acted as clinical instructors. In fact, one school had an enrolled nurse as a clinical instructor. They also incurred less costs on staff training (refresher courses), staff transport and welfare. The available records did not allow us to compare expenditures by specific items. For some schools, expenditures were very generalised. However, we noted that wide variations in expenditure could not only be justified by the differences in location and size. Analysis of the total recurrent cost per student in different schools would help to demonstrate this. The analysis below shows rural schools - Mutolere and Kisiizi as incurring the higher recurrent expenditure per student compared to other schools. The two are located in rural areas where the cost of living should be lower compared to the schools located in towns. However, these also are the schools with the lowest student enrolment of 47 and 49 respectively as against 308 and 231 for Nsambya and Mengo, which are located in Kampala city. It is such poor enrolment that increases their average cost since they incur almost the same fixed costs with the rest. We picked on one expenditure item and assessed its cost per student in different schools to compare financial efficiency. The following figure provides a summary of the analysis: Yet, the figures shown in the graph above are an understatement of the real costs. The actual costs should have included other things like salaries and allowances for cooks, costs for kitchen utensils, maintenance costs for the kitchen and kitchen store etcetera. Without addressing such costs, one would not reasonably compare cooking for students with, for instance, contracting out of the feeding services. Again, rural schools were found to incur much higher costs than their counterparts located in the city. Management of funds Resources are never enough. The recent policy for all nurse training schools to train comprehensive nurses requires a lot more funding than is assured. The importance of managing the available funds carefully, skilfully and honestly cannot be overemphasised. Scarce resources need prudent management to help in achievement of meaningful results. We looked at the budgets, source documents that verify financial transactions, essential books of account and financial reports/statements. We found out that all the 8 NTS possessed key financial records either at the school or the hospital, namely Annual budgets, Cash analysis book, Vote book, Ledger book, and vital source documents that verify financial transactions - receipts, payment vouchers, requisition and issue vouchers and bank statements. Two schools lacked income and expenditure statements for 2003/ 04; and only three schools had a standard budget in a self explanatory and informative format. Yet, while availability of financial records is good, it is never sufficient. The whole system of transacting business – who initiates the expenditure, who approves it, who controls the money etc. – is equally important. We therefore investigated the management of finances and found varying systems in the different schools. While all the 8 schools had separate bank accounts, only 3 of them had bank accounts for all their funds. The rest were allowed to collect only the school fees. In two schools, the principal tutors of the schools could not originate the expenditure. Even for the rest who could, some expenses in the school budget could be incurred by the hospital without their knowledge. Only in 4 schools were school authorities allowed to keep imprest fund. The rest had to run to the hospital authorities even for small and emergency expenditures. Financial gaps There are three common methods of establishing financial gaps of every institution: the gap between revenue and expenditure, which shows whether an institution went into debts, the gap between budgeted revenue and the actual revenue, which shows whether all the expected funds were realised, or the value of activities that remain unimplemented due to shortage of funding. The method of book keeping used in the NTS did not allow us to establish the gap between revenue and expenditure. Majority of the schools recorded all the received cash as income including advance fees payments, which would be used in the subsequent year. It needs mention that some students would pay fees for the entire course but it would be recorded as income for the current year, exaggerating the annual income to appear higher than expenditure. Given that income from students’ fees and external donations was erratic, we analysed the PHC C.G which is relatively more stable. The following table summarises the schools’ allocation for 2003/04, the actuals and the discrepancy. (Table 4) On the whole, PHC C.G funding was still low. For all the 8 NTS, only Ush. 150,185,879 was realised instead of 282,305,610, a mere 53% of the allocated amount. If we divide this by the student population of 900, government support per each student nurse was only Ush. 166,873. Thus government contributed a paltry 16% of the average fees paid by a student nurse, which was estimated at Ush. 1,000,000 (UEC Health Commission, 2005) Activities that suffer due to insufficient funding We established that budgeting was made on the basis of the expected income rather than the need. The income and expenditure approach, therefore, could not present an accurate picture of the financing gap. We therefore investigated the activities that suffer due to insufficient funding. We were not able to cost these activities in the limited time available. The gaps were identified in the following areas:
Strategies employed to address the gaps
