 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 5, No. 1, April, 2007, pp. 48-56 PUBLIC PRIVATE PARTNERSHIP FOR HEALTH IN UGANDA:WILL HSSP II DELIVER ON THE EXPECTATIONS? Christine Kirunga Tashobya1, Nelson Musoba2 and Peter Lochoro3 1 Public Health Advisor with the MOH/DANIDA Health Sector Programme Support and was the first PPPH Desk Officer Corresponding author: Dr. Christine Kirunga Tashobya, Ministry of Health, P.O Box 7272 Kampala, Uganda, e-mail: christine@hsps-ug.org Code Number: hp07006 Abstract At the inception of Uganda's second 5-year Health Sector Strategic Plan (HSSP II), this paper traces the history of the public - private partnership for health (PPPH) in Uganda, giving its justification and mandate. It also gives its current state of the art, outlining the successes scored, the challenges still faced in its implementation and current efforts being made to make it comprehensively institutionalized. The successes include the bilateral acceptance of the principle and need for partnership by both the public and private partners, the overt gestures by the public partner through direct funding of the private providers, the ceding of some responsibilities to private players, the acceptance by the private players to take on some public responsibilities using their own resources etc. The challenges include the slow formalization of the partnership, skepticism about autonomy, the stagnation of government funding, the poor understanding of the partnership at sub-national levels and poor sharing of information, among others. These challenges are now further compounded by the recent introduction of new policy reforms like fiscal decentralisation to the same local officials who do not fully appreciate the partnership and are therefore not likely to support it. The paper concludes with some useful suggestions on how these challenges may be tackled. Introduction A number of reforms have taken place in the health sector in Uganda in the recent past. One of the major reforms is Public Private Partnership for Health (PPPH). This article analyses the efforts made in the area of PPPH over the past decade with a focus on progress and challenges and proposals on how the latter could be addressed during the Health Sector Strategic Plan II (2005/06 to 2009/10). Partnership can be referred to as “the formal relationship between two or more partners who have agreed to work together in a harmonious and systematic fashion and being mutually supportive towards common goals, including agreeing to combine or share their resources or skills for the purpose of achieving these common goals” (MoH 2003). In health, the term Public Private Partnership has been used to refer to any on going relationship between the public and private sector and provides for a method of involving private health care providers in delivering public services. Such partnerships also provide a vehicle for coordinating with non-governmental actors to undertake integrated, comprehensive efforts to meet community needs (Harding and Preker 2003). The private sector in Uganda is recognised as a big and heterogeneous sector and includes: Private Not- For Profit providers [both facility and non-facility based] (PNFPs), sometimes referred to as NGO providers; the Private Health Providers [practicing western medicine and not NGOs] (PHPs); and traditional and complementary medicine providers (TCMPs) (Birungi et al 2001, MoH 2003). The private health sector is quite big with the PNFP constituting 42% of hospitals and 64 % of the capacity for training nurses/midwives in the country (MoH 2002). The size of the PHPs and the TCMPs is much more difficult to determine, but judging from household expenditure on health of US $10, which is about 55% of all health spending in the country, the bulk of which is spent with the PHPs and the TCMPs, this sub-sector is quite big and is providing a sizeable portion of the health services to the population (MoH 2004). It is therefore clear why PPPH would be considered an important aspect of Uganda’s health sector reform. Public Private Partnership for Health before and during the HSSP I The history of PPPH in Uganda The earliest recognised form of Public-Private Partnership for Health in Uganda is the relationship between Ministry of Health and the facility based PNFP sector dating back to the early 1960s under the general notice 245 of 1961, which is the tool government used to provide support to the voluntary sector as the PNFP were referred to then. This support however dwindled and eventually stopped during the crises of the 70s (Bataringaya and Lochoro 2002). The 1987 Health Policy Review Commission Report recommended integrating the private sector into the national health care system. This Report formed the basis for the 1993 government White Paper on Health Policy which highlighted the need for a higher profile for the private sub-sector in health. However it was not until 1996 that this issue actually got squarely on the health policy agenda. This