 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
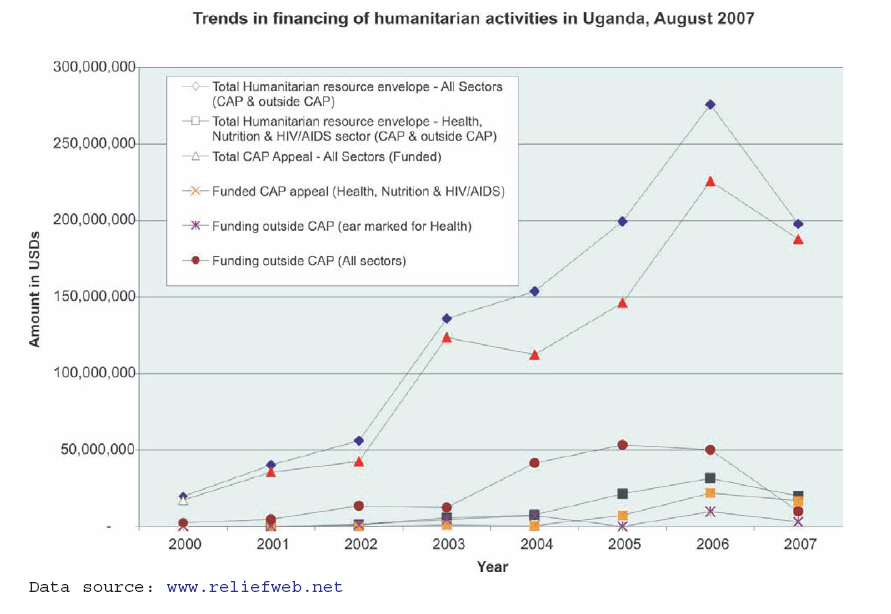
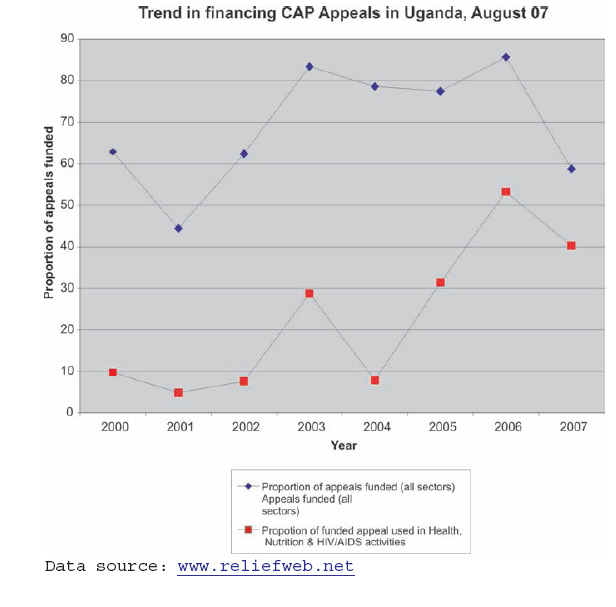
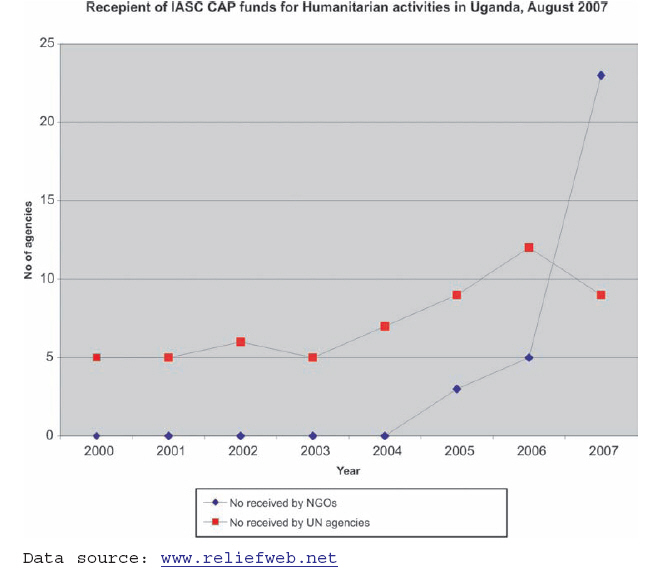
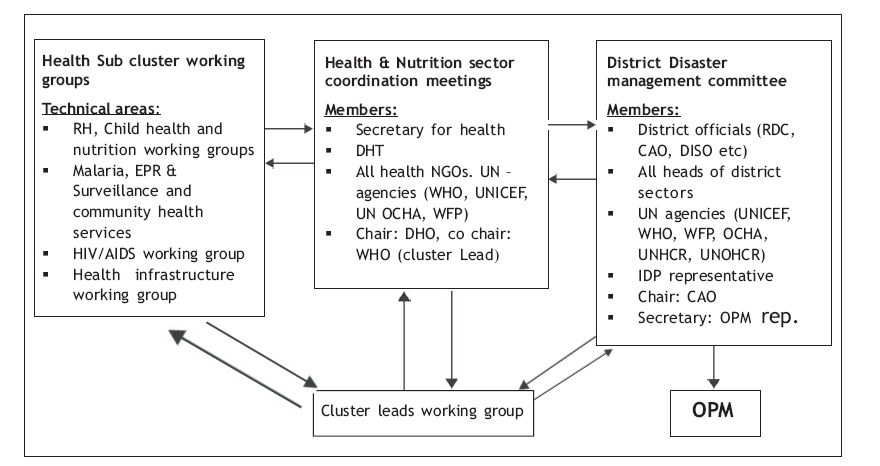
Health Policy and Development Journal, Vol. 6, No. 1, April, 2008, pp. 73-82 Miscellaneous Articles Coordinating Health Care During Humanitarian Emergency: Experience From Pader District, Northern Uganda Innocent Komakech, National Professional Officer Health Action in Crisis, WHO Pader Field Office, Uganda. Contacts: e-mail: innocentkomakech@yahoo.com Code Number: hp08009 Abstract Coordination of humanitarian assistance has been a subject of concern for several decades. The humanitarian reforms initiated by United Nations following UN General Assembly resolution 46/182 and the subsequent reforms that introduced the Cluster Approach to humanitarian assistance offers some opportunities for improved coordination. The main challenges to these reforms remain their acceptance among the humanitarian community, mainly NGOs, and donor faith in providing funding through the structures. We conclude that offering a comprehensive package to coordination encompassing joint humanitarian planning, policy, financing and monitoring of interventions is a step towards holistically addressing the needs of the crisis-affected people. There is also need for the UN to intensify dissemination of the humanitarian reforms to key stakeholders to improve their acceptance in the field. Introduction: The global pressure on the humanitarian community to `do no harm' to the world's crisis-affected people has led to major reforms of the way in which humanitarian assistance is delivered. There is a general perception that humanitarian assistance does not adequately address the needs of the affected people and that wide disparities exist in the quantity and quality of the aid received by the intended beneficiaries. Poor coordination of assistance and inequitable distribution of assistance has been blamed for the inadequacies in humanitarian response. Henry Dunant witnessed and documented the horror of poor humanitarian response following the lethal battle of Solferino in Italy. In 2 questions, Dunant advocated formation of relief societies for provision of care to the wounded in wartime and an international principle for protection of the relief society personnel providing such care. The main outcomes were the Red Cross movement and the Geneva Convention ratified by 16 states mainly Western European countries in August 1864 to protect volunteer humanitarian workers and to enable access to the wounded at war. No attempts were instituted to prevent war but only to mitigate its effect. Complexities caused by World War II reversed the casualty pattern during wars; this time 90% of the war victims were the civilians, overtaking the active combatants. It soon became apparent in the humanitarian arena that a single agency alone would not be able to provide all the available services/assistance. It also meant that assistance to the victims of wars would surpass medical services in a sick bay or ambulance services for casualties given the required skill mix and a large number of personnel to provide those services and assistance. This mixed situation continued and resulted in nearly every war ending up with a couple of humanitarian organisations each with its own mandate, principles, line of allegiance and identity for their personnel. Over time, influx of humanitarian agencies meant that the scale and scope of services provided during humanitarian emergencies became more holistic and the fatigue on one agency having to cover a large population alone reduced. Advocacy and resource mobilization activities increased financial assistance for humanitarian intervention. Large numbers of agencies providing humanitarian assistance necessitated coordination since most agencies offered similar assistance; food, health care, water and sanitation and protection. This paper seeks to elucidate that effective coordination is critical to addressing the needs of the crisis-affected people. Institutionalisation of humanitarian coordination: The UN, in its charter of 10th December 1948, adopted the Universal Declaration of Human Rights affirming the principle that human beings (including those in crisis) shall enjoy fundamental rights and freedoms without discrimination. In 1951 the Refugee charter provided a framework for dealing with the refugee situation with omission of the internal displacement situations during crisis. The UN Guiding Principles, a soft law on IDPs, provided some form of legal instrument but vested the sole mandate for humanitarian assistance, including coordination, into the national authorities (UN, 1998). Why two different legal instruments for people with similar needs and experiences during crisis (IDPs & Refugees)? The 20th session of the General Assembly of the United Nations Organisation in 1965 while