 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 6, No. 1, April, 2008, pp. 54-65 THEME TWO: HEALTH SERVICES MANAGEMENT OVERCOMING BARRIERS TO ANTI-EPILEPTIC TREATMENT: A LIFE-TIME SENTENCE? John Odaga*, Luigi Cicciò# and Everd B. Maniple* *Senior Lecturer, Faculty of Health Sciences, Uganda Martyrs University Code Number: hp08007 Abstract Epilepsy, like many other mental illnesses, is more prevalent than is commonly acknowledged. Moreover, its social and economic burden is excessive for the individual, family, health system and country at large. People with epilepsy have low quality of life and productivity. They and their families are stigmatized and discriminated against. Doctors with Africa - CUAMM, has operated a project for epilepsy treatment together with the local health authorities in Nebbi and Arua districts since 2005, aimed at increasing access to free, effective anti-epileptic medicines. Despite the availability of the medicines, the attendance of many enrolled patients has been erratic. This study was done to document the level of adherence to treatment, the reasons for the observed health-seeking pattern and to assess the feasibility of sustainability of enhanced epilepsy treatment services once the project ended. Retrospective analysis of records of all patients registered in 2004 and 2005 was done in order to determine the level and pattern of adherence. A cross-sectional survey of 93 patients, selected according to the documented patterns of clinic attendance, was done to investigate the reasons for the observed pattern of healthcare use. Assessment of feasibility of sustainability was done by interviewing key informants and reviewing records of expenditures on anti-epileptic medicines for 2005. Conducted in 2006, the study shows that about 84.5% of the enrolled patients missed at least one appointment over the two-year period of follow-up, with about one third missing all the clinics since enrolment. A typical patient missed about 60% of all the appointments. The overall attendance level at any given time was at a low 40% (30% for those registered in 2005 and 50% for those registered in 2004). There was wide variation in the magnitude and frequency of defaulting at the different sites. Younger and older patients defaulted more often than the middle-aged groups, just as female patients defaulted more frequently than the male counterparts. The reasons for the poor compliance were multiple, patient-specific and often acting simultaneously. The most critical and cross-cutting included distance from the health facility, family support, persistent health education and individual patient/family counseling. The mobilisers (often epilepsy patients themselves) were pivotal in patient/family education and counseling as well as reminding patients about clinic days. The most important adherence-promoting health systems factors were the regular availability of effective medicines and the vertical nature of the delivery system. There were several constraints working against sustainability of enhanced epilepsy care, including technical competence of the health workers, regulatory limitations that forbid the use of some anti-epileptic medicines at some levels of health care, negative staff attitude and high investment levels in ensuring constant availability of anti-epileptic medicines. Introduction: Epilepsy is more common than a number of conditions often recognised as public health priorities in developing countries. There are as many cases of active epilepsy in developing countries as there are in industrialized countries, ranging from 0.5% to 1% of people. It is the commonest of the severe forms of neurological diseases, and also the commonest of all non-communicable diseases (WHO, 2003a; Scott et. al., 2001). Recent data on the prevalence of epilepsy in Uganda are hard to come by. However, a recent household survey conducted by Doctors with Africa - CUAMM (2004, unpublished) showed that the prevalence of the disease at selected sites in Nebbi and Arua districts of north western Uganda was very high, at 8.7% and 12.3% (about 1 case for every 2 households) respectively. Yet, the burdens produced by epilepsy go beyond the sheer number of individuals affected by the condition. People with epilepsy have lower quality of life and productivity than people with other chronic illnesses. In many developing countries epileptics and their families are stigmatized and discriminated against. Epilepsy threatens the aspirations of the entire family, not just of the individuals with the disease (Baskin and Birbeck, 2005; Scott, 2001). Therefore, epilepsy is a significant public health and socioeconomic burden, requiring urgent action. Despite its importance, resources are often allocated away from epilepsy programmes for conditions generally perceived to be more important. Apart from failure to recognize epilepsy as an important problem, the treatment of epilepsy is very expensive. In India, in 1988, a year's supply of phenobarbitone, the cheapest anti-epileptic drugs [AED], cost about 25% of the average per capita income. The per capita public expenditure on phenobarbitone was estimated at 15 - 20% of the public expenditure on health in China. Thus, it is unlikely that AED could be provided solely by government-funded schemes alone in poor countries. Moreover, private provision of AEDs could cause significant financial hardships to already poor households. Consequently, a large number of those affected go untreated, or are inadequately treated, particularly in developing countries where an estimated 75 to 90% receive no treatment at all (WHO 2003a; Coleman et al 2002). Yet, there is value in such an investment. Recent evidence from both developed and developing countries suggests that most patients could have their seizures completely controlled with the available anti-epileptic drugs (AED) (WHO, 2003; Scott al., 2001). Of much greater concern is the fact