has been attributed to a more sympathetic sector political leadership at the time, and the financial crisis that had hit some of the PNFP institutions and led to meetings between Ministry of Health leadership and the proprietors of these institutions (Birungi et al 2001). The process of institutionalizing PPPH was set in motion with the appointment of the NGO health sector panel which was assigned the role of formulating methods for collaboration between the government and the private sector. The recommendations of the panel were incorporated into the National Health Policy and the Health Sector Strategic Plan 2000/01 to 2004/ 05 (HSSP I). Subsequently the role of the panel was taken up by the PPPH Working Group which is one of the Technical Working Groups that operate under the Health Policy Advisory Committee (HPAC) for the implementation and monitoring of the HSSP. The PPPH Desk and Desk Officer for the coordination of PPPH activities were put in place in 2000. The areas for partnership were identified as: policy development, coordination and planning; resources management including financial resources mobilization and allocation, and human resources for health development and management; services delivery including management and provision of health services and community empowerment and involvement (MOH 2003). The progress against these is summarized below. Policy development, coordination and planning Collaboration and partnership between the public and private sectors in health is an important guiding principle of the National Health Policy and a key element in strengthening the health care delivery system as laid out in the Health Sector Strategic Plan (HSSP) (MoH 1999, 2000). A need was expressed to detail out a specific policy for PPPH and move away from working with ‘a gentleman’s agreement’ (Birungi et al 2001). The process to develop the PPPH policy started in 2000, with the PPPH Working Group responsible for drafting the policy. It has been a long process which has seen the development of a PPPH policy and components on PNFPs (facility-based and non-facility-based), PHPs and TCMPs. The components for the PHPs and TCMPs have taken longer to produce due to the less developed structures representing the players in these sub-sectors, and the need to really appreciate points of mutual interest and convergence. The draft policy currently awaits finalization of the TCMP component. Implementation guidelines are in place for the PNFPs (these deal most explicitly with issues of the PNFP facility based providers) and PHPs. The PPPH policy has been developed guided by the 1995 Constitution of the Republic of Uganda and the government’s liberalisation policy, which gives strong incentive for government to collaborate with and support private initiatives in health care delivery. The PPPH policy is also consistent with the National Poverty Eradication Action Plan (PEAP), recognising that for development to be sustainable, health and economic growth must be mutually reinforcing (MoF 2004). As such all government and private sector partners in health should be working towards the goal of poverty eradication and economic growth. The policy takes into account the roles and responsibilities of local government structures for service delivery under decentralisation. With the movement towards SWAp in the late 90s at the national level efforts were made to include some representatives of the private health sector in some of the SWAp structures like the Health Policy Advisory Committee (HPAC), the HPAC Technical Working Groups (which include PPPH) and the Health Sector Working Group (Bataringaya and Lochoro 2002). These groups are responsible for working with government at national level for purposes of policy development, implementation, monitoring and resource mobilization and allocation. The PPPH Desk provides a focal point for partnership issues. At the service delivery levels there had been adhoc coordination and planning with PNFPs in the past in some districts, depending on the circumstances and personalities. With the evolution of the current partnership, more is being done: a number of districts have put in place District PPPH focal persons in line with the implementation guidelines and PNFP health institutions especially the facility-based are now more routinely being involved in comprehensive planning and monitoring for district and health sub-district (HSD) health services. As an example 29 HSDs (13.5%) are headed by PNFP facilities. The Health Management Information System (HMIS) routinely captures information on facility-based PNFPs (Bataringaya and Lochoro 2002). Resources Management Even as the process of developing the PPPH policy and implementation guidelines has been going on, partnership in terms of resources management – finances, supplies and human resources has been taking place. Financial resource mobilization and allocation In 1997/98 government resumed provision of the subsidy to the facility-based PNFPs in form of the