 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
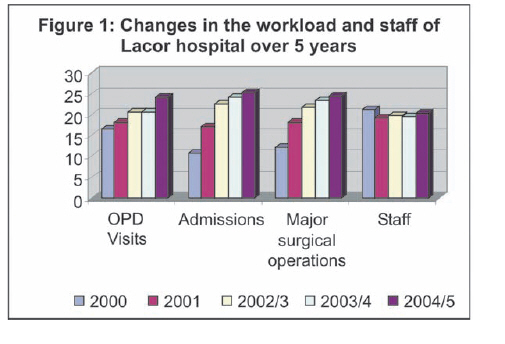
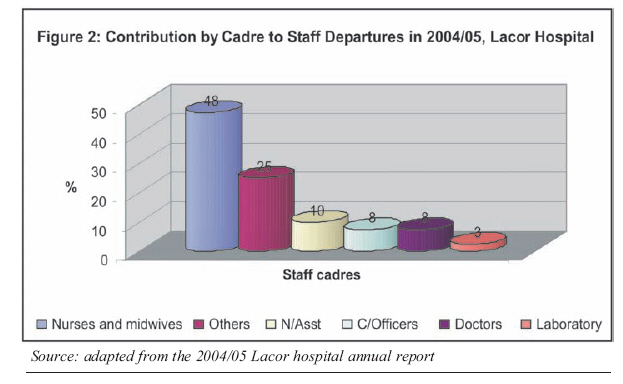
Health Policy and Development Journal, Vol. 6, No. 1, April, 2008, pp. 1-15 THEME ONE: HUMAN RESOURCES FOR HEALTH Using The Workload Indicator Of Staffing Needs (WISN) Methodology To Assess Work Pressure Among The Nursing Staff Of Lacor Hospital John F. Mugisha1 and Grace Namaganda1 1 Faculty of Health Sciences, Uganda Martyrs University Code Number: hp08003 Abstract In their effort to provide adequate and quality health services, health systems in both developed and the developing countries have to confront the challenges of an ever increasing population with limited or diminishing resources. This includes the human resource which constitutes a major input in health care delivery and a key determinant of the cost and quality of care. There is an increasing need therefore for health organizations to identify the most appropriate staffing levels and skill mix to ensure efficient use of the limited health personnel. This paper demonstrates the use of the workload indicator of staffing needs (WISN) methodology in determining staffing requirements for the nursing staff in a hospital setting. It shows how the results can be used to assess overstaffing and understaffing as well as determine the work pressure among the different categories of nurses thus providing a basis for effective nurse redistribution to exploit efficiency gains without compromising the quality of services. Introduction: Health systems in both developed and developing countries are under pressure to improve service delivery to an ever increasing population with limited or reducing resources (Hossain and Alam, undated). This includes the human resources which constitute a major input in health care delivery and a key determinant of the cost and quality of care. Expenditures on personnel in most health systems around the world account for over 70% of recurrent budgets (Buchan, 1999; Ozcan and Hornby, 1999; Hall, 2001; and AED, 2003). There is an increasing need, therefore, for health organizations to identify the most appropriate staffing levels and skill mix to ensure efficient and effective use of the limited resources (Buchan, 1999). If used efficiently health personnel can make a major contribution to the health of a nation. Often times however, health personnel are in wrong proportions to each other, in the wrong geographical locations, sometimes spend too much time on activities that make a limited contribution to health care or are inappropriately used considering their level of training (Hall, 2001; Namaganda, 2004; Delanyo, 2005). In Africa, like in several other parts of the world, the number of trained health personnel has historically been inadequate hence the need to use this scarce resource effectively (AED, 2003). This has created the need to scrutinize closely the basis on which staff is distributed throughout the health service and how they can be used more effectively and efficiently for the good health of the population as a whole (Ozcan and Hornby, 1999). This translates directly to determining appropriate numbers and skills mix for the individual health facilities. The total number of staff and their skill mix required to work in a health facility will depend on the workload and the scope of services of the health facility (Shipp, 1998). Therefore health facility staffing norms based on population or health unit size alone without consideration to the workload may not be appropriate (Shipp, 1998; Ozcan and Hornby, 1999). Hence, introduction of the workload indicator of staffing needs (WISN) methodology to determine staffing requirements basing on the fact that each health facility has its own pattern of workload and each type of workload calls for effort i.e. time from specific health staff categories. This therefore means that each health facility will have its own staffing requirements depending on its workload. The WISN methodology was developed by the WHO and has been used to determine staffing requirements in countries such as Papua New Guinea, the United Republic of Tanzania, Kenya, Sri Lanka, Bahrain, Egypt, Hong Kong, Oman, Sudan and Turkey (Shipp, 1998). Although determining staffing requirements per facility may seem cumbersome it has the advantage of ensuring effective and efficient use of staff by eliminating problems of over or under utilization of staff and staff inequalities where staff of the same category and in the same location work under differing work pressures (Buchan et al, 2002). This paper presents the experience of using the WISN methodology in determining staffing requirements for nurses in Lacor hospital, in northern Uganda. The workload was compared to staff numbers to assess work pressure facing nurses in different departments and suggestions made for staff redistribution to even-out this work pressure. Lacor Hospital Lacor hospital is a private-not-for-profit (PNFP) hospital located in Gulu district in Northern Uganda. The hospital is owned by the Gulu Archdiocese and is accredited to the Uganda Catholic Medical Bureau (UCMB). Its activities are in line with the Ugandan Ministry of Health (MoH) policies for health care delivery. Founded in 1959 by the Comboni missionaries and Gulu Archdiocese as a dispensary, Lacor hospital sought to pursue a mission of providing health care to the needy and fighting disease and poverty. Today Lacor is a fully-fledged hospital with a total of 468 beds and an average of 500 outpatients per day. It also runs peripheral health units at Amuru, Opit, and Pabo as satellites to the main hospital and has over 500 staff. In addition Lacor has training schools for Nurses, Anaesthetic