referring to the resolution of the United Nations Economic and Social Council resolution 1049 of 15 August 1964 empowered the Secretary General to assist international NGOs in pursuing the question of coordination during emergencies (UN resolution - 2034 (XX) of 7 December 1965). Other decisions were contained in UN General Assembly resolution 2816 (XXVI) of 14 December 1971 on Assistance in cases of natural disaster and other disaster situations. This resolution called on the Secretary General to appoint a Disaster Relief Coordinator (DRC) to foster cooperation with all organisations for effective humanitarian assistance; manage the relief activities of the UN system in response to disaster-stricken states; coordinate UN assistance with assistance given by intergovernmental and NGOs and ICRC. The Secretary General was also to assist crisis-affected governments to assess their relief needs and priorities, inform donors, and to serve as a clearing house for assistance of external aid; assist governments in pre-disaster planning in consultation with other stakeholders and in information management to aid planning and coordinating disaster relief, including keeping set stockpiles of supplies in disaster-prone areas. The governments were called upon to establish disaster contingency plans, appoint a disaster coordinator; stockpile emergency supplies and ensure training of personnel on their application and to formulate related legal framework. Donor governments were requested to respond promptly to calls by the Secretary General or, on his behalf, the Disaster Relief Coordinator, continue offering emergency assistance in disaster situations and to inform the Disaster Relief Coordinator in advance about the facilities and services they might be in position to provide immediately. The UN system and all other organisations involved with relief operations too should liaise with the Disaster Relief Coordinator. UN resolution 46/182 recognised earlier decisions of the General Assembly, particularly resolution 2816 (XXVI) of 14 December 1971 and 45/100 of 14 December 1990. It prescribed the guiding principles for humanitarian assistance; principles of humanity, neutrality and impartiality and that humanitarian assistance should be provided with considerations for sovereignty, territorial integrity and in accordance with the Charter of the United Nations. The requirement that the national unity of states be respected and consent of the affected country be sought was also provided for in the resolution. The central and unique role of the UN in providing leadership and coordinating the efforts of the international community to support the affected countries. In an effort to strengthen leadership and coordination role of the UN, the resolution in the annex paragraph 33 recommended the Inter-Agency Steering Committee (IASC), consolidated appeals, a central emergency revolving fund (CERF) and a register of stand-by capacities. It was resolved that the inter agency steering committee chaired by the Emergency Relief Coordinator, merges the role of this position with that of the United Nations Disaster Relief Coordinator (Resolution 46/182, Annex 34, 1991). This structure placed humanitarian assistance high on the international policy arena; the plea of the world's crisis-affected people could now receive attention. The presence of the IASC also meant that the quality of the policy proposal forwarded to the general assembly and the executive board is improved given the different experiences and personalities that form the committee. Though dependent on donor good will and interests, the Consolidated Appeals Process and the CERF funds were seen as more reliable opportunities for raising funds for emergencies. The Consolidated Appeals Process: the humanitarian planning and financing Framework This humanitarian planning and financing framework resulted from the experience of uncoordinated and poor response to the Kurdish refugee crisis in the aftermath of the 1991 Gulf War. The crisis, characterized by massive influx of refugees (an estimated 1 million people), uncoordinated response and chaos (UNOCHA 2006) and political manoeuvres on refugee asylum by Turkey exposed the lack of capacity by the UN system, NGOs and International organizations to assemble and effectively coordinate major humanitarian response during crisis. The Consolidated Appeals Process (CAP) was thought of as a way forward. It mandated the Secretary General to work with all concerned organizations and states in preparation of Consolidated Appeals for all emergencies requiring a coordinated response. The CAP is a program cycle, quite synonymous with the conventional planning cycles used in routine programming. The CAP involves a cycle of activities for the aid organizations to analyze the context, assess needs, build scenarios, plan, coordinate, fund, implement, and monitor their response to disasters and emergencies, in consultation with governments. It