Delegated Funds under the Primary Health Care Conditional Grant (PHC CG). This is a recurrent nonwage grant channeled through the local government, initially extended to hospitals in crisis and subsequently widened to include all PNFP hospitals and Lower Level Units (LLUs). In 2001/02 the grant was also extended to PNFP Training Schools, and in 2003/04 a medicines credit line was introduced for both government and public hospitals and LLUs. A wage subvention has been in place for PNFP facilities to cater for mainly seconded medical officers but was for the first time explicitly indicated in the budget in 2002/03. The entire package to PNFP health facilities has grown from 1 billion in 1997/98 to just under 21 billion Ug. Shs. in 2005/06 as shown in Table 1 (MoH 1997, 1998, 1999b, 2000b, 2001, 2002b, 2003b, 2004c, 2005b). Smaller sums of money from the budget have been given to a few non-facility based PNFPs including MildMay, TASO, Uganda Red Cross, UNHCO and the Religious Bureaus through the government budget – in total just below 1 billion in 2000/01, but subsequently less (MoH 2002b). These figures represent the funds that are readily traced in the Government budget and some interventions which include government budget and donor funds (N.B.: the medicines credit lines include DANIDA support to the Essential Medicines Account). However public funds are channeled to the private sector much more frequently than this, particularly if the definition of public funds includes donor funds declared in bilateral and multilateral agreements. This is clearly illustrated by the National Health Accounts Report for 1998/99 to 2000/01 which showed that 60% of all donor project funds are channeled through PNFPs especially the non-facility based PNFPs (MoH 2004). Much more recently this is noted to be the case with Global Fund for AIDS TB and malaria (GFATM) and the US Presidents’ Emergency Fund for AIDS Relief (PEPFAR). These Initiatives have identified the private sector, especially PNFPs, PHPs, and other private enterprises dealing in health-related business, as major partners. In addition supplies in kind are usually provided including: vaccines, contraceptives, specific drugs like for TB and HIV/AIDS. PHPs and TCMPs do benefit from public funding in a number of circumstance but to a much less extent. In the FY 2004/05 for the first time a few PHP hospitals benefited from the government budget (MoH 2004b). Table 1: Facility-Based PNFP facilities’ GOU Budget Allocation (Billion Shs.)
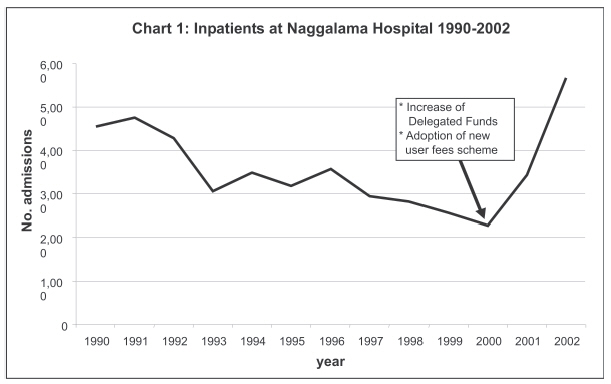
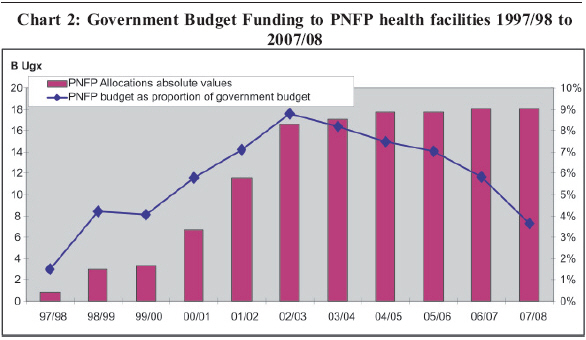
Human Resource Development and Management Another substantial area of partnership has been in human resources development and management. The large private sub-sector requires many health workers – for example the facility-based PNFPs employ about 10,000 health workers (MoH 2003)). The number of health workers with the PHPs and TCMPs are much more difficult to estimate, because of the heterogeneity and poor representative structures among these partners but also because there is a high rate of dual employment particularly between government and the PHPs. The private sector train many health workers, with the facility-based PNFPs training up to 70% of the country’s nurses and midwives (MoH 2003). Progress in partnership in this area has been slow and cautious. The government makes a contribution to training schools in PNFP institutions (see Table 1) as do some donors namely the European Union (EU), Italian Cooperation (IC), Department of Cooperation Ireland (DCI), and DANIDA. The PNFP training schools, or more commonly the Bureaus on behalf of the training schools, are getting more involved in the discussions on training policy and standards. The wage subvention to cater for 118 medical officers has been in place and has not changed much over the years. Capacity building at the management and service delivery levels carried out by government more often than not include health workers from facility-based PNFPs but less for the non-facility based PNFPs. Capacity building of TCMPs usually takes place for Traditional Birth Attendants (TBAs) and for traditional healers involved in certain disease programmes like HIV/AIDS. Service Delivery What has been the effect if any of these efforts in policy development , planning, resource mobilization and allocation on service delivery? There is an opinion among health sector reform proponents that the private sector is more efficient than the public sector (Preker 2005). But often times this is not backed by hard facts in the local setting. Given the efforts in partnership that have been made in Uganda in the recent past, it was thought necessary to analyze the effect of this partnership. Specific analysis was made by the Uganda Catholic Medical Bureau (UCMB) in the 27 hospitals that are affiliated to them. Data from these hospitals for the period since 1995/96 was used to determine whether partnership objectives of: increasing access; improving quality; and