assistants and Laboratory assistants and is now a teaching hospital for Gulu University medical students. It also trains intern doctors from the Universities of Makerere and Mbarara. Yet, it operates in a very difficult political and socio-economic environment due to the long rebellion by the Lord's resistance army (LRA) which has been fought in the area since 1986. It is hardly surprising, therefore, that a huge number of the hospital's catchment population comprises the internally displaced people and refugees from the neighbouring and equally unstable southern Sudan. Problem analysis High staff turnover especially of low cadre nursing staff is a major human resource problem in Lacor hospital. According to the hospital management, the nurses cited work pressure as one of the reasons for leaving the hospital. Analysis of hospital data indicates an increase in workload without a corresponding increase in staff numbers over a five year period. This could mean that the staff was now working under more pressure than was previously the case and was suspected to be a contributing factor to the further staff attrition. Figure 1 below illustrates this. Further analysis of data indicates that the Nursing cadre has been worst hit by the problem of staff attrition as demonstrated in Figure 2. High turn-over of staff makes human resource planning difficult for the hospital managers. Most importantly it contributes to stress among the remaining staff, compromises the quality of care and threatens continuity of services. The high staff turnover may also create a feeling of insecurity and a `band-wagon effect' leading to a vicious cycle of staff turnover. It should be noted that a high staff turnover rate may not be replenished through recruitment given both the high costs involved and the fact that Lacor hospital is located in a war ravaged area and therefore not able to compete favourably for the scarce nurses on the open market. In an attempt to solve the problem of staff turn-over, the management of Lacor hospital requested Uganda Martyrs University to examine the work pressure among the nursing staff and advise on how they could be distributed within the different hospital departments to reduce the pressure without compromising quality and efficiency in service delivery. General objective The general objective of the study was to assess the workload pressure among the nursing staff of Lacor hospital and to determine the optimum nursing requirements needed to adequately handle the present workload. If used, the results of this study would possibly contribute to the improvement of human resource planning and management and overall efficiency in the hospital. Specific objectives The specific objectives of the study were:
Methodology and design This was a descriptive cross sectional study that adapted the WISN methodology. Like all WISN studies, the methods used were mainly quantitative. The data for the study were collected in January 2006 and therefore the workload statistics used were those of January 2005 to December 2005. This was done to enable us determine staffing requirements that were as close to the present workload situation as possible. Scope of the study Due to limited time, it was not possible to study all departments in the hospital. Therefore this study covered eighteen departments which were selected purposefully in consultation with the hospital management. The departments selected included: the general outpatient department (OPD), the dental clinic, Aids clinic, Antenatal clinic (ANC), Casualty, Private clinic, Young child clinic (YCC), Maternity ward, Three wards under surgical department , Two wards under medical department, Three wards under paediatric department, Theatre and Anaesthetic department. These departments were chosen because they utilise nurses to deal directly with patients and are therefore directly affected by high workloads. Secondly, this is where most complaints about high work pressure had originated. Using the WISN To assess the work pressure and to calculate the nursing requirements for Lacor hospital using the WISN, we followed a sequence of steps that included the following:
Identifying the activities carried out by the different cadres of staff in the hospital. Each category of staff has got specific activities that they carry out in a hospital. To get a comprehensive list of all activities carried out by each type of staff cadre, we sent a questionnaire to the heads of departments a month prior to data collection asking them to list the activities carried out by the different nurse cadres under them. The lists of activities from the different departments were then used to compile comprehensive lists of activities carried out by the various nurse cadres. This list was further updated during the data collection period through observations and also during the group discussions with senior and experienced professionals of each staff category. Setting activity and allowance standards for the activities identified. After compiling the comprehensive list of activities for each department, we assigned one researcher to each of the departments selected for the study. The aim of doing this was three-fold: to observe what activities were being carried out in the department and update the departmental activity list, to time how long it took to carry out each activity and to note which nurse cadre carried out each particular activity. At least three observations were done per activity on the list and averages calculated which were used to guide professional group discussions. In total we carried out six professional group discussions with senior, knowledgeable and experienced nurses and nursing assistants during which