that, of the small number that have access to treatment, even a much smaller fraction gets successfully treated, largely because of poor adherence to prescribed medication. Adherence to antiepileptic drugs in patients with epilepsy generally ranges from 20 to 80%; with the adherence for adult patients ranging between 40-60% and for children ranging between 25_75% (WHO, 2003a). Good adherence to treatment is fundamental to the successful management of epilepsy. Non-adherent patients experience an increase in the number and severity of seizures. Non-adherence, therefore, results in wastage of healthcare resources, and reduced quality of life. The Project of Doctors with Africa - CUAMM In 2005, Doctors with Africa - CUAMM, (CUAMM), an Italian NGO, undertook to provide AEDs through a programme that used the local primary health care facilities. Treatment was provided at 7 health centers (level III and IV - Rhino Camp, Offaka, Wandi, Okollo, Koboko, Olujobo, Omugo) and one outreach outpost (Buniababa). Buniababa, is an "under-the-tree" outreach post, created because of the large number of epilepsy patients in the locality, many of whom are integrated Sudanese refugees. The nearest health center (Rhino Camp) is over 15 km away. Counties with hospitals were excluded in the programme because it was felt that the hospitals could provide the service. CUAMM services were mainly directed at remote areas and those with large numbers of displaced or migrant populations which tend to present a special challenge for treatment delivery and adherence. The programme was mainly run by a mobile team of staff from the CUAMM office in Arua town, with two psychiatric nurses from Arua Regional Referral Hospital. The CUAMM staff was responsible for the overall coordination and organisation of the programme, and procurement and storage of AEDs. Quantification of medicine requirements was jointly done with the psychiatric nurses and appointment days were fixed with community representatives. The psychiatric nurses were responsible for clinical examinations, prescribing treatment and monitoring the patients for the outcome of treatment. The staff of the health units operated routine outreach clinics alongside the mobile team and kept records for all the patients. Shortly after the introduction of the epilepsy outreach programme, one selected health worker from each of the earmarked health centers received 2 weeks of training either in the management of epilepsy specifically or mental illness in general. Six of the seven treatment centers (except Wandi) enrolled a community volunteer `mobiliser' responsible for the education of the public and patients about epilepsy, reminding patients about their clinic days (through home visits, community meetings announcements in public gatherings) etc. In addition, the mobilisers provided individual counseling (on the benefit of treatment, self care etc) and were responsible for identifying and referring suspects of the disease and home-based distribution of medicines. The mobilisers were either patients themselves or caretakers of other epileptic patients, who were elected by and on the basis of trust by the patients. Many of the mobilisers were either retired or serving primary school teachers. In some areas, notably Rhino Camp, the mobilisers were people formally recruited as community-based rehabilitation (CBR) officers under an earlier programme jointly run by CUAMM and Community Based Rehabilitation Alliance (COMBRA), a national community development organisation. Mobilisation was voluntary, although the CBR officers were paid a monthly allowance of Shs. 10,000/= (about US $ 5.5). Clinic days were held every 28 days except in a few centres where they were twice a month. Treatment was free at the point of delivery for all the patients. The common medicines used were oral phenobarbitone, phenytoin, and carbamazepine, whose unit cost increases in that order. Treatment was often initiated with phenobarbitone; where necessary, this was progressively complemented or substituted with either of the latter two medicines depending on the patient's response. Folic acid was always provided, as adjunct therapy. It was observed that, despite the free treatment with effective medicines delivered closer to patients, adherence to treatment was very irregular. There was a very high drop-out rate. Moreover, the externally-funded programme was coming to a close and there was concern over its continuity and financial and technical sustainability. This study, commissioned by CUAMM and conducted jointly with a team from Uganda Martyrs University's Faculty of Health Sciences, was intended to (a) determine the extent and pattern of adherence (or non-adherence) to anti-epileptic drug therapy by epileptic patients registered as of December 2005; (b) investigate the major factors influencing patient adherence to treatment (c) investigate the feasibility of sustaining the programme once CUAMM support ends. It was conducted in June 2006. Methodology We retrospectively analysed the attendance records of patients registered during 2004 and 2005 respectively and categorized the patients into three groups i.e. those who never missed any appointments, those who missed all appointments and those who attended erratically. Subsequently, we undertook a cross-sectional survey of patients in the different categories above to investigate the factors likely to have been responsible for the observed health-seeking pattern. We plotted drop-out patterns over the follow-up periods (the probability of defaulting, or remaining on treatment after registration) and estimated the number of times a typical patient was likely to default over a ten month period of follow up. We interviewed key stakeholders to determine the sustainability of the project without CUAMM support. Study Sample We sampled patients with different attendance patterns to investigate the reasons for their behaviour pattern. The sample size for the survey was obtained using Kish's formula