increasing provision of preventive and promotive health services had been achieved. From this analysis Giusti et al 2002 shows that there had indeed been a crisis in the facility-based PNFP sub-sector in the mid-90s, with falling utilization of these facilities at its worst in 1997/98 and recovering to 1995/96 levels by 2000/01. This was in line with the decline in user fees in these institutions that was made possible by the injection of funds from government referred to before. Data from the HMIS at the district and health facility level and a number of studies done linking the HMIS with the communities have also shown that increasing utilization of PNFP health facilities has been related to decrease in user fees following increase in government and/or donor funding (Santini S 2002,; WHO 2005). Chart 1 below shows the experience of Naggalama hospital in central Uganda. A positive effect has also been noted in the quality (as measured by qualified staff availability) and the level of involvement in preventive and promotive heath services by the PNFPs (Giusti et al 2002). It is much more difficult to analyze the effect of the partnership on the non-facility based PNFPs, PHPs and TCMPs. Of recent there has actually been concern about the lack of impact of the investment in TBAs on maternal mortality statistics. Challenges to the PPPH in Uganda The progress in PPPH in Uganda over the last decade has been significant. However a number of challenges still exist which need to be addressed. These include challenges in policy development and conceptualization of the partnership; resource mobilization and allocation and information sharing. Policy development and conceptualization of the partnership The process of drafting the policy for PPPH started in 2000, five years later the national policy on PPPH is still in draft. This apparent delay has occurred because efforts have been made to generate consensus among most stakeholders especially the different components of the private sector and the various levels of government. The most challenging aspect has been the policy dialogue with the PHPs and the TCMPs. This has been difficult because of the need to identify common goals and the heterogeneous nature of the providers who constitute these components. There is no approved policy or regulatory framework for the TCMPs, and efforts are being made to put these statutory instruments in place. This is required before the PPPH policy can be submitted for approval by the executive arm of government (Cabinet) and then passed on to the legislature (Parliament). It is unlikely therefore that an approved PPPH policy will be in place in less than a year’s time. The failure to have an approved policy on PPPH has far reaching implications -decisions are being made based only on draft policy documents and mutual understanding. Given the diversity of players and changing ways of work this could lead to challenges of policy and/or legal implication. This is likely to be a continuing challenge at the local government/service delivery level, where the private sector is usually viewed as a competitor. In the era of Fiscal Decentralisation Strategy (FDS) where local governments are being allowed increasing flexibility in the allocation of public funds this is likely to be a source of friction. Despite the fairly advanced stage of the partnership, there are still challenges of conceptualization within the partnership with the tendency to relate partnership with funding. This often leads to the understanding of the partnership in Uganda to just the relationship between government and PNFPs and specifically the facility-based PNFPs which are benefiting most from government funding. PPPH is also seen by some as the threat to the autonomy of the private sector, and some of the private sector stakeholders especially proprietors of PNFP facilities have even indicated fear that PPPH might be a sneaky way for government to take over these privately owned institutions like happened with missionary-founded schools in the Uganda in the 1960s. Quite often the bigger role of government as a steward is not given its due emphasis both by government and private sector managers in the PPPH. Regulation of the private sector has been recognised as a function of government. However the relationship between regulation and other aspects of partnership is not well appreciated and recent activities of the partnership have not put as much emphasis on the regulatory aspects. Resource mobilization and allocation Progress has been noted in resources mobilization and allocation in the partnership. The period 1997/98 to 2002/03 showed marked increase in the funding from government to the facility-based PNFPs as shown in Chart 2 (Nyamugasira 2005). However in recent years the amount of funds allocated to the PNFPs has stagnated just below 20 billion Uganda shillings (N.B.: this analysis utilises the government budget figures only and does not include the medicines credit line). This has been related