Alternative Funding Options The schools generally had limited funding options, which also varied from one school to the other. We investigated the existing options, their strengths and weakness. Basing on our own rapid field assessment of the training schools and the suggestions we gathered through the key informant interviews, we also proposed other funding options and how they could be operationalised, highlighting their opportunities and constraints: Students’ fees Income from the students’ fees, on average, contributes about 60% of operational revenue for the schools. The percentage contribution is relatively higher in the schools located in Kampala because of bigger student numbers. The increase in entry requirements for nurse training by the Nursing Council in 2003 led to an abrupt drop in student enrolment, hence also fees revenue. High school fees present an access obstacle to candidates from the rural areas where most PNFP health training institutions are located. Attracting international students and students from urban areas would have human resource implications as these are unlikely to remain and serve in the rural health facilities (MoH, 2004). Yet, the international students were reported to be the biggest fees defaulters. We suggest that schools plan for fixed student numbers to avoid enrolment fluctuations, which in turn affects planning for and use of income from fees. We also suggest that a system of fees payment be put in place to match the financial years for proper planning. The fees which exceed the fraction for the given year should be recorded as ‘advance payments’. The balance sheet should clearly reflect advance payments as a liability to the school for a particular financial year. This will help to avoid deceptive financial surpluses in the income and expenditure statements of some schools. PHC conditional grant The PHC C.G, for most schools, has been the only stable source of income since its inception in 1999/ 2000, especially for the schools in rural areas. It is clear what the PHC C.G funds can be used for so that schools are able to plan and budget accordingly. For some schools, this is the only revenue for which they have a Bank account since the cheque is written in the school names. It is therefore the only money directly controlled by the schools. However, this grant still requires the schools to negotiate with districts to agree on activities that they want to carry out. For some districts, the cheque for the school is written in the names of the hospital and because of the fused nature of budgeting and financial management; schools end up not accessing the funds. The management of schools were not happy with the failure to control these funds directly. At the same time, the PHC CG for training schools is not a guaranteed source of revenue because it comes from the MoH whereas the schools are currently under the MoES. In case the MoH decided to withdraw this support, there would be a crisis because the records indicate that the MoES did not yet have a budget for the health training schools (UEC Health commission, 2005). It is further noted that while PHC C.G under the MoH was protected because it was part of the poverty action funds (PAF), the poverty action funds under the MoES included only the money for universal primary education (UPE). Therefore, money for HTI even if budgeted for could still be diverted. The future of funding, (and real survival) of the PNFP NTS depends on quick steps by the MoES to include it in its planning and make a budget provision for it. This in turn depends on the strength of the partnership between the MoES and the PNFP health training institutions. The public-private-partnership in health (PPP-H) that has made the support from MoH possible is relatively new to the MoES. The MoES is used to a different form of partnership with government-aided schools, which involves government more in their management. The HTI could easily find this arrangement difficult because of mission considerations and the nature of health training. For instance, who takes liability in case a nurse student injured a patient resulting into litigation, if MoES was involved in governance? There is need for the two sides to streamline this partnership. We propose that the coordinating medical bureaus continue lobbying on behalf of the PNFP NTS for clarification of partnership with government under the MoES and also for the retention and increment of the PHC C.G especially given the need for increased funding that will be necessitated by the recent policy on comprehensive nurse training. External donations The donor funds contribute 80% – 100% of capital development expenditure of most nurse training schools. These are free grants that are not to be paid back. They are secured after writing proposals and submitting them to the organisations that fund social activities. Other donors were accessed through the respective dioceses, old foreign staff and the coordinating medical bureaus. Since many of external donations are made in-kind, they are not easily diverted or misappropriated. The donor funds are given mainly in-kind or tagged to specific capital outputs. This makes them less flexible. Donor funds thus may not help the schools to buy students’ food during food shortage or finance students’ field trips, which may be the immediate problems. Nevertheless, they can cater for other needs freeing money for recurrent costs. Donor project aid is also rapidly reducing in Uganda because of the sector-wide approach (SWAP) and the shift in donor funding to national budget support. It is scarcely surprising that many schools did not have any revenue from external donations. Health