where: p = proportion of patients who never missed
any appointments after registration, estimated at 40%
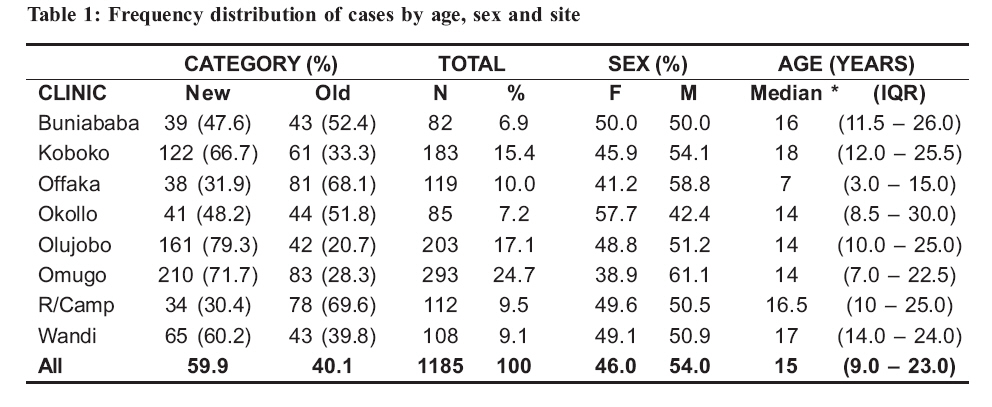
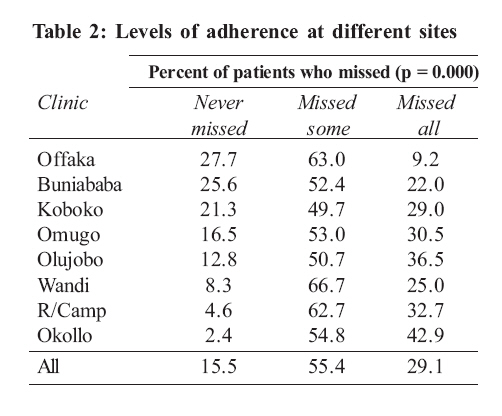
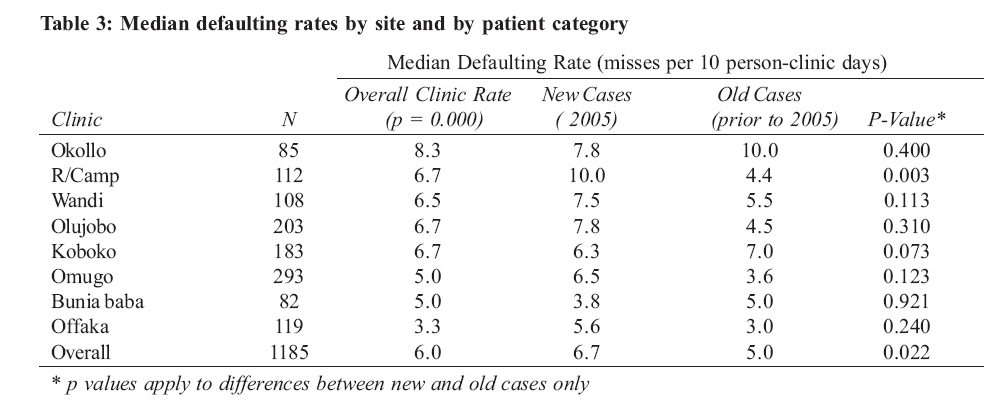
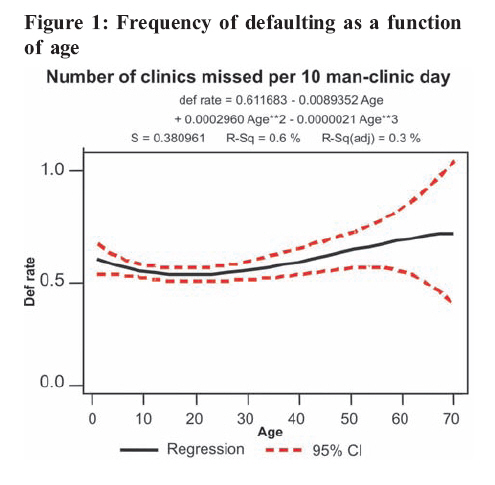
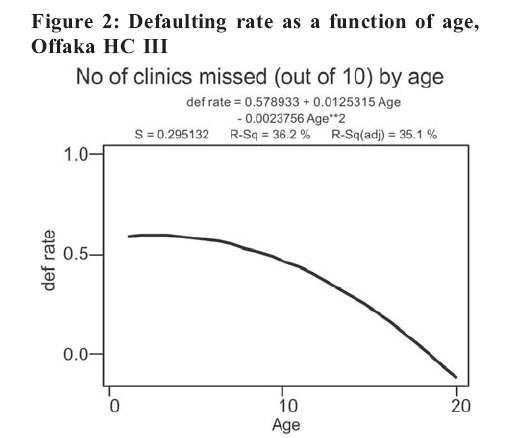
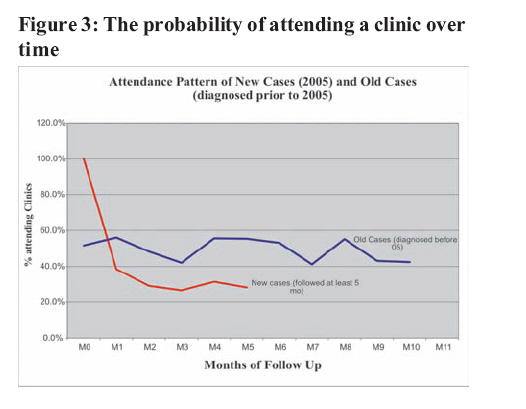
(as per WHO, 2003) Basing on the formula and values above, the estimated sample size was 95 patients. Because of practical considerations, (e.g. the availability of patients in different categories created [defined below]), the minimum sample size was adjusted to 93 cases (as explained in the section on the sampling technique). Eligibility for the interview The attendance behaviour of "new" cases (registered during 2005) and "old" cases (registered in 2004). Those registered during 2006 were excluded because of the short duration of follow up (maximum of 6 months by the time of the study). The mean (and median) follow up periods for new and old cases were 5 and 10 person-clinic days respectively i.e. we analysed the attendance of a typical new case in a period of 5 months (5 clinic days) and that of a typical old case for a period of 10 months (or clinic days). Only those new cases with complete data spanning at least 5 months and only those old cases followed for at least 7 months were considered for the interview. This was dictated by the completeness of the data since very few cases had been followed fully for more than 7 months. For interview purposes, the cases were further grouped into three categories, namely `fully adherent patients' `irregular attendants' and `non-adherent patients'. A `fully adherent' patient was one who did not miss any appointment during the period considered. On the other hand, a `non-adherent' case was one who, after registering for treatment, missed all the subsequent appointments during the observation period. An irregular attendant was any patient who fell in between. Because of the large number of this latter category, only those who missed about half (i.e. 3 and 5 respectively) of the appointments during the period of observation were selected for the interview. Thus we had 6 categories of: a) New fully adherent cases: those registered during 2005, followed for at least 5 months (clinic days), and never missed any appointments during the period of follow up b) Old fully adherent cases: all those registered prior to 2005, followed for at least 7 months during 2005, and did not miss any appointment during the observation periods in 2005 c) New irregular attendants: those new cases (defined above) who missed exactly half of their appointments d) Old irregular attendants: old cases (defined above) who missed half of their appointments during the period of observation (defined above) e) New non-adherent cases: new cases (as defined above) who missed all appointments during the period of observation f) Old non-adherent cases: old cases (as defined above) who missed all appointments during the period of observation (defined above) A total of 328 patients satisfied the criteria above, out of whom 95 cases were to be selected for the survey. Sampling techniques The eligible cases were selected from patients' attendance records. Where the number of eligible cases at a particular treatment site was smaller or equal to the calculated sample size of a patient category, all the cases were included in the study. Where the number of eligible cases exceeded the required sample size of a given category, cases were selected by way of random systematic sampling. Generally, the number of cases selected was proportionate to the size of each category at each health center. However, adjustments were deliberately made to ensure that all categories were represented, and that we did not have an excess of one category. We also wanted to keep the number of cases at each health center to about 12, the number thought to be the feasible workload for interviews in one day. After all the due considerations, we arrived at a sample size of 93 cases. As expected, some of the selected patients were not available for various reasons (migration, death, etc). In such cases, they were conveniently substituted with cases in similar categories, until the quota for each center was filled. Therefore, we were able to raise the sample size of 93. Results General Characteristics of the Patients A total of 1,185 patient records were evaluated and most (about 60%) of them were new (registered in 2005). However, the proportion of new and old cases varied from site to site as shown below: Overall, there were more male patients than females, although this pattern was not consistent at all the sites. The patients were generally young at all the sites, with the overall median age being only 15 years. The patients registered at Offaka HC III, were exceptionally young, all of them being under 20 years of age. Adherence rates a) Level of adherence Table 2 summarizes the patients that exhibited different types of health-seeking behaviour at different sites. The table shows that, across all the treatment sites, only 15.5% of the patients were able to attend all subsequent clinics after registration. This means that 84.5% of all the patients missed their subsequent appointments at least once over the period of observation, with about one third dropping out permanently. There was a wide variation in the attendance rates across different clinics. For example, Offaka, Buniababa and Koboko had the highest overall attendance rates of all the centers (with at least 20% of registered cases attending all the follow-up clinics). Offaka had the best overall attendance rate, with the highest rate of fully adherent patients and the least rate of non-adherent patients (those who never attended any follow up clinics). Okollo had the worst adherence record, with the lowest rate of fully adherent