 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 6, No. 3, December, 2008, pp. 102-116 THEME ONE: HIV/AIDS, REPRODUCTIVE HEALTH AND RIGHTS Lifetime experience and management of cases of gender-based violence in the health facilities of Kabarole District, Uganda Margaret Tumwebaze*, Everd Maniple# and Shannon McMorrow# *Corresponding author: Senior Nurse Tutor, Virika School of Comprehensive Nursing, Fort Portal, Uganda, P. O. Box 233, Fort Portal
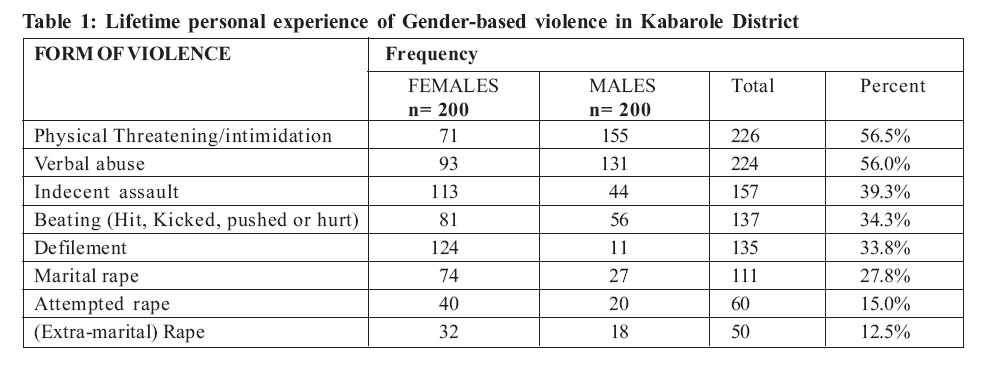
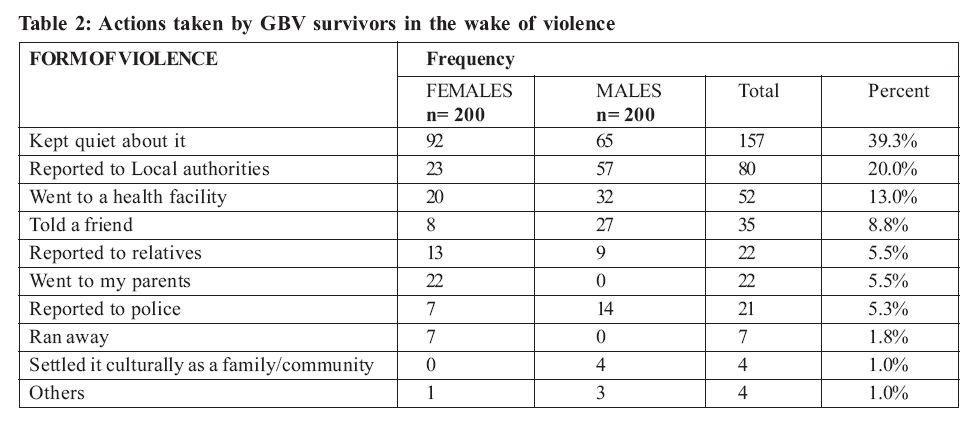