is developed on the basis of the strategic plan (Common Humanitarian Action Plan, CHAP) that is formulated under the leadership of the Humanitarian Coordinator and the IASC country team; other key players, government of the affected country and donors, are consulted during the process. The CHAP describes the humanitarian context, needs of the affected people, scenarios, stakeholder analysis, objectives, priority response plans and monitoring strategies. Consolidated Appeals present a snapshot of situations, response plans, resource requirements, and monitoring arrangements. All Consolidated and Flash Appeals are derived from the CHAP. By design, Flash Appeals are for emergencies lasting between 3-6 months and Consolidated Appeals are for crises of more than 3 weeks. Flash Appeals should be issued between 2 to 4 weeks; they are originated by the Humanitarian Coordinator in consultation with the IASC country team, ERC and IASC Headquarters team. The endorsement of the host government is required (IASC, 2003). The abrupt nature of the disasters means that the resources for Flash Appeals may not be readily available; however agencies with no available hard cash could access funds through the Central Emergency Response Funds (CERF), thus, the possibility for quick response and improved humanitarian response (IASC, 2003). The CAP has been instrumental in facilitating a strategic approach to humanitarian action, fostered close cooperation between host governments, donors, aid agencies, and in particular between NGOs, the Red Cross Movement, IOM and UN agencies. Since 1992, about one hundred donor countries have provided US$29 billion for 240 appeals to address the needs of people in more than fifty countries and regions. The CAP reforms spearheaded by UN OCHA resulted in formation at global level of the CAP working group in April 1998 to discuss and address weaknesses in the CAP (IASC, 1998-a). Over the years, there has been increase in the humanitarian resource envelope. As shown below, the CAP has gained a remarkable confidence becoming the main funding mechanism for humanitarian activities. Figure 1 Trends in the financing of humanitarian activities in Uganda, August 2007 Further analysis suggested over 90% of the funding received before 2003, both CAP and outside CAP, targeted Sudanese Refugees in Uganda. For example in 2001 only US $23,474 of the US $160,416 was ear-marked for IDPs (www.reliefweb.net), and the main recipient of funding were the Sudanese Refugees. The question is; how does the Humanitarian Coordinator or those designated decide that a conflict is of a scale that requires a coordinated response for which CAP is required? The criteria "for conflicts requiring a coordinated approach", for which the Humanitarian Coordinator should call for CAP are not clear. The affected governments could exploit this in the pretext that the existing system or government structure can manage and that there is no need for external interventions; while no humanitarian assistance is provided to the affected communities. Figure 2 Trend in financing CAP Appeals in Uganda, August 2007 As shown above, the response of the donors in financing of CAP appeals has been very good. However the health component of the appeals remained largely under-funded until 2004. The WHO/MOH mortality survey in northern Uganda in July 2005, one of the most contested surveys on the topic, shed some light on the possible situation of health outcomes in Northern Uganda and yet could have been responsible for the growing funding for the sector in the region after 2005. The numbers of NGOs receiving CAP funds have also increased tremendously from 2004 surpassing the UN agencies in 2007. This increment could be due to increased confidence of both the donors and the NGOs in CAP. As provided for in the UN resolution 46/182, Consolidated Appeals should be prepared in consultation with the government in the affected state. It is expected that this approach will pave way to flexibility in interpretation of country situations, impartiality of the UN and IASC and to allow for government inputs into the appeal process (IASC, 2003). What happens when affected governments do not perceive a major humanitarian crisis as a problem? Can the Humanitarian Coordinator go on with the Appeals process? When does a country get considered to be weaned off from developing CAP? Is it determined by donor response or by humanitarian and development indicators necessitating termination? The governments cannot appeal directly for funding under this arrangement even though the resources so mobilized are utilized for humanitarian work in partnership with government institutions and teams. At field level two appeal process models are in use. With the exception of the 2008 CAP process, the past processes involved NGOs and UN agencies deciding on their priority interventions, considering their capacity and comparative advantage and then developing CAP sheets