patients and the highest rate of non-adherent patients. Offaka, with the best adherence record, and Okollo, with the worst records, are found in the same county, a few kilometres. apart, with the same socio-economic mix (including ethnicity) and are at the same referral levels. b) Frequency of defaulting Table 3 summarises the number of appointments missed by a typical patient if that patient was followed for 10 clinic days after registration. The Clinics were run once every month. The table below shows that, overall, a typical epileptic patient missed more than half of the appointments (6 out of 10). However, there was a wide variation between the different treatment sites in the number of appointments missed by a typical patient; at least 50% of the patients across all clinics missed from as low as 2 clinics to as high as 10 out of 10 clinics (IQR = 2.0 - 10.0; p = 0.000). The highest overall rate of defaulting was experienced in Okollo where a typical patient missed more than 8 clinics out of 10 appointments. It was lowest in Offaka, where the number of clinics missed by a typical patient was just about 3 out of 10. In Rhino Camp, the new cases missed all their appointments in the period under study. Overall, there was a significant difference in defaulting rate between new and old cases, with a typical new patient missing about 7 out of 10 clinic days, compared to 5 out of 10 for an old case. c) Frequency of defaulting by Sex Category There was some (practical) difference in the defaulting rates between females and males, with the former missing 64% of all their appointments compared to only 55% for the male patients. This pattern was observed at all the sites except at Offaka HC II where it was reversed. The biggest difference in defaulting rates between the sexes was observed at Buniababa (F = 70%; M = 25%) and Okollo (F = 86%; M = 71%). d) Frequency of defaulting by age Figure 1 shows the variation in defaulting rate by age across all the centers. Generally, age was not a strong predictor of adherence to treatment at most sites, accounting for only 0.3% of all the missed appointments across all clinics. The effect of age on clinic attendance was most notable at Offaka (accounting for over 35% of all the clinics missed by a patient, without taking all other possible factors into consideration), where, a young age was a strong predictor of high defaulting rate, as shown in Figure 2: According to the mobilisers and the health workers at Offaka, a frequent defaulter here was likely to be a child, for whom the decision to seek or continue with care depended on some one else. S/he was also likely to be a new case whose family had not (yet) been sensitized enough. [Reasons underlying adherence pattern are elaborated below] b) Attendance pattern over time Figure 3 shows the probability of attending a follow-up clinic over time for new and old cases. It also shows the rate at which the different categories fall out over time. These probabilities are equivalent to the proportion of the different categories of patients who are still adherent at different points of follow up. Of the new cases, only those followed for at least 5 months were considered in this analysis. The graph shows that, of the newly registered cases, under 40% returned for the next immediate appointments. The massive decline in the number of patients honouring subsequent appointments continued, reaching the lowest level at about the 3rd appointment (3rd month) from the date of registration. There seemed to be a slight rise in attendance four clinic days (months) later as shown by the slight bump in the graph for both new and old cases. This trend was observed in nearly all the treatment sites. It can also be noted from the same graph that about 50% of all the cases registered prior to 2005 continued with treatment. The pattern of care-seeking amongst this group seemed to follow exactly the same pattern as described for new cases, with a typical pattern repeating itself cyclically. The rate of clinic attendance generally declined from about 50% of all old cases, to just above 40%, 3 clinic days (months) later. This pattern is repeated again. However, it should be noted that the patterns of care-seeking among old cases at the various specific sites were more haphazard than the cyclical pattern presented. Main factors responsible for the observed adherence level and pattern In order to understand the main reasons responsible for the observed attendance levels and patterns, we interviewed the healthcare providers, the patients and/or attendants, and the patient mobilisers, a number of whom were patients themselves. In all cases, the aim was to understand the extent to which various factors were at play at various centers. Some of the most frequently mentioned factors are summarised thus, in order of frequency: a) Long distance from the clinics Long distance from the treatment centers was cited several times by both the patients and health workers as the main reasons for frequent defaulting, especially by new cases who were still experiencing fits frequently, and by children. Many of the patients had to walk long distances (10 - 20 kms) to the clinics, wait for hours before they were seen, and walk back late on empty stomachs. Some patients experienced fits during the clinics and attributed them to the stress of walking long distances, long waiting time and staying hungry the whole day. Patients walking long distances often had to be accompanied, especially if they were children or were experiencing frequent fits. Because of the time cost involved, the caretakers often had to make trade-offs between attending the clinics and other commitments. b) Time management Poor time management by health workers was said to be one of the reasons for the long waiting time. This was common in units which were very distant from Arua town, the operational base of the mobile care team. Sometimes, patients had to wait long for the mobile team, and so the clinics often started late. It was noted that this had discouraged some patients, including those living close to health center "Time management is a key issue. If the personnel running the clinics were residents here, work would be starting early. If possible, all drugs should be stocked here. … need a separate room where we can organise from, proper record keeping here at the Health Centre".