to the overall slow growth of the government health sector budget that has been attributed to the conservative management of the macro-economy (MoF 2004). However as is represented by the right axis on Chart 2, as a proportion of the health sector budget, funding to the PNFP has declined for the last 2 budget years and is set to decline further given figures indicated in the Medium and Long Term Expenditure Framework (MTEF and LTEF). The PNFP health facility budget was 9% of the health sector budget in 2002/03 compared to 7% in 2005/06 and a projected 4% in 2007/08. This shows that even within a stagnating resource envelope the funding to the PNFP facilities has slipped from its former level of prioritisation. This is of concern to the PPPH stakeholders in Uganda and particularly the PNFP health facilities that have made decisions on the basis of the broad health sector policy which includes increasing access to basic health services by all Ugandans including the poor, women, children and other vulnerable groups. This had led to adjustment of user fees in these institutions (decreased levels and flatter fee structures), which move requires a consistent and increasing source of funds. However as has been mentioned before this is not the only source of public funding for the private sector. Substantial financial support is received from donor projects and Global Initiatives like the GFATM, PEPFAR and the World Bank Multi-country AIDS Project (MAP). The biggest challenge with this type of support is accountability – linking the inputs with the outputs. This is usually because the donor organization often deals with the particular PNFP or PHP on a vertical arrangement, without the necessary linkages with other stakeholders. This often leads to inequitable and inefficient use of the resources. In addition these resources are usually provided for a specific purpose and time-frame, with minimal opportunities for systems building (including stakeholder accountability structures) and sustainability. The recent media detailing of non-registered NGOs allegedly benefiting from GFATM resources is a case in point (Weekly Observer Sept. 15, 2005). The private sector is the major recipient of funds from households estimated at about US $ 10 per capita. The government as steward has a responsibility to the population to put mechanisms in place to understand who is paying this money, who receives this money and whether these resources are being efficiently and equitably used. This is particularly of concern given that more than 70% of these funds are out-of-pocket – i.e. patients pay directly to the providers and not through any developed insurance mechanisms (MoH 2004). The challenges in human resources development and management are two-fold – some relate to the budgetary constraints referred to above and others to the institutional framework for Human Resource Development in the country. Government has implemented pay rises for public health workers of up to 100% over the last 5 years. These pay rises and recruitment of health workers into government service has triggered off instability within the PNFP sub-sector including low morale, in some cases even strikes by the PNFP health workers and, massive exodus (MoH 2005b). The funding to the PNFP health facilities from government has not been increasing at the rate to take care of this marked increase in salaries. The PNFP workers constitute about one third of the 30,000 work force within the health sector, this is a substantial proportion of the workforce and are responsible for a big part of the health sector output. There is evidence that up 20% of the PNFP health workers leave every year and although replacement takes place there remains a net loss and the replacements take time before they can perform well only to be lost again just as they begin to be competent enough. (MoH 2005b). The wage subvention to PNFP originally targeted to finance salaries for 118 medical officers, considered back then to be the most critical cadre needed, has not changed in amount or mechanism to adjust to current circumstances. The current subvention is not flexible – the funds can only be paid out to medical officers recruited and posted by the Health Service Commission, and once these officers leave the process to replace them takes several years. A recent survey found less than 50% of these medical officers in post – the rest were either on study leave or not accounted for (MoH 2005b) Health workers training policy and regulation in Uganda, is largely handled by Ministries of Education, Public Service, Health Service Commission and the Ministry of Health (Nurses and Midwives Council, and Personnel and Human Resource Development Divisions). The PNFP training institutions contribute the bulk of output of the nurses and midwives in Uganda. However in the past they have not been involved as much as they should in policy and regulatory framework development. Two major changes over the last decade have had huge implications