at central level. Such sheets are then aggregated into the overall appeal for presentation to the donors. This therefore meant that the CAP sheets were a collection of projects thereby losing the benefits of holistic programming and the opinions from the representatives of the crisis-affected people. The other model involves a brief of the key stakeholders (government representatives, NGOs, UN agencies and other interested persons) on the CAP process. Subsequent processes then involve consultation of the districts, NGOs and UN agencies at district level that identify the priorities for the development of the CAP sheets that is done at central level. It is anticipated that NGOs and UN agencies can then develop projects from the block planning figures of CAP to address the needs of the affected people. In the CAP process the critical steps seem to centre on the development of the CAP sheets and the projects; the former being a political process. It is in these two steps that the needs of the crisis-affected people may be at stake. Ideally, upon obtaining commitment or actual funding a planning meeting should be organized for all stakeholders at appropriate levels to fine-tune assistance to the local needs at that particular point in time. This should be the basis for project development from CAP funds and not the ad hoc consultative or project development. Figure 3 Recipient of IASC CAO funds for Humanitarian activities in Uganda, August 2007 At field level CAP is a popular framework as evidenced by participation of agencies (UN & NGOs) in its development. Nonetheless, some NGOs still do not subscribe to the CAP process. There is a feeling that there is no need to bother with the CAP process if an NGO gets its funding directly from a specific donor. Some NGOs feel that the CAP is an initiative from the UN to control NGOs while others view CAP as a rigid framework which impedes speedy funding in emergencies. Some agencies even question the neutrality of the UN in administering humanitarian funds given that the UN derives its authority from member states that represent the views of governments including that of the affected people. Even among the UN staff there is still a feeling that the CAP is UN- driven. The Humanitarian Policy arena The establishment of the Inter Agency Steering Committee in June 1992 chaired by the Emergency Relief Coordinator in UN General Assembly resolution 46/182 (IASC, 2005) introduced new dimensions in humanitarian assistance; the interface between humanitarian assistance and politics. The Resolution spelt out the composition of IASC to include "all operational organizations and with a standing invitation to the International Committee of the Red Cross, the International Federation of Red Cross and Red Crescent Societies, and the International Organization for Migration. Relevant non-governmental organizations can be invited to participate on an ad hoc basis." The Committee seeks to develop and agree on system-wide humanitarian policies; allocate responsibilities among agencies in humanitarian programs; develop and agree on a common ethical framework for all humanitarian activities and to advocate for common humanitarian principles to parties outside the IASC. The other objectives include identification of areas where gaps in mandates or lack of operational capacity exist and resolution of disputes or disagreement about and between humanitarian agencies on system-wide humanitarian issues. Critically speaking, resolution 46/182 made a land mark undertaking in streamlining not just coordination of humanitarian assistance but its management as well. It provided a framework for planning, policy and financing of humanitarian assistance within one system which can be seen as very crucial in managing emergencies. The agency has been instrumental in formulation of both micro and macro humanitarian policies which have shaped intervention at global level and it the field. The IASC membership at national level mirrors the global arrangement and it is the sole IASC structure in country; no further structures are present at field level. But how does an issue reach on the IASC agenda to get discussed? Who decides what should be discussed by IASC? How is the implementation of the policies done? What mechanism is there to encourage adherence to the IASC policies and guidelines by all stakeholder agencies? Most humanitarian policies seem to stem from past mistakes in humanitarian emergencies; including the resolution which recommended the IASC itself. The press and advocacy groups have played major roles in setting the humanitarian policy agenda. A wide variation exists between the agendas set by the media, organized groups, NGOs or advocacy groups. The media concentrates on flag-raising in case of poor or non response. The interest groups also protest operational guidelines and policies, sometimes without giving alternative suggestions. The acceptance rates of global humanitarian