[one patient-mobiliser] c) Effect of treatmenti. Improvement on treatment The perceived improvement resulting from regular medication had a double-edged effect on adherence rate. On the one hand, it was reported to "make patients or their caretakers relax". Once patients have shown some improvements, medication became less important compared to other commitments, "… such as funerals" [one staff], especially where the decision to seek care did not rest with the patient, e.g. young patients. This was one of the major reasons for irregular attendance by old cases (those who had already been on treatment for long). "Many parents wait until the patients have developed fits again, and then bring them" [a staff]. On the other hand, the perceived improvement strengthened the resolve of a number of patients (and/or their care givers) to remain adherent until complete relief of symptoms. A number of them had resumed normal life in the community and desired to get on with life uninterrupted by attacks of seizures. To them, medication had given them a new lease of life. ii. Delayed or lack of improvement According to a number of patients whose seizures were under control, improvements, unfortunately, were rarely immediate, often coming after prolonged and regular treatment. Quite often, it took the health workers a while to get the right medication and the right dosages for a particular patient. Sometimes the seizures got worse as the medications were changed from one type or dosage level to another. Newly registered patients, in particular, often expected immediate improvements. If that did not happen, or their conditions got worse instead, they quickly got discouraged and dropped out, or attended irregularly, often when their conditions were really bad. This was noted to be more likely among those who were still skeptical about the benefits of western medicine and with misconceptions about the causes of the disease. d) Forgetfulness and effectiveness of reminder mechanisms The normal practice was for the health workers to inform the patients and caretakers attending a clinic of the next clinic day and date. Although the majority of the patients/care givers were able to remember these appointments, a number of patients often forgot them because of the effect of the disease or medication. Sometimes the patient or care giver found it difficult to keep the dates because they kept changing. It was noted that a number of them needed to be reminded close to the clinic days. One of the tasks of the mobilisers was to inform or remind all patients/care givers about the next immediate appointments, close to the dates. This was done by either passing on the message through public gathering, or through the local council officials, or by directly visiting the patients' homes. Information passed through public places did not always reach the intended targets. As expected, door-to-door reminder of patients proved the most effective method. At Offaka health center, this was the single most important reason for the good adherence level. The highly motivated mobilisers engaged in routine home visits, one of the reasons for which was to remind the patients about the appointment dates. The importance of door-to-door mobilization and reminder of patients was acknowledged at all the centers. e) Family support and counseling Family support was observed to be another crucial single factor responsible for the observed adherence levels and patterns at all the sites. In fact, every reason given for the observed attendance pattern seemed confounded by two reinforcing factors—the extent of family support and the extent of counseling available to the family and individual patient. Family support included acts like accompanying patients to the clinic, reminding them of the clinic days or supervising their medication, etc. The extent of family support partially depended on a number of factors including the extent of family cohesion. Quite often the responsibility for care was taken by the female spouse, while the male partner was either apathetic or overtly against formal medical treatment. Where mobilisers were successful in counseling the family members, the patients were able have regular treatment. f) Negative beliefs There was still widespread belief that epilepsy was the result of witchcraft or a curse and could not be cured. This belief was noted to be stronger among new cases, or those who had not yet experienced any improvement. A number of patients in this category attended clinics simply "because the health worker asks us to do so" [one patient] g) Displaced and Migrant population Some of the treatment centers had large catchment population of internally displaced people, or refugees from Sudan. In addition, some of the patients were people who had temporarily migrated to the catchment areas in search of suitable land for cultivation. It was very difficult for groups like these to comply with treatment as they were quite mobile. This was one of the main reasons for the poor adherence rates at Okollo, Rhino Camp, Olujobo and Koboko. Nearlly all of the defaulters at Buniababa had either died or emigrated from the area. h) Perceived Financial barriers All forms of AED and care related to the condition were provided free-of-charge to all patients, and this information was made abundantly clear to all the patients or care givers. However, each of the sites had an association of patients aimed at generating income for the groups or continuing funding the programme in