for the PNFP training schools namely – the transfer of the responsibility for basic health workers’ training from Ministry of Health to Ministry of Education, and the change from singly trained nurse and midwife to the comprehensive nurse. These decisions have had wide reaching policy and financial implications for the PNFP institutions yet they were not seriously involved in the decisions and were not adequately prepared for the changes. As a result of such uni-lateral decision making, Enrolled Comprehensive Nurses training which was initiated 4 years ago had by the end of the FY 2003/04 produced only 2% of the expected output from all from all Training Schools and less than 30% of the PNFP Schools had commenced ECN courses (MoH 2004c; 2005b). Information sharing, Monitoring and Accountability The SWAp and PPPH in Uganda have led to a marked improvement in sharing information amongst partners particularly using the SWAp and PPPH structures especially the Joint Review Missions (JRM), HPAC, PPPH and other Working Groups, the Health Sector Working Group; the Annual Health Sector Performance Report (AHSPR) and the Budget Framework Paper (BFP). At the national level this has worked very well especially for the partnership with facility-based PNFPs which are well represented in these fora and documents. However between the public and the non-facility based PNFPs, the PHPs and TCMPs there are still big challenges of information sharing, monitoring and accountability. The HMIS and sector reports do not routinely include information on these sector stakeholders. Accountability of these stakeholders is usually limited to donor projects that support them, and the voluntary associations some of them belong to. This is still a big gap in the partnership. Expectations of the HSSP II The HSSP II just as the HSSP I derives its mandate from the Millennium Development goals, the PEAP and the National Health Policy. Development of the HSSP II was also guided by the need to consolidate the achievements of the HSSP I (MoH 2005c). In the HSSP II, the PPPH efforts highlighted include the following:
Emphasis is put on strengthening and broadening the partnership through more active engagement with other health related sectors, professional associations, private health care providers and TCMP, civil society and representatives of the principal consumers. In addition it is planned that a similar policy framework will be developed for other private service providers such as private laboratories, pharmacies, drug shops and civil society non-facility-based service providers. The objective is to update and harmonize regulatory provisions governing the various components of the private health sector. The important role of traditional and complementary medicine is recognised, and the need to expedite the process of facilitating the TCMP groups to come together and develop an appropriate policy and draft regulatory bill. These are the broad statements included in the HSSP II. The question then is – does this provide enough leverage for the PPPH stakeholders to address the challenges highlighted in the previous section? There is a lot that the PPPH stakeholders can do given this framework. Some specific suggestions are made here: Policy development and institutionalization of PPPH The PPPH policy needs to be finalised and ratified by the appropriate institutions of government. This is urgently required as implementation of the HSSP II begins – there are many new players and changing circumstances. The “gentleman’s agreement” used early in the HSSP I will not have much influence during the HSSP II. However the need for a TCMP Policy and Regulatory Bill before submission of the PPPH policy implies that this process will require at least another year. The remaining part of 2005 and most of 2006 are a very busy period for the executive and legislators, and such “non- priority” issues may not quickly get on the Cabinet and Parliament agenda. The structure and mandate of the PPPH Office though may have implications on the process including the pace of policy development. The current PPPH Office was put in place to coordinate PPPH, with the support of the Italian Cooperation. This was supposed to be a medium term arrangement with the Office eventually to be fully taken up into the MoH structures and supported by public resources (budget and otherwise). The transition has not yet taken place and the Office is currently not well facilitated to carry out its functions. This has to change if the processes initiated are to be taken to their due conclusion. Resource mobilization and allocation Resource mobilization and allocation is a major challenge for the HSSP II – and not just in terms of PPPH but more generally. The expectations of the international, national and sectoral stakeholders are much more than the resource envelope as it is currently known. This is very clearly demonstrated by the funding gap which ranges between 44 -53% of the HSSP II cost over the 5 years (MoH 