we also set activity and allowance standards for all activities. For activities that are rare and could not be directly observed, we depended on the experienced professionals to set the activity or allowance standard. An activity/allowance standard is the time it would take a well trained and well motivated member of a particular staff category to perform an activity to acceptable professional standards (Shipp, 1998; Buchan, 1999). For activities which are carried out per patient and whose annual workload can be obtained from the service statistics, we set activity standards. We set allowance standards for those activities which are done for more than one patient at a time and whose annual workload cannot be obtained from the service statistics e.g. health education talks. Allowance standards set were of two types: individual and category allowance standards. Individual allowance standards are set for activities done by one or a specific number of staff. For example a nurse may take 30 minutes per week to write minutes of meetings. This is an individual allowance standard. Category allowance standards are for activities done by all staff of the same category. For example, all nurses, irrespective of level, spend one hour per week to do general cleaning on their wards. This is their category allowance standard. Whereas we appreciate the possibility of aggregating the individual activities into few sub-groups composed of related activities e.g. direct patient care, administration and management etc as has been done in other WISN studies, we realised that such a venture would be confusing to most staff and possibly jeopardise the use of the results. Therefore we decided to set activity standards per individual activity. Efficiency and quality considerations While setting activity standards, we were wary of the need to use staff more efficiently without compromising quality. We used group discussions to utilise the professional judgment and experience of some senior staff to set activity/allowance standards with the underlying goal of ensuring appropriate and effective use of staff and performance within acceptable quality. For each activity a consensus was reached on who should be the most appropriate staff cadre to carry out the said activity and how long it would take to accomplish the activity without compromising quality or being inefficient in staff use. Below are some of the measures that we took:
Calculating the available working time (AWT) for each staff category Available working time is the amount of time available in a year, per staff category for delivering health services (Shipp, 1998). That is, the actual time spent per staff category at work. The AWT depends on how many days are spent in holidays, official leave, off duties and other absences. Data on staff absences was collected both through interviews with the senior nursing officer and medical director and by review of personnel records. The available working time for each nurse category was then obtained by subtracting the total absences per nurse category from the total working days in a year. The total days off due to the different absences were divided by the total staff per category to obtain the average days off per staff. For example the total days spent on maternity leave in a year were divided by the total number of staff to get the days spent on maternity leave per staff. Calculating nurse requirements in the selected departmentsStaffing Requirement per department was calculated using the formula given by Shipp (1998) i.e. Staff requirement = Basic staff requirements *Category allowance factor + Total Individual Allowance Standards. The basic staff requirement is the staff you need to cover the workload reflected in the annual statistics. Therefore, basic staff requirements = Annual workload divided by standard workload. Annual workload was obtained per department from the inpatient and outpatient Health Management Information System (HMIS) annual summary reports. The workload used was that from January 2005 to December 2005. The reasoning behind this was to use the most recent data so as to reflect the staffing situation which is as close to the present situation as possible. Standard workload is the amount or volume of work in delivering health services which can be accomplished during the course of the year by one staff working to acceptable professional standards. Standard workload = Available working time in a year (AWT) divided by Activity standard With the AWT known and the activity standards set, it was easy to calculate the standard workload and subsequently the basic staff requirements. After obtaining the basic staff requirements we multiplied the result by the category allowance factor. Category allowance factor =1/1-(Total % Category Allowance Standards) (Shipp, 1998). Allowance standards are set in different units i.e. either per day, per week, per month or per year. They are thus standardized by changing them to percentages of the available time in the different units e.g. an activity which occupies a staff for one hour a day will be standardized by dividing one hour by the eight working hours in a day and changed into a percentage. When totalled up one is able to calculate the category allowance multiplier. The product of the basic staff requirements and the allowance multiplier is referred to as intermediate staff requirements. To this you have to add the total Individual allowance standards to get the total staff requirements. Individual allowance standards are added, not multiplied because these are activities done by either one or a very few members of the department and therefore which do not constitute a multiplier effect. Provision for night duty The wards that have night duty got a special consideration. When nurses in Lacor hospital work the night shift, they are compensated with three days off as payment for one week of night duty. This time of rest is therefore counted as ordinary working time and needs a staffing provision. This means therefore that for the wards and other departments with night duty, the nurse staffing requirements have two components:
The night duty in the hospital was 10 .5 hours per night and each staff did night duty for 7 consecutive nights. For each night duty (i.e. 7 nights) the nursing staff was given 3 days off. Such off duty needs a nurse provision because during these off duties the nurses are not available for work. Night duty therefore requires (10.5 hours per day x3 days off per week of night duty x 52 weeks in a year) hours of staff time a year. This means that the time to be compensated is also (10.5x 3 x 52). But the nurses were available for 1884 hours a year while the nursing assistants were available for 1815 hours a year. So the staff equivalent of the time off as compensation for night duty would be equal to (10.5x 3 x 52)/ 1884 for nurses and (10.5x 3 x 52)/1815 for nursing assistants. The staff requirements thus obtained is the staff that would be needed to cover both the workload reflected in the annual statistics and workload that is not reflected in the annual statistics and is true only for departments that do work at night. Calculating the WISN for the different nurses per department The WISN is the ratio of present staffing numbers to the calculated staff requirements. This ratio is unique to this methodology and is the basis of its name (Shipp, 1998). The WISN ratio is used to demonstrate the varying work pressure among the departments and among staff of the same cadre. The WISN ratio was determined by dividing the present staffing in the hospital with the calculated staffing requirements per department. The present nurse numbers were obtained from the hospital staff list for the month of January 2006. Ideally we should have used the nurse numbers for 2005 but we wanted to assess the pressure as of 1996 assuming the workload was to remain the same as of 2005. Measures to ensure validity and reliability Reliability means that under constant conditions, measurement will yield similar results when repeated while validity means a scale's ability to measure what it is supposed to measure (Moser and Kalton, 1993). Validity and reliability can only be achieved if data are accurate and the data collection process well monitored. The following measures were taken to ensure quality of the process:
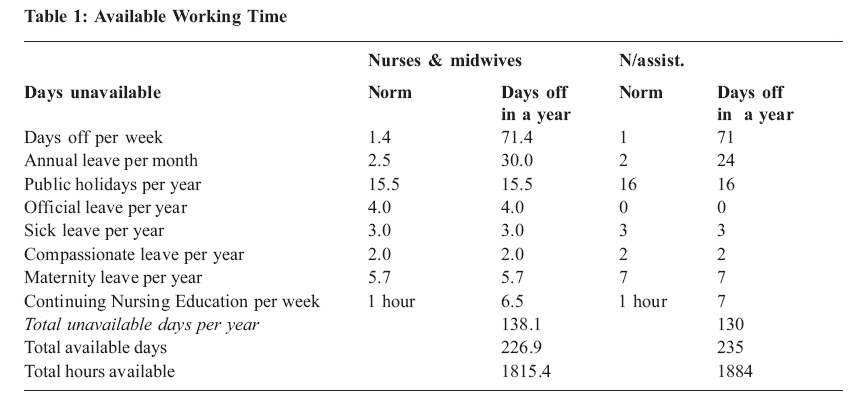
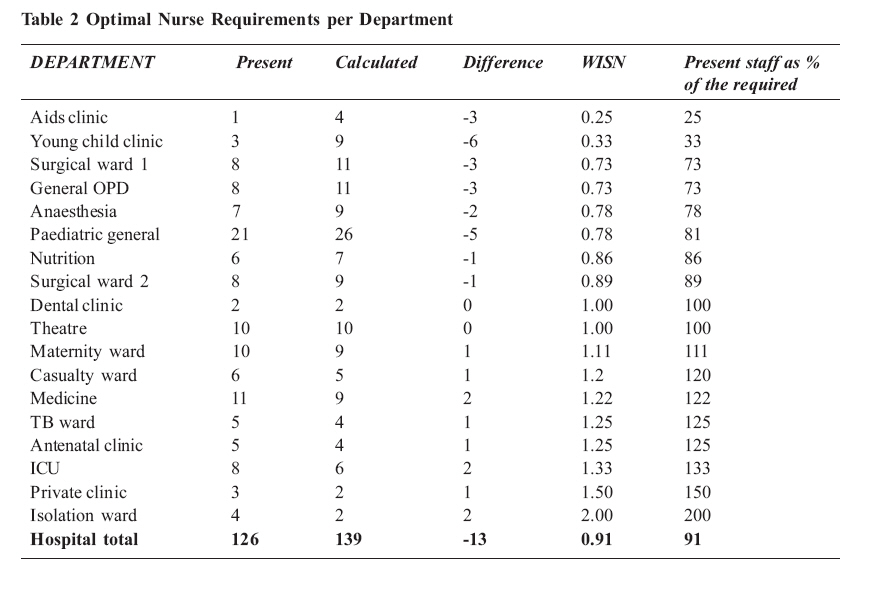
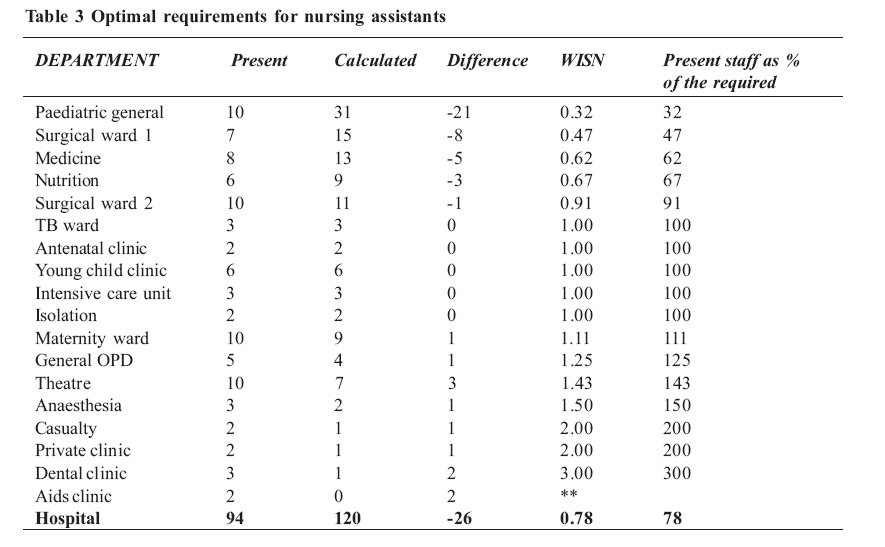
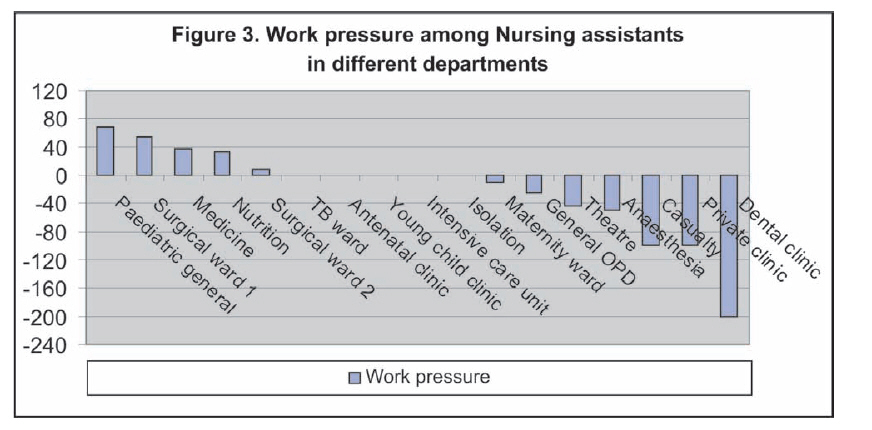
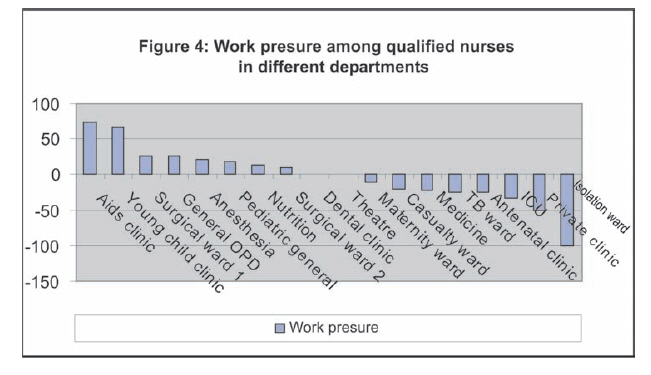
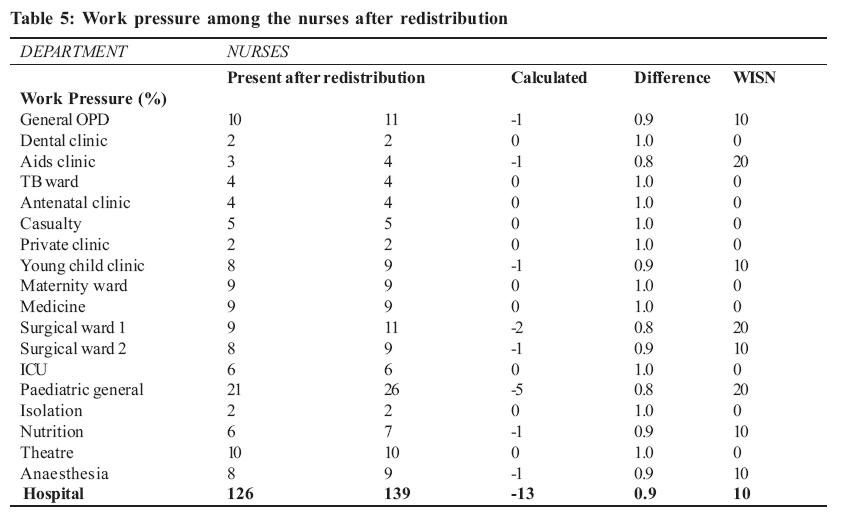
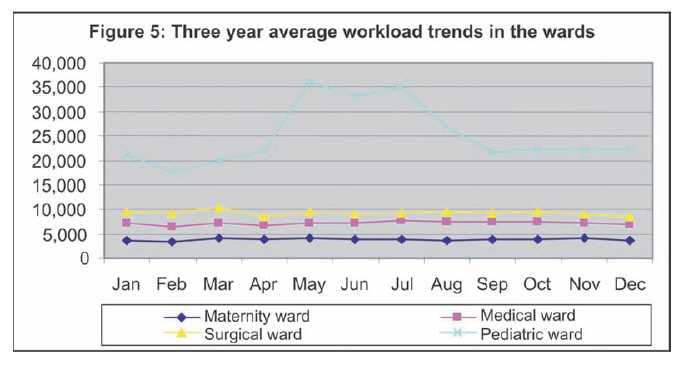
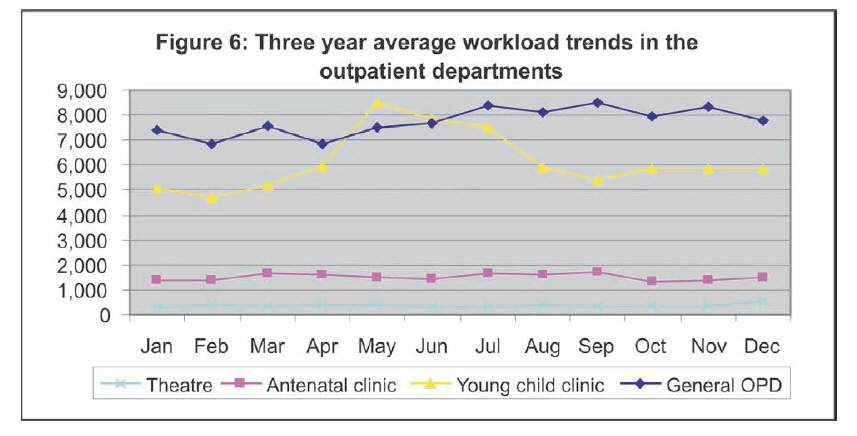
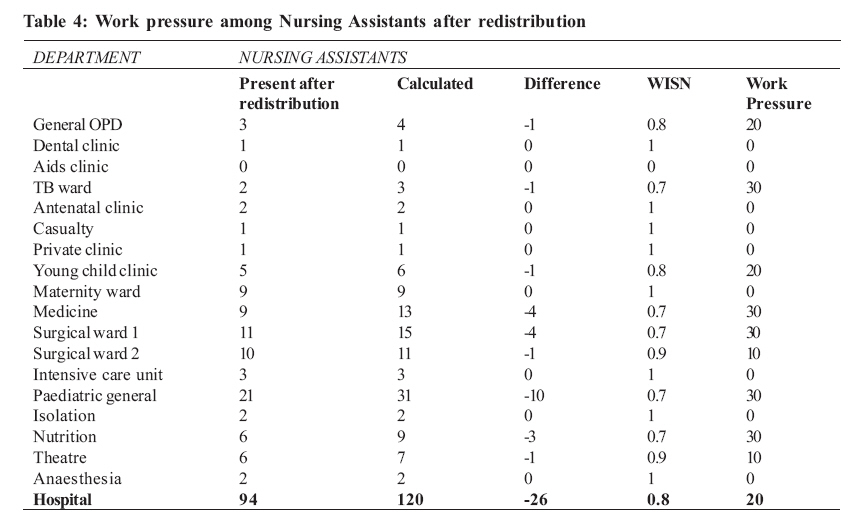
Ethical considerations Permission to carry out the study, indeed the request for it, was obtained from the management of Lacor hospital. We ensured that they clearly understood and appreciated the methodology involved. In addition, we sought individual consent from every staff that we interviewed or observed after a thorough explanation of the study and its purpose. Confidentiality, where necessary, was ensured. The plan for dissemination of results was discussed with the management of Lacor hospital and agreed upon. A draft report was presented to the management of the hospital to ascertain the accuracy of data and later the final copies. Limitations of the study One of the main weaknesses of WISN studies is that they depend heavily on the accuracy of the workload records. Hence, in case there were any inaccuracies in the service statistics, they may have affected the validity of our study. However following up on a few sampled statistics, we got convinced that the data we obtained from the hospital were satisfactory. The WISN methodology also uses workload data of the previous year to calculate staffing requirements for the present year. In so doing it creates a potential source of error since the staffing requirements obtained would be as of the previous year. This is however not so worrying since hospital workloads do not change so drastically from one year to the next .To counter this we used the most recent workload data that could be obtained from the hospital. Since we had to explain the methodology and reason for observation of staff at work, knowledge that they were being observed could have influenced the practice of the health workers and thus affected the duration of activities. However, we thought that for a very busy hospital like Lacor, this effect would quickly be worn out as the staff adopted their routine working speed. STUDY RESULTSThe Available Working Time for Nurses in Lacor Hospital The available working time was calculated on the basis of subtracting the non-available working time (absences) from the time available in the year. Table 1 below provides details of the absences that were considered. Table 1 shows that, on average, the qualified nurses had more days of annual leave and off-duty in a year compared to nursing assistants. They also had official annual leave, which the nursing assistants did not have at all. On the whole, the nursing assistants were available for 8 days more than nurses (i.e. 235 days compared to 227 days). Optimal nursing requirements per department Optimal staff requirements were calculated using the WISN methodology. The results obtained are illustrated in Table 2 and 3, for the nurses and the nursing assistants respectively. These two