the event of no external funding. The association expected all the patients to pay 3,000/= each (about US $ 1.70) for registration and, at some centers, an additional 2000/= (about US$ 1.1) for proposed income-generating projects. Payment by installment was acceptable. Although these payments were not a pre-condition for accessing treatment but rather to create a fund for sustaining the treatment in the event of loss of external funding, this fact was not well understood by all patients, some of whom subsequently opted out of treatment. At one center, the patients were required to pay 500/= (about US$ 30 cents) each per visit, to the chairperson of the group, or the mobiliser. Adherence at this particular center was one of the poorest among both the new and old cases. The monthly charge was highlighted as the single most important factor for the poor attendance at this site. The evidence shows that attendance has been improving fast since the abolition of that monthly fee. i) Health education and the significance of personal testimonies Regular and sustained health education, particularly individual and family counseling, was crucial in ensuring and reinforcing adherence. Health workers routinely provided the correct information regarding all aspects of the condition. These were reinforced by the mobilisers, whose messages were better received by the patients and their care givers because of their closeness and similar experiences, as many were patients themselves. Mobilisers who had shown good improvements provided strong and inspiring testimonies to many who were still skeptical about the benefits of medication. "I use myself as a living example to the doubting patients. I have lived with them, and they see the improvement I have had. I am living a normal life. I ride unaccompanied, and without any more fears of seizures. For those who know me, I don't have to speak many words about the benefits of treatment…" [one patient-mobiliser in Omugo] Effective mobilization, and sustained counseling by motivated mobilisers were responsible for the high rate of regular attendance in Offaka. j) "Being a new case" Nearly all the factors operating at individual, family and community level were operational in a new case at the same time. A new case was likely to be one with misconception about the cause of the disease, skepticism about the benefits AED, inadequate health education, and poor family support (because of lack of awareness) k) The quality of service delivery We looked at the range and frequency of services delivered, the players involved, their attitude towards the patients, effectiveness of communication or counseling about the various aspects of the condition and availability of the medicine. We found that medicines were always available. On only a few occasions, the necessary medicines required by some patients were missing, and such cases had to be referred to Arua Hospital. Clinics were very regular, 28 days apart and rarely missed. Indeed, the mere knowledge of assured availability of free and effective medicines, within reach, was one of the reasons why some patients attended clinics regularly. Health education and counseling seemed adequate and effective. Most patients interviewed could describe the main facts about the disease and its treatment. Information was mainly provided by the mobile team, but reinforced by the mobilisers. A number of patients and mobilisers conceded that non-adherence could not be blamed on lack of or inadequate health education. l) Summary The factors presented above are the major ones captured from patients/caretakers, health providers and the mobilisers. In almost all cases, there was more than one factor, interacting to determine the health-seeking decision of the patients, although to different degrees. Similarly, some factors were more dominant at some centers than the others. The main factors operating at the various sites are summarised in the table below. Sustainability without external support The possibility of the programme continuing without Doctors with Africa - CUAMM support was examined here along four parameters a) Sufficiency of local budget size (at facility level) b) Staff involvement and attitude c) Technical capacity at the health facility d) Willingness of the existing facility-based and community structures to continue with the programme a) Budget size The table below compares the annual expenditure on AED for two treatment centers in 2005, with the estimate of the annual drug budget and the average utilization rate over the periods of study. At Okollo, about 12.4% of the medicines budget would need to be made available for AEDs, for just about 15 patients in a year. At Offaka, about one quarter of the budget would be needed for the same purpose in a year to cater for only about 80 patients. If the number of patients increased over the years, and if adherence rate also improved, even moderately, the share of the AEDs expenditure could be well over 30% at most health centers. Given other priorities, this is not feasible. b) Staff integration and attitude There was generally very low local staff involvement in the running of the clinics. The local health workers played a passive role, of helping to store patients' records or providing space for the clinics, and storing limited stocks of medicines. At best, most of them only provided treatment for new cases, or for continuing patients, who reported between the clinic days. The clinics were largely "mobile-team-run" to the extent that the overwhelming majority of the local staff associated the project with Doctors with Africa - CUAMM rather than with the health Units. The reasons officially given for the low staff involvement were shortage of staff and workload pressure. However, there was also evidence that many local staff did not wish to be involved in the care of epileptics, viewing it as extra workload for which they expected extra pay; particularly