training schools need to be vigorous and proactive in mobilization of donor funds. They need to write project proposals to solicit for this funding. They will obviously require skills in project proposal writing and accounting for project funds since external donations require transparency, timely and accurate accountability. Schools also need to market themselves and make different organizations more aware of the activities they carry out. Hospital contribution Hospitals obviously contribute to the running of the training schools. Unfortunately, this contribution is not, in all training schools, valued in monetary terms. Some schools had included an estimated amount into their budgets as contribution from the hospital but there is a possibility that this was an under-estimate, as there are numerous in-kind exchanges between the hospital and the school that may not be easily captured. The insistence by some hospitals to have joint financial recording and reporting with training schools does not help this. As a result, some key informants thought that some hospitals were instead over-depending on their training schools. In one school, the management board had ordered the hospital to refund money to the school, also failing to appreciate the inter-twined nature of the two institutions. We suggest that schools and hospitals prepare and maintain distinct financial records. An attempt should be made to capture and value all the assistance that comes from the hospital to the school and vice-versa. The schools should keep accounting to the hospital and function as a cost centre within the hospital. While the hospitals assist the school, the finalist nurse trainees or those up-grading also work on the wards to beef up hospital staff. This close collaboration should continue to exist and all efforts made to keep the relationship cordial and symbiotic. Conducting short courses The PNFP nursing schools could organise short training courses as a means of earning more revenue. Mutolere had done it after working out an arrangement with Kabale Diocese to do refresher training for all the staff in the Diocesan health units. Consequently, the school realised Ush. 16.5 millions. Many PNFP schools were also reported to be under-utilized, therefore short training courses, which are tailor-made, could help to ensure their full staff utilization. Fortunately, the schools already have the space and teaching facilities for such courses. However, there is still a tendency of only looking at the traditional roles of giving mainly pre-service training. Some schools also have few qualified tutors who may fail to get time to run such courses. The schools need to jump out of their traditional teaching domain. They should organise and market short tailor-made courses to be conducted, for instance, during students’ holidays. They also could lobby with the MoH and district directors of health services (DDHS) to run refresher courses for the staff already in service. The medical bureaus could also participate in this lobbying on behalf of their training schools. Hiring of school facilities Nearly all the health-training institutions have facilities that could be hired out for a fee to boost the income. Such facilities include halls that could be used for weddings and other social functions especially on weekends, accommodation for seminars etc. however, some of the school facilities especially the physical infrastructure needs to be first renovated before they could be attractive to the outside customers. The schools may also lack skills to market themselves for this kind of business. The schools will need to devise strategies to market themselves locally and nationally, if possible even internationally. They also need to lobby with big non-governmental organisations and government departments such as health and education, which usually organise workshops and seminars. Then they can assign one staff member to be responsible for management of such functions who can report to the principal tutor. Running school canteens Some schools already run canteens, which they stock with materials that are likely to be consumed by the students. The canteens need not necessarily be situated within the school compound. They could be outside to target outside market especially for those schools that are located within towns. We also found out from one of the schools that students prefer buying things from outside the school fence so as to have a feel of different atmosphere. Canteens will require hiring a trustworthy full time employee. The schools may only be having structures within their premises and not outside which restricts them to only the internal market. The school needs to hire an employee to run the canteen or get one non-teaching staff member to run it in addition to other duties depending on its location. If its near the administration block, an office attendant could run it or if its near the kitchen, the food clerk or kitchen supervisor cook also run it. Alternatively, the canteen could also be contracted out to avoid administrative problems so that the school gets money at once and leaves the contractor to run the day-today business. Farming projects Some key informants suggested farming as a possible income generating activity for the schools. The possible farming activities that schools could carry out include fruit and vegetable growing, poultry and piggery since they do not require a lot of farm space. But they can also do other activities. For instance, Villa Maria NTS was already doing cattle keeping and it also had a banana plantation from which it was getting about Ush. 1,500,000 per year. Kamuli was farming