nurse categories were treated differently because they do different work. However, all cadres of qualified nurses were reported to be doing similar activities and thus, we analysed them as one group. To get the present staffing as a percentage of the required, we divided the staff present by the calculated requirements, and converted this into a percentage. From Table 2, it can thus be noted that the hospital required 13 more nurses (i.e. 126 nurses against 139 required or 91%). However, their distribution was skewed so much that one ward had a mere 25% of its required nurses while another had 200% of its requirements. The departments worst affected by understaffing were the AIDS Clinic and the Young Child Clinic while excess staffing was registered mainly in the Isolation ward and the Private clinic. What should be understood here is that the difference shows the number of staff who are required but are missing while the WISN ratio shows the work pressure facing the existing staff. If the WISN ratio were to be converted into percentage, it would represent current staffing as a percentage of those required. Hence, the lower the WISN ratio (tending to zero), the greater the work pressure given that the current staffing would be a smaller percentage of the required staff. Conversely, the work pressure decreases as the WISN ratio increases. At WISN ratio of 1, there is no work pressure at all since the workload equals the current staffing. When the WISN ratio goes above 1, it implies excess staff (by any number above 1) since the existing staff as a percentage of those required will exceed 100%. For instance, a WISN ratio of 1.5 implies that the current staff is 150% of the required staffing, constituting an excess of 50%. The table below shows that Lacor Hospital needed 26 more nursing assistants to meet its requirements and that 21 of these were needed in the paediatric ward alone. Eight of the eighteen departments had more nursing assistants than required i.e. all those above 100%. Here, the range was even wider between 32% and 300% of the staffing requirements. The AIDS Clinic did not require any Nursing Assistants and yet it had 2. This was wasteful deployment of staff who were needed elsewhere. Work pressure among the nursing staff in the different departments It suffices to note that in any analysis of staffing needs, the general picture tends to mask the differing work pressure suffered by the staff in various departments. For instance, looking at the general picture tabulated above, it is easy to conclude that nurses face only 9% of work pressure while nursing assistants suffer only 22%. However, analysis of individual departments reveals discrepancies in work pressure suffered in those departments. Figure 3 and 4 below further demonstrate the extent of imbalances in nurse allocation within departments and provide a more vivid picture of the resultant discrepancies in the work pressure. The positive bars indicate the degree of work pressure while the negative bars the absence of work pressure. Therefore, work pressure among the nursing assistants was highest in the general paediatric and surgical wards while it was lowest in the dental and private clinics. The Isolation Unit, Intensive Care Unit, TB ward, Young Child Clinic and Antenatal Clinic had just the right number of Nursing Assistants for the workload in their departments. We excluded the AIDS Clinic from this analysis. Interdepartmental imbalances in work pressure also existed among the nurses as shown in Figure 4. Work pressure on qualified nurses was highest in the AIDS and Young Child Clinics and lowest in the Isolation and Private clinics. The Dental Clinic and Theatre had just the right number of nurses they needed. Suggested redistribution of Nursing Assistants to even-out the work pressure There was need to redistribute the nursing assistants so that the work pressure gets fairly shared in all the departments. The proposed redistribution would also lead to more appropriate use of staff. To achieve this, we suggested movement of nursing assistants from one department to another as follows: Move 2 nursing assistants from the AIDS clinic to the paediatric ward, 3 from the theatre to the paediatric ward, 1 from the theatre to surgery 1 ward, 1 from the private clinic to the paediatric ward, 1 from the anaesthesia to the paediatric ward, 1 from the maternity ward to surgery 1 ward and 1 from the casualty ward to surgery 1 ward. Move 2 from the general OPD clinic and send 1 to the paediatric ward and another 1 to the medical ward, 2 from the dental clinic to the paediatric ward, 1 from the young child clinic to surgery 1 ward; and 1 from T.B ward to Paediatric ward. After these movements, the staffing in the hospital would be as illustrated in Table 5 below, with work pressure ranging from 0-30 instead of 68 and -200 (i.e. WISN of 0.32 and 3.0) Suggested redistribution of Qualified Nurses to even-out work pressure The following movements would distribute the present workload fairly and even out the work pressure amongst the nurses in the hospital: Move 2 nurses from the isolation ward to the young child clinic; 1 nurse from the TB ward to the Aides clinic; 1 midwife from the antenatal clinic to the young child clinic; 1 nurse from the casualty department to the Aids clinic; 1 nurse from the maternity ward to the young child clinic; 2 nurses from the ICU to the general OPD; 1 nurse from the private clinic to the department of anaesthesia; and 1 nurse from the medical ward to surgery 1 ward. The table below shows that after redistribution, the work pressure among the qualified nurses would be more evenly distributed with a range of only 20. Workload trends in the departments The nursing