also because the mobile team members received some allowances. Other health workers were, themselves, not free from ignorance and stigma about the disease as they feared that the condition was contagious, and therefore preferred to refer the patients to other health units. The general impression we got was that most of the staff are really not interested in caring for epilepsy patients. Even if funds were to become available, probably very few staff would be committed to continue with the project at the level at which it is presently being implemented. c) Technical capacity at the units Many of the centers treating the patients were run by staff not qualified, and therefore not authorized, to stock or dispense phenytoin and carbamazepine. They are only permitted to stock and dispense phenobarbitone. Any patients requiring the former two medicines are supposed to be referred to a hospital or HC IV. However, within the project, it was possible to provide the phenytoin and carbamazepine to patients even at lower health centers because the epilepsy clinics were run by the technically qualified and authorized staff on the mobile team. Therefore, even if funds were available, treatment of the patients at the lower level units, with the more effective and expensive medicines would not be officially accepted. If all cases that required the two medicines (phenytoin and carbamazepine) were to be referred to the Health Sub-district [HSD] headquarters, this would impose a high demand on the latter given the large number of cases in the catchment areas. d) Willingness of the existing community infrastructure The programme extensively made use of the local community structures (mobilisers, Local Council members, etc) who said they would be willing to continue to volunteer. However, it was also apparent that many of them would expect some form of incentives (e.g. means of transport, token allowances, etc) in order to do so. At Offaka, whose stellar performance was partly attributed to effective mobilization by `motivated mobilisers', it was hinted that the morale of those mobilisers was on the decline because the token allowances they used to receive had been scrapped. From the foregoing, it is therefore not foreseeable that the project can continue in the manner, quality and scale being provided at the moment DISCUSSION This study shows that the number of patients who missed clinic appointments during the period studied was extremely high, despite the availability of very effective AEDs, provided free at the point of delivery. Further more, the frequency with which the patients missed appointments was also very high (over 60% of appointments). Adherence to AED has been shown to be very low and varying widely elsewhere, ranging from 20% - 80%, even in developed countries (WHO, 2003; Wagner et al., undated). Poor adherence impairs the ability of health care programmes to achieve the expected outcomes (WHO, 2003). Therefore, if efficiency were the main guiding principle in running such a treatment programme, one would find these results very disappointing and frustrating. On the other hand, given the stigma associated with epilepsy, treatment programmes should be initiated, expanded and/or continued over the long term on the basis of altruism. Moreover, this study also suggests that running epilepsy treatment programmes over the long term seems to improve adherence—as seen by better adherence rates among `old' cases as compared to `new' ones. A new case was likely to have misconception about the cause of disease, benefits of treatment, inadequate education and family support. At Offaka, for example, negative beliefs were not as significant as were noted in many other centers; the main reason being protracted health education that started with another project prior to this particular one. Hence time is required to `win the minds and souls' of both the patients and public through health education and counseling. This implies that better benefits (in terms of improved compliance) are likely to accrue if treatment was sustained for a long time, rather than provided as short-term projects. There is also an ethical dimension related to the provision of anti-epileptic treatment as short-term projects. Withdrawal of treatment is normally followed by very serious rebounds, with many patients becoming worse than they were before treatment. From a moral standpoint, it would be better not to have started the treatment in the first place if it was clear from the beginning that treatment would be short-term. Therefore, frustrating and expensive as the project may be, there is a moral obligation to ensure its continuity over the long term, or to explore ways of doing so, hence the need to move from short-term projects to long-term programmes in such cases. However, this study also illustrates the complex nature of adherence as a phenomenon. The factors determining patients' compliance were largely patient-specific, and varying from one programme site to another, and often confounding one another. Therefore, it is difficult to recommend a `one-size-fits-all' strategy. Nevertheless, there seemed to be some critical success factors that cut across all facilities and individuals. A key lesson learnt is that for this type of programme to be successful, family and community support are crucial, particularly where patients are reliant on caretakers (e.g. children, and those with frequent fits). The significance of family support in ensuring adherence of adolescents AED has also been demonstrated elsewhere (Kyngas and Rissanen, 2001). The use of patients or caretakers as mobilisers-cum-counselors was found to be critical in ensuring family support and promoting patient adherence. They were able to address the barriers operating at individual and family levels, where the health workers do not usually have much influence. However, volunteers are not inexhaustible resources, especially if they are