policies and guidelines are low; and here it does matter how many the agencies protesting are but the number of significant stakeholders (donors) they can influence. Even with trivial reasons, a handful of humanitarian actors have defeated many good intentions in the enhancement of the quality of humanitarian assistance. The Sphere Project standards and the Humanitarian Ombudsman/Accountability Project remain the most contested humanitarian guidelines (UN 2000 in Griekspoor and Sondorp, 2001). The Ombudsman Project initiated in 1997 in response to concerns of deficiencies in accountability for humanitarian outcomes for the crisis-affected people was labeled a policing mechanism for Sphere standards/and or Code of Conduct (UN 2000 in Griekspoor and Sondorp, 2001). The sphere standards, an outcome of the evaluation of the Rwanda crisis, are facing the same fate (Griekspoor and Sondorp, 2001). Despite the wide consultation and NGO consortium-based approach to documenting lessons learnt from refugee emergencies and other acute emergencies for the Sphere Project, the critics view the standards as only applicable in refugee camps and acute emergencies, and that they expose humanitarian assistance to political manipulations; too much technical focus, unrealistic expectations, publicity which affects donations and ignoring the fact those complex situations require innovative responses (Griekspoor and Sondorp, 2001). The critics provide no alternatives; perhaps intuition. Consensus-based approach to conducting business in the humanitarian field provides a major buffer for simple rejection of humanitarian mechanisms and no culprit is accountable as long as there is funding and government approval for their programs. More donor support to the CAP and insistence that all agencies access humanitarian funding through this as a sole financing mechanism could promote more accountability, better tailoring of the humanitarian assistance to the need of the affected people and reduction in parallelisms in the field. The 2005 Humanitarian Response Review; what is new? The uncertainty in humanitarian response prompted the Emergency Relief Coordinator (ERC) in 2005 to launch a Humanitarian Response Review. This resulted from the perception that the humanitarian response varied in different crises and that provision of basic needs to the affected people was not timely (UN, 2005). The review team assessed the response capacity of the UN, NGOs, Red Cross/Red Crescent moment and other international actors including International Organization for Migration (IOM) between February and June 2005. The findings suggested that the humanitarian response is not good enough accountability to the beneficiaries; joint planning (each agency pursued individual initiatives) and major gaps existed in preparedness of the humanitarian organizations - human resources (management and over-reliance of emergency teams) and sectoral capacities for provision of basic social services. The IASC, the most representative coordination body was also found not representative of all the humanitarian actors. Resulting from the recommendations of the Humanitarian Review team, 4 pillars of humanitarian coordination were developed by the IASC in 2005; the humanitarian coordinator system, predictable funding for emergencies, the Cluster Approach and partnership between UN and non _UN humanitarian actors. For the first time, a Central Emergency Response Fund (CERF) was established with a loan of up to $50 million dollars especially for emergencies with committed funding or likely to get committed funding but where not fund is yet available. Under-funded crisis could also benefit from a grant of up to $450 million for rapid response. The Cluster Approach was an attempt to improve on predictability, timeliness and effectiveness of humanitarian response. It was also thought that the approach would strengthen leadership and accountability for the humanitarian response. The cluster leads are accountable for ensuring appropriate level and standards of response to the Humanitarian Coordinator who reports to the Emergency Relief Coordinator. But, when does the cluster lead account? And should the cluster leads alone be accountable for the entire poor response? What if lack of funding impeded humanitarian response, who should, then, be held accountable? Documented evidence of success of the Cluster Approach includes the response to the Pakistan and Lebanon emergencies. It was concluded that clarity in cluster leadership averted large scale loss of life as opposed to the uncoordinated approach during the early phase of Darfur crisis (IASC, Nov 2006). This approach is being piloted in Uganda, Liberia, Somalia and Democratic Republic of Congo for chronic emergencies and Pakistan, Lebanon, Mozambique and Philippines for areas with acute emergencies. It requires that for each thematic area, a cluster lead be designated. In new emergencies a Humanitarian Coordinator (HC) or resident coordinator consults the national authorities and relevant IASC partners at country level, forwards a list of agencies to the Emergency Relief Coordination (ERC) for endorsement within 24 hours. The ERC, in consultation with the IASC at global level and the HC to clarify any discrepancies, approves the cluster leads within 24 hours. In on-going emergencies, the Humanitarian country team, government, national NGOs and other stakeholders reach a consensus on the proposed list of cluster leads for the HC to forward to ERC who follows a similar process as before. However, the approval is expected within 1 week. The cluster leads are expected to identify key partners, coordinate humanitarian program implementation, plan and strategize development and application of standards. The roles include monitoring and reporting, advocacy, capacity building and acting as a provider of the last resort. Providers of last resort provide all interventions or funding which the agencies in the field and government are unable to provide. Should this be funded through funds already with the agencies in the field or a Flash appeal or CERF funds? When should such a situation be considered prevailing? Cluster monitoring assessment conducted in 2006 (about 8 months after its introduction) in Uganda noted achievements in cluster work plan development, mapping, inclusive coordination, training and better coordination of participants but raised concerns of negligence of HIV/AIDS interventions, weak coordination at district level and poor reporting, among others (IASC, 2006). World Health Organization was designated to be the cluster lead for Health Nutrition and HIV/AIDS in Uganda taking over from the pioneer lead - UNICEF in November 2006. The Cluster Approach was introduced in northern Uganda in April 2006 replacing the Joint MOH/UNICEF sector coordination arrangement which mainly comprised of meetings. The initiative began with development and dissemination of tools (cluster strategic documents, Work plan - 2006, and the Modus Operandi), mapping of the cluster members according to their capacity and comparative advantage in humanitarian assistance and orientation of the NGOs and UN agencies on the Cluster Approach by UNOCHA. The opening of a UNOCHA office in Gulu in June 2001, pressured by lack of humanitarian information for planning, paved way for closer collaboration with the Disaster Committees in the districts. The committees receive technical assistance to effectively analyze the needs of the population, design strategies to cope with the needs and deliver the necessary live saving assistance to the population in the camps (UN, 2004). But it was not until 2003 that additional OCHA national offices were opened in Kitgum, Moroto, Soroti and Pader District. The main national achievement of the cluster so far includes improved partnership among humanitarian agencies, coordination of humanitarian activities and better understanding of the needs of the affected people from joint assessments, monitoring and supervision, service availability mapping and implementation matrix of who is doing what and where. Information sharing among the humanitarian agencies has improved; the cluster mailing lists, Google groups and emergency reference libraries are examples. Misunderstanding of the concept of Cluster Approach, disparities in agency mandates and weaknesses within the district structures have been a major obstacle to the cluster roll-outs. Some NGOs and International organizations also initially perceived the Cluster Approach as a UN-driven arrangement and that it is only introducing another layer of bureaucratic barrier to humanitarian funding. Inside the Pader Health Cluster The implementation of health sector coordination arrangements, mainly monthly meeting in Pader District, began in 2005 led by UNICEF and the then District Director of Health Services (DDHS, now District Health Officer, DHO). At that time, a sector was defined as the `technical programs or specific areas of humanitarian activity', while clusters were the agencies who implement those technical programs grouped together. The implementation of the Cluster Approach in Pader District was initiated by the then lead, UNICEF, in February 2006. The cluster activities faced major challenges at this time given the delicate humanitarian situation and the fact that the agencies were few and scattered. The humanitarian response to the district's 337,513 people scattered in 18 sub counties was conducted in a situation then described as the epi-centre of the Northern Uganda conflict where greater than 90 % of the rural villages where displaced into camps at the height of hostilities. The majority of cluster members, including the cluster lead, commuted from Kitgum, which weakened the coordination efforts. Active cluster activities began to take root in mid 2006 as UNICEF beefed up its staffing and with the presence of a WHO field office in