requirements calculated using WISN methodology are the average requirements for the average workload. But in reality the workload varies throughout the year with seasonal peaks and troughs. This means that even departments that show no work pressure basing on average annual workload could still impose higher work burden on a few staff who work during certain times compared to others. Therefore, the officers responsible for duty-rostering should take workload variations into account if work pressure is to be really shared throughout the year, and posting of nurses should not be permanent. The workload of the hospital for three years (January 2003 – December 2005) was analyzed and an average trend obtained. Figures 5 and 6 and present the workload trend in the wards and out patient department respectively. As noted in Figure 5, the workloads in the paediatric ward vary significantly throughout the year. The workload starts rising in April continuing up to mid May when it remains constant for the next two months. After the peak, the workload starts falling late July reaching its usual level in September. The workload in the other three wards is fairly stable. Hence in effect, a work pressure of 20 which has been provided for the Paediatric ward would come down to zero or even negative in some months. On the contrary, wards with a more stable workload have been left with a work pressure of zero. The YCC has relatively high workload between April and August while the workload in the General OPD is fairly stable, being highest between July and November. The antenatal clinic and theatre on the other hand have stable workloads through out the year. This guided the suggested redistribution of staff in the outpatient departments. DISCUSSION Activity and allowance standards In setting the activity and allowance standards it was of paramount importance to ensure that the quality of service delivery and efficient use of the nursing staff are not compromised. It is on the basis of this that the professional group discussions recommended the reallocation of nursing cadres from one activity to another Letting qualified nurses do activities like daily cleaning and damp dusting, collecting results from the lab and X-ray, washing instruments, collecting user fees from patients etc is inappropriate use of time. These activities consume a substantial amount of nurse's time and yet they could be done equally well by other staff categories that are either more available or less costly to remunerate. Delanyo (2005), while studying wastage in the health workforce in Africa, found that not only are health workers scarce but their full work potential is never realized because of misapplied skills and lack of supervision. This culminates into high costs on the human resources that can be minimized by ensuring efficient and appropriate use of staff. In cases where lower cadres of staff do activities meant for nurses, the effect is not on cost or efficiency but the quality of service delivery. So if the hospital is to ensure continuous quality improvements then the use of appropriate staff has to be guaranteed. Involving the nursing staff in work that is completely out of their training e.g. collecting user fees from patients might not be entirely wrong if the benefits of doing so have been weighed against the opportunity cost of diverting the nursing staff from their technical work. If such instances are few and take a negligible amount of the nurse's time, and there are no major concerns about the quality of that service, only then can this be overlooked. If other work consumes a substantial amount of time or the cost of using the nursing time is higher than the alternative or there are major concerns about quality, then recruitment of the appropriate staff is strongly advised. Some non-nursing activities such as collecting user fees might also involve ethical dilemma. For instance if a patient cannot pay, how far can a nurse go in trying to get the fees? It was not possible in the analysis to calculate how much of the time of nursing staff is spent on non-technical activities. This result would have provided a guideline on how much time of nursing staff is used inappropriately and how many cashiers would be needed in the hospital. Calculating the staffing requirements for the cashiers would also need a WISN study for this cadre of staff. It is imperative to note that most activity and allowance standards were not set to reflect the ideal situation. That would have produced the ideal staffing requirements but might have been unrealistic, unachievable and unlikely to be used by the hospital management. Rather, they were set basing on what was observed or agreed upon with expert professionals. Nevertheless, they compared well with other standards set elsewhere in countries of similar settings. For example attending ward rounds was set at 4 minutes per patient in Papua New Guinea, 5 in Sri Lanka and 10 minutes in Tanzania (Shipp, 1998). We set it between 5-8 minutes depending on the ward. In future, the standards could be revised towards the ideal so as to ensure continuous quality improvement without compromising the efficiency of staff use. Since most studies done do not show the detailed breakdown of all the activities in the hospitals with their set standards it was not possible to make a comparison in the set standards activity by activity. Besides, activities vary from country to country, from one hospital level to another and from ward to ward because of differing morbidity patterns and level of technological advancement. So it is not possible to have the same activity standards for all activities even in the same hospital (Shipp 1998). For example wound dressing in