patients themselves. To be effective and committed over the long term, they need to be motivated, however symbolic the modality may be. It was clear that mobilisers who received some token allowances were better motivated than the ones that did not. What are necessary for them are some form of transport means (e.g. bicycles) and/or money for lunch. This could make the programme expensive, but cost-effective, and justified for the cause. It is often argued that non-availability of AEDs is the most important obstacle to the care of people with epilepsy (Scott et. al., 2001). Unlike what is often the case, the usual health systems related barriers were paid due attention to in this treatment programme; e.g. making treatment free at the point of delivery, ensuring effective medicines were available nearly all the time, tailoring treatment to patients' needs and providing protracted health education. Treatment was prescribed and regularly reviewed by appropriately qualified staff, who were dedicated and empathetic. These factors worked positively to encourage some patients to continue treatment. However, it should be noted that this was partly possible because of the vertical nature of the programme. It is highly doubtful that the same level of diligence would be maintained if the programme were to be fully integrated into the existing health system as part of the minimum health care package, the main reasons for the skepticism being not only workload, financial and regulatory constraints highlighted before, but also because of the attitude of staff at some of the health units. Hence, the best way forward, would be to keep the programme semi-vertical, as a joint venture between Doctors with Africa - CUAMM and the local health system, at least in the short to medium term. Distance from the facility featured prominently as one of the important barriers to keeping clinic appointments. Decentralization of treatment to more health centers has the potential of improving adherence, as evidenced by the establishment of Buniababa out-reach post. However, given the current vertical nature of the programme organization, it may be operationally difficult to effectively operate any extra treatment centers. One option to explore, perhaps, is the use of community treatment volunteers. Some mobilisers, with good level of education, could be trained to do so. Community treatment volunteers have been successfully used in the TB treatment programmes (WHO, 2003b), and are being tried in the treatment of HIV/AIDS. Even in Uganda, they have been used for home-based management of fever, and for distribution of medicine for the control of onchocerciasis. The use of community volunteers to treat epilepsy patients is reported to have resulted in an adherence rate of 82% in Kenya, with a number (53%) of the patients experiencing a cessation in seizures over a 6 - 12 months period (Scott et. al., 2001). Empowering community volunteers to give treatment could also address the concern for time management. That is, they could be authorized to dispense medicines for patients who have already stabilized to allow the mobile teams to concentrate on people in early phases of treatment who need more attention. CONCLUSION This study shows that, despite considerable efforts to overcome barriers on the supply side, the uptake of the anti-epilepsy services remained considerably, but not surprisingly low. Most of the barriers to uptake of services were on the demand side, operating at the individual, household and community levels. Most factors were patient-specific and often operating simultaneously. This study also shows that although some of the factors are well beyond the realms of the health system, some of them are still amenable to health programme interventions. For example, protracted health education and individual patient/family counseling was critical in ensuring family support, a strong predictor of adherence. The mobilisers (often patients themselves) were pivotal in patient/family education and counseling as well as reminding patients about clinic days. Therefore, it would seem reasonable to suggest that protracted community-based interventions seem to be the way to go in order to overcome demand-side barriers, irrespective of whether any incentives are patient-focused (e.g. use of various reminder mechanisms), or on the supply side [e.g. use of volunteers to provide medicines focusing on community resource persons]. This study also shows that in the treatment of epilepsy, confidence in modern treatment and good results can accrue only when treatment is sustained for a long time. Therefore, a long term treatment programme is likely to be more effective, and ethical, than a short-term project. Unfortunately this does not seem to be feasible by integrating the current project into the existing health system. It is not foreseeable that the existing local health system can overcome the numerous barriers on both the supply and demand sides. Hence the best way forward would be to continue with the current semi-vertical partnership arrangement between Doctors with Africa - CUAMM and the local health system. The question is whether Doctors with Africa - CUAMM is, or will, be in a position to carry on her side of the `burden' over the medium to long-term, including the suggested incentives. If the project is going to continue for a few more years only, it is also important to re-focus its objectives. There might be need to consolidate the activities at the existing service points to promote adherence and involvement of local staff, rather than expanding to new centers and, eventually, spreading the available resources thinly on the ground. References
Copyright 2008 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp08007t1.jpg] [hp08007t5.jpg] [hp08007t2.jpg] [hp08007t6.jpg] [hp08007t3.jpg] [hp08007f1.jpg] [hp08007f2.jpg] [hp08007f3.jpg] [hp08007t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}