Pader. Analysis of the cluster structure before October 2006 concluded that the Health and Nutrition cluster meeting was the sole coordination arena. There were many questions on the functionality of the Health, Nutrition and HIV/AIDS cluster then. How do issues reach the agenda of the health and Nutrition meeting? Who decides what issues should be discussed? Who ensures that the decisions are implemented? Should the cluster lead shoulder the entire blame resulting from the team's non-response or poor response? How can all the technical areas under the jurisdiction of the Health, Nutrition and HIV/AIDS cluster receive equitable attention? There was the observation that generalising the Health and Nutrition meeting with one single agenda was to blame for the poor attention given to some technical areas. Nutrition and HIV/AIDS were some of the technical areas that rarely got on the agenda. The thinking that as a team, the health cluster members should fail together and that all technical areas should receive equitable attention after January 2007 resulted in a cluster coordination structure below initiated by WHO and agreed on by the cluster members during the Health and Nutrition meeting. It was also agreed in the Health and Nutrition cluster meeting that each working group could have up to 7 members; health NGOs were encouraged to participate in at least 1 working group. The membership depended on interest and technical experience of the agencies. The agencies in the working group organised and discussed the issues related to the working group and solve some manageable problems. The working groups received reports from all the humanitarian agencies, discussed them and summarised them for the consumption of the Health and Nutrition meeting. The work groups also identified gaps, recommendations and achievements from the working group meetings for presentation to Health, Nutrition and HIV/AIDS cluster meeting and where decisions were made by consensus. The summary of discussions and decisions in the Health, Nutrition and HIV/AIDS cluster meeting were forwarded to the District Disaster Management Committee meeting for discussion and decisions. This management structure increased participation of all stakeholders in health and nutrition cluster coordination, ensured that all technical programs in the cluster receive ultimate attention and improved the overall management of the cluster through a team approach. Because the working groups were chaired by a member of the District Health Team (DHT) closely supported by the UN agencies, the participation of the district improved and attendance from the humanitarian agencies became significant. The DHT members who were expected to chair the working groups received training by the WHO technical officers on facilitation skills during meetings and agenda formulation. District participation also ensured that the district is actively engaged in humanitarian interventions which would in the long term facilitate smooth hand over once the emergency was over. The introduction of the working group approach in Pader began with a protest in the Health, Nutrition and HIV/AIDS working meeting in Kampala; the point of contention being `many meetings'. Later a consensus was reached that the cluster at central level would not interfere with agreed cluster management arrangements at district level. To facilitate in operationalising the working group concept, the cluster lead (WHO) drafted generic terms of reference which were discussed and agreed upon among the cluster members. According to the generic terms of reference, working groups were expected to ensure that all the technical areas are comprehensively covered and that service gaps are tabled in the health and nutrition coordination meeting for opinion and decision. The groups also identified and mobilized members while respecting their mandates and program priorities, received and discussed reports from members on the status of implementation of their activities in the technical program area to aggregate the outputs the health, nutrition and HIV/AIDS cluster meeting. The other roles were to harmonize areas of operation of the members to prevent duplication and where possible explore the options on relocation to fill gaps and to ensure linkage between working group members and the district structures at all levels of service provision. Working group members were also expected to prepare for and participate in joint interagency program monitoring activities in collaboration with the district and other advocacy activities for the technical program. The introduction of working groups meant that activity reports from humanitarian agencies are discussed in depth in the working groups and were therefore not individually presented in the plenary of the cluster meeting. This kept the discussions more focused, shortened the length of the meetings and increased the members' willingness to participate. On the whole, the district