Surgery 1 ward was set at 15 minutes per patient while it was 10 minutes in Surgery 2 ward, because the former had patients with septic wounds who needed more time for dressing compared to the latter, with clean wounds. Available working time The available working time which is the time actually spent working was obtained by reviewing personnel records and from the employment manual to obtain staff absences. The AWT time was different for nursing assistants and nurses. This trend has also been observed in other countries and it is because each staff cadre has different days off duty or entitlements depending on their terms of service. The 227 and 235 days available for work for nurses and nursing assistants respectively are comparable to what was used in many studies. Hossain and Alam (1999) while using the WISN in Bangladesh calculated the AWT for nurses to be 205 days while Ozcan and Hornby (1999) used about 199 days in Turkey. Shipp (1998) used a range of 228-248 days while Namaganda (2004) used 246 days in Uganda. It suffices to note that AWT largely depends on the terms and conditions of work of the country and the organization under study, all of which tend to vary. According to the employment manual for Lacor Hospital, which spells out the terms and conditions of service for personnel, a permanent staff should not work for more than 45 hours a week i.e. approximately 5.5 days a week. Each staff is entitled to annual leave depending on his / her level (Lacor 2001). If that were to be the case then the nursing staff would be expected to work between 238-264 days a year. But there are some unavoidable circumstances like sickness and other absences that keep the staff away from work. Delanyo (2005) states that the average of 2.4 days spent on sick leave as was found in Ghana was high and is synonymous to wastage of staff time. However, we contend that the duration and frequency of sickness absenteeism depends partly on the environment, socio-economic and technological development of a country. Hence even the 3 days found in Lacor hospital plus the days away due to compassionate leave and maternity leave are acceptable in the circumstances. Actually, they are far less compared to the 15 days sick leave used by Ozcan and Hornby (1999). An average of 4 days of official absences for nurses, which include external meetings and workshops, means that substantial amount of nurses' time is spent on these activities hence diverting them from their core activities. Effort should be made not to exceed this level because in reality, it could be only a few nursing staff spending more days in workshops, leaving the rest of the work for the others. Although training provides skills, workshops have been found to provide perverse incentives in poor countries due to the generous allowances received by participants (Delanyo, 2005). Staff shortage As noted in the results, the staff works under some degree of pressure in some departments and this pressure will persist even after the staff redistribution from departments with less pressure. This means therefore that the problem of staff shortage is real for both nurses and nursing assistants. Hence, it can be argued that even after redistribution, the nursing staff will not be able achieve the required quality standards without work pressure unless their numbers are increased accordingly. The shortage of nursing assistants was twice that of nurses with nursing assistants working under more work pressure than the nurses. This leaves a possibility for nurses to help out the over-burdened nursing assistants leading to inappropriate and inefficient use of the nurses. However, if the required number of nursing aides was recruited, these problems should be solved and the scarce nurses used more efficiently. Despite the nursing shortages and the high work pressure, the workload was being accomplished. This could have two meanings: either the work was being accomplished with a compromise on quality of service delivery or somehow the nursing staff was overburdened or getting help from some other staff cadres. In the case of Lacor Hospital, the extra nursing workload was being done by the student nurses. The student nurses could, therefore, be a useful resource to the hospital if well managed. This would entail close collaboration of the hospital with the school in order to agree on how many students to be released to the hospital each day for some shifts. This number has to be constant so that the ward managers can be able to roster the students with other staff on the ward. Final year students and those on registration courses could be very helpful in relieving the nurses because they need less supervision while the beginners could help the nursing aides as they get oriented to the hospital work environment. This, however, should be balanced with other demands on students such as class work and community practice. Moreover, careful supervision would need to be in place to guarantee quality. Thus, hospital management may need to consider training some staff in student supervision. Inappropriate use of available staff Because of imbalances in the staff mix between nurses and nursing assistants in the departments, there were cases where nursing assistants were doing work meant for nurses which could compromise the quality of services rendered in the department. In other situations, the nurses were doing work meant for nursing assistants e.g. daily cleaning, making beds, washing instruments etc which leads to inefficient use of this scarce resource (SARA, 2003). This work can be done well by a nursing assistant and the nurse may just need to supervise to ensure that it is done well. Not only are trained health workers scarce but