in vegetables and cereals. These boosted students’ catering services. However, farming can be labour intensive and may require technical supervision skills, which most schools do not have. Besides, some PNFP schools do not have land at apart from their compound. The schools which have land need to learn from those already farming. They could recruit a qualified agricultural technician to manage their farming activities who can be supervised by either the principal tutor or any of the senior members of staff. Since most PNFP schools are located in rural areas, they could exploit the cheap labour in these areas. Fundraising Another possible way of mobilising funds is through fundraising activities. Schools could organise fundraising functions targeting a particular project such as renovation of buildings, construction of library or students’ hostel. Such fundraising functions usually realise funds that almost see the targeted projects to completion and are most ideal for capital development. However, schools will need to set aside some funds for use in mobilization, advertising and generally making preparation for the fundraising. Some projects also require to have been started on in order to attract charity. Schools could borrow from the students advance fees payment since some students tend to pay on a yearly rather than termly basis. They could use that money and reimburse it after the fundraising function. They need to involve more popular people such as the diocesan bishop, the area member of parliament or the local council chairperson to attract many people who could contribute. This is possible and has been done successfully by secondary schools. Hospital management boards could also help in organising this since they may be more popular. Soliciting for alumni contributions This has not been a source of funding for nurse training institutions. However, it has been a source for secondary schools where the alumni have organised associations of old students who usually come together to visit and help their former schools. In developed countries, the alumni contributions are said to contribute more than 5% of all education revenues (Kiwara A.D and Mujinja P.M, 2001). The alumni contributions will depend on their satisfaction with the management of their former institutions and how they will have been treated while still there. Many alumni of NTS do not earn enough to enable them spare some to give away. However, they are many enough to raise huge sums of money with little individual contributions because most PNFP NTS have been in existence for many year. The success of mobilising the alumni contributions will depend on the ability of the training institutions to track all their old students. An advert could be made asking all the alumni to register themselves. Alumni could also be invited to some functions by radio announcements. It is also possible to use some old students to track others. The old students could be encouraged to form associations so that new alumni could easily join, after completion of their studies. Bookshops and stationery shops Bookshops and stationeries are another income generating business that HTI could engage in. These have an advantage of not requiring huge amounts of money for capital; they do not involve high running costs and can stock only the items that students and staff will buy. The schools themselves could provide market to their own stationeries hence retaining the funds spent on purchase of stationary elsewhere. Unfortunately, many health workers lack skills even for small businesses. Managers of HTI are not any exception. Book shops and stationeries are affordable since they require little capital which the schools can mobilise. They could also arrange to buy the initial stock on credit from the big stationeries and bookshops, targeting the opening of the students’ semester when a number of items can be sold off. Then they can pay back. The HTI that already have Bursars could utilise their business skills to supervise such projects. Consultancy and Technical Assistance Consultancy services have been identified as another potential source of revenue for HTI. Kiwara A.D and Mujinja PM (2001) have argued that some of these HTI have staff members who have both academic and practical skills, and are very competent in their areas of specialisation. Some have specialist staff in medical education, public health nursing, vector control, health planning and management. They could provide services in these areas at a fee to both the public and private institutions either as institutions or through their individual members of staff. However, due to serious understaffing, most schools suffer a heavy workload. Besides, health professionals generally lack self-marketing skills to advertise even what they can do best. They have known health not to be a consumption good that can be subjected to market forces. Health Training Institutions will need to organise workshops on consultancy skills for their staff to enable them gain competencies and confidence in this area. They can then lobby with Ministry of Health, Local Governments and Medical Bureaus to provide Technical Assistance (TA) to the rural health facilities in form of ‘on-the-job training’ in various fields and support supervision, all of which are avenues for income generation. Conclusions The NTS had a narrow resource base with limited sources of funding. They relied mainly on students’ fees and PHC C.G although very few NTS also receive external donations and some benefited projects. The sources of funding were generally erratic. This limits predictability, which is a prerequisite for good planning.The