health team thought that the working groups provided an excellent opportunity to negotiate resource investment into other constrained technical programs. Others found it difficult to lead the working groups since it required more close interaction with the NGOs, demanded for accountability for activities to and from the NGOs and required more time for the officer to be present and to technically support their individual programs. Some NGOs were at the beginning more stereotyped; the notion that it is the UN pushing its influence was expressed but 4 to 6 months later the working groups was approved as reasonable structure by most agencies, especially those with strong leadership such as the HIV/AIDS working group and the Malaria and Community Based Services group. There were difficulties in the Infrastructure, Child Health, Reproductive Health and the Nutrition working groups. The common characteristics of the poorly performing working groups were weak leadership from the district health team, weak capacity of the NGO partners, lack of prioritization of the working group activities (feedback meetings and Joint Interagency Monitoring), low morale to participate in a coordination system, inadequate presence at implementation level (creating fear of exposure) and inadequate charisma from the technical officers (co chairs) supporting the DHT. The working groups organised and conducted joint interagency monitoring visits. The visits allowed the sharing of field experiences (lessons learnt and program outputs) among agencies, identification of strengths and gaps in the implementation of programs in the Health and Nutrition cluster and contributed to incremental improvement in Health, Nutrition and HIV/AIDS interventions through routine regular feedback on agency activity implementation. Reports from the visits are discussed in the working group meetings and further presented to the Health and Nutrition cluster meetings. The monitoring reports are then developed into action plans, discussed in the responsible working groups and documented. For interventions requiring resource inputs beyond the available resources of the NGO partners/local government, the resource gap is floated by the cluster leads. All options are explored including internal sources within the cluster members in the district, outside the district or with the cluster lead's buffer resources. The status of implementation of the action plan is discussed regularly in the working group meetings and the health and nutrition cluster meetings. In the past interagency action plans also formed a basis for future interagency monitoring visits in addition to other interventions decided by consensus in the working groups. Joint interagency monitoring added value to the overall humanitarian response; it provided an environment for sharing technical information and the regular visits provided a momentum for continuous program improvement (both in quality and scope). It was also a deterrent to agencies intending to provide lip service to the community given the transparent nature of the visits. Other obstacles to coordination In the past, coordination of humanitarian intervention was done through meetings alone. This created disparities in accountability. Meetings were long and some agencies stopped attending. There has been misunderstanding of humanitarian principles and complementarity of interventions. Too much attention to individual agency priorities and visibility compromises coordination of effective response to the crisis-affected people. Conclusions and recommendations Several attempts have been made to coordinate humanitarian assistance to the world's crisis-affected people resulting from past mistakes in humanitarian response. Offering a comprehensive package to coordination; joint humanitarian planning, policy, financing and monitoring of interventions, is a step towards holistically addressing the needs of the crisis-affected people. The recent reforms introduced by the United Nations offer new challenges and hope for a sustainable coordination mechanism. There is need to embrace a more holistic approach to coordination of humanitarian interventions. Effective coordination should encompass joint humanitarian planning, policy, financing and effective monitoring of assistance for the humanitarian actors to save lives. Such a mechanism would provide for flexibility and tailoring of response in the ever changing situations of crisis. For coordination to work, humanitarian agencies should make deliberate and voluntary efforts to participate in a coordination mechanism; intrinsic more than extrinsic. There is need for UN humanitarian agencies to disseminate the coordination reform to improve its acceptance in the field. References:
OPM Data source: www.reliefweb.net Copyright 2008 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp08009f4.jpg] [hp08009f1.jpg] [hp08009f3.jpg] [hp08009f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}