they are also comparatively more expensive to remunerate. It is therefore important that they are used efficiently and effectively by limiting their use to more technical work for which they cannot be substituted. The other instance of inappropriate use of staff was in using the nursing staff to collect user fees from patients. This creates a shortage because whereas the nursing staff is expected to be doing the nursing work, she/he is diverted from this to do work which could most appropriately be done by a cashier. Other than consuming a considerable amount of time meant for nursing work, it also creates a problem in financial management, because the nursing staff lacks knowledge in financial management and can create problems of adherence to proper financial management procedures. Work pressure among the nursing staff Work pressure varied by cadre from department to department. It should be noted that work pressure is not constant through out the year. What is illustrated in the figures and tables is the average pressure but in actual sense, there are times when the pressure is much less or much higher than illustrated. This is because work pressure depends on patient flow. When patient follow is high like is the case between April and August for the paediatric ward and YCC, work pressure is conversely very high. Patient flow is relatively higher from July to November and therefore the work pressure is higher than average in these months. During periods of high patient flow it is not advisable for staff on the ward to be given annual leave if it can be avoided. This would ensure availability of all staff to handle the increasing work load/pressure. Likewise, some departments such as the isolation ward have few cases in a year hence a low workload and subsequently requiring few nursing staff who are inadequate to run the ward during busy periods. So during such times, one or two more nurses may have to be borrowed from other wards which are less busy at the time. The WISN methodology works with prudent management. It is therefore incumbent upon managers to ensure that during times when a ward has no patients, the nurses are transferred to other wards which are busier at that particular time. Alternatively, that is the best time to hold training sessions, short courses and workshops. Conclusions The nursing numbers obtained were the requirements to cover the annual workload assuming that patient flow was about average throughout the year. In reality however there are peaks and troughs in workloads meaning that even with the optimal nursing numbers, there would be times when the nursing staff could be under pressure and times when they would not. There was a real staff shortage of both nurses and nursing assistants in hospital, and the shortage of nursing assistants was twice that of nurses. However, the shortage of nursing staff was in part being relieved by the student nurses from the nurse training school. There was inappropriate use of both nurses and nursing assistants in the hospital. This either led to inefficiency in cases where nurses were used for activities that could be done by lower level cadres or could have compromised quality in cases where nursing assistants were doing the work meant for qualified nurses. The nursing staff is working under some degree of pressure to accomplish the present workload. This could pose a negative effect on the quality of work that the nursing staff was providing. It, also, could have a negative impact on staff motivation and could easily explain the high turn-over of this cadre of staff in the hospital. Staff inequalities existed among the nursing staff and between departments of the hospital in terms of work pressure. In some departments, the staff was highly overstaffed while in others, they were highly understaffed. It might be necessary to assess whether there are staff in equalities within departments to minimize the negative effects it has on staff morale. Recommendations The hospital management was advised to consider redistributing the present nursing staff among the departments as suggested so as to even out the work pressure and solve the problem of staff inequalities. The management of the hospital and the nurse training school could work out a modality for the school to provide a specific number of students to the hospital throughout the day. Such students would then be deployed as staff to help reduce the work pressure among the nursing staff. The hospital management also needed to consider recruiting more nursing staff as calculated by the WISN. Nursing aides would be the priority staff to be recruited since their shortage was twice as much as that of the nurses. The hospital management was also advised to consider recruiting more cashiers and records assistants so as to relieve the nurses of this non-technical work. This could lead to more appropriate use of the nursing staff and reduce their work pressure. The Matron and heads of departments were advised to consider planning annual leave to their staff in periods when workload is low. This would entail a critical workload trends analysis per department. Finally, close supervision and job descriptions for the different cadres of nursing staff could help in reducing the inappropriate and inefficient use of staff. Training of all departmental heads in the use of the WISN would certainly be beneficial to the hospital. Suggested research areas
References
The following images related to this document are available:Photo images[hp08003t5.jpg] [hp08003f6.jpg] [hp08003f1.jpg] [hp08003f2.jpg] [hp08003f3.jpg] [hp08003f5.jpg] [hp08003t2.jpg] [hp08003t3.jpg] [hp08003t4.jpg] [hp08003f4.jpg] [hp08003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}