students’ fees as a source of income could not be increased due high poverty levels still prevalent in Uganda, especially in rural areas where the majority of the PNFP NTS are located. External donations as a source of funding were likely to reduce further due to a shift from donor project support to sector-wide approach as a financing strategy for the health sector. The future of government support to PNFP HTI was uncertain. There was a possibility of MoH scraping the grant to the PNFP HTI as they had been transferred to MoES. Unfortunately, the MoES had not attached the same importance to the PNFP HTI as did the MoH, which was proved by the fact that it had so far failed to plan or budget for them. The attempts by the schools to undertake cost minimisation and other copying strategies like early closure of the semester, reduction of food to students, reduction in the number of students’ field trips and sharing of limited learning and teaching materials could easily compromise the quality of training. Several activities in the NTS were left undone due to insufficient funding, which also affected the quality of teaching namely: recruitment of the required staff numbers, necessary students’ field trips, required text books, basic ICT equipment, transport facilities and teaching materials like flip charts and papers. Employee costs constituted one of the largest expenditure items for the PNFP NTS in spite of gross understaffing. Any improvements in staffing position would require additional funding. Government policy is currently not in favour of secondment of staff to the PNFP health institutions. This stance needs re-thinking, if the contribution of these HTI is to be maintained. The schools had the capacity to manage funds as proved by availability of basic financial records either in the schools or in the hospitals. They had the cash analysis book, the vote book; the ledger book and school annual budget estimates. Majority of them also had income and expenditure statements as well as source documents – receipts, payment vouchers, bank statements and requisition and issue vouchers. Recommendation As a matter of urgency, the Ministry of Education and Should plan to include financial support to PNFP health training schools in its budgeting and also to increase it. Short of this, the future of these school remains uncertain. Those PNF NTS which do not get any government funding needed to take initiatives to follow up this matter directly with their respective local governments (offices of the DDHS and the Chief Administrative Officer) and with the MoH since it was clear how much had been allocated to them. Umbrella organisations needed urgent negotiations with the MoES, the MoH and the National Council for Nurses and Midwives to devise means of meeting the financial needs created by the new policy on training comprehensive nurses. This was necessary especially given that government policy did not favour secondment of staff, which would have been a partial solution to the problem. The Ministries of Health and Education and Sports needed to ask all local governments to prepare cheques for PHC C.G for the PNFP NTS directly in the names of those schools, not the hospitals. They should also insist on a separate school accountability signed by the principal tutors, even if this would be attached to the bigger hospital accountability. The NTS should adopt a uniform format of financial reporting for all the funds they receive and use. It saves time and resources. This may necessitate negotiating with the different donors to accept this. The umbrella organisations could also help the schools in these negotiations by setting guidelines for financial reporting. The schools also needed to adopt a uniform system and method of budgeting, bookkeeping and financial reporting. This would enable them to learn from one another. It will also permit easy comparability and benchmarking. The umbrella organisation would help to provide the format. All NTS needed separate bank accounts for all the revenue meant for the school. Keeping school funds on the hospital bank account should be avoided as it creates temptations of encroaching on these funds for non-school activities. There should be no exceptions to this. The principal tutors should be the principal rather than alternate signatories. However, the hospital CEO would still first approve all school expenditures before they are incurred. While separate financial records should be kept by the NTS, amicable relations between the two institutions need to be maintained, promoted and reinforced as the two benefit from each other in ways that are difficult to value in money terms. Keeping them under the same management board is one effective way of ensuring this symbiosis. The PNP NTS need to consider diversifying the traditional funding mechanisms with other alternative funding options such as fundraising functions targeted at certain projects, mobilizing the alumni for contributions, hiring out school facilities for income, conducting short but tailor-made courses and initiating income generating activities such as farming and running school canteens as discussed before. Further research needs to be undertaken to cost the PNFP HTI and all their activities. This would shade better light on the actual unit cost of training one student nurse, the actual value of income generating activities, and the value of hospital contributions to the NTS. References
Copyright 2007 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp07005t3.jpg] [hp07005t2.jpg] [hp07005f2.jpg] [hp07005f1.jpg] [hp07005t1.jpg] [hp07005t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}