2005c). This has led to further prioritization within the HSSP II shown in the short to medium term scenario that is to be reviewed every year, during the budget cycle. How much these funding resources are shared amongst sector stakeholders will ideally depend on the level of the priority the activity the stakeholder is involved in. However as demonstrated by Chart 2, the level of prioritization given to funding the private sector in the most recent past, here equated to the PNFP health facilities, has been on a downward trend. This understanding is reinforced by the finding that in the process of developing the HSSP II there was unwillingness to accept or understand the implications of the health partnerships (Euro Health Group 2005). Although the costing of the HSSP II took into account the private sector particularly the facility-based PNFPs, the financing does not explicitly deal with this issue. The resource allocation aspect of the partnership, especially regarding the PNFPs and the government budget needs to be tackled explicitly over the period of the HSSP II – more so than is currently spelled out in the document. On the other hand some donor projects and initiatives will continue to support the private sector. There is need to put mechanisms in place for increasing accountability for the use of these resources to ensure efficiency and equity. The challenges of human resource development and management although recognised in the HSSP II are only half heartedly addressed. There is need to address motivation of the health workers in the facility-based PNFPs, together with the public health workers, to ensure overall efficiency and equity. The role of salaries in this, the source of funding for these salaries, together with the institutional arrangements for implementation of any updated human resource partnership schemes need to be properly articulated. The findings and recommendations of several studies including the Task Force on PNFP health workers should be part of the short, medium and long term sector expenditure framework (MoH 2004b; MoH 2005b). Under an updated framework the wage subvention currently meant for the 118 seconded medical officers should be reviewed and made more appropriate – reacting to actual need (what cadres are needed most, where), and ensuring maximum utilization. Information sharing and M&E The framework provided by the HSSP II can be used by the stakeholders to build a health sector database which reflects that actual service proportions by the public and the private sub-sectors of health. This would be useful in developing future policies for the heath sector. There is need to provide appropriate incentives for the non-facility based PNFPs, PHPs and TCMPs to provide information on inputs, processes and outputs so as to judge levels of efficiency and equity in the private sector. This will determine the interventions required of government as a steward. Conclusion Marked progress has been made during the HSSP I towards the National Health Policy objective of making the private sector a major partner in national health development. A number of achievements have been made in the areas of policy development, planning and coordination; resource mobilisation and allocation; and service delivery. However a number of challenges have been noted in the various aspects of the partnership. In the HSSP II a number of objectives and strategies have been highlighted for the purpose of taking the partnership forward. It is important though to appreciate the environment in which the HSSP II is to be implemented. Is there the will to make PPPH in Uganda over the HSSP II work? Or has it gone out of fashion? Given the efforts that continue to be made by institutions and individuals from the public and the private sub-sectors of health, there is reason to believe that the will to make the partnership work is still there. However the climate today is much more challenging for reformers than it was 5 years ago at the launching of the HSSP I. although initial steps to establish the partnership have been taken, it is important to consolidate this, and broaden and take forward the partnership both in the type of stakeholders, and the depth of the partnership. The next steps are crucial and will determine whether the partnership succeeds or stays struggling at its current levels. There has to be appreciation of this by the various stakeholder institutions (government, donors, private sector), and individuals (politicians, technocrats, proprietors, front-line health workers) in the partnership to move away from business as usual and look for innovative and practical ways to make the partnership work for them. In the end Uganda requires both the public and private sectors to be working together to reap efficiency and equity gains that will enable the attainment of the PEAP and MDG targets. References.
Copyright 2007 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp07006c2.jpg] [hp07006c1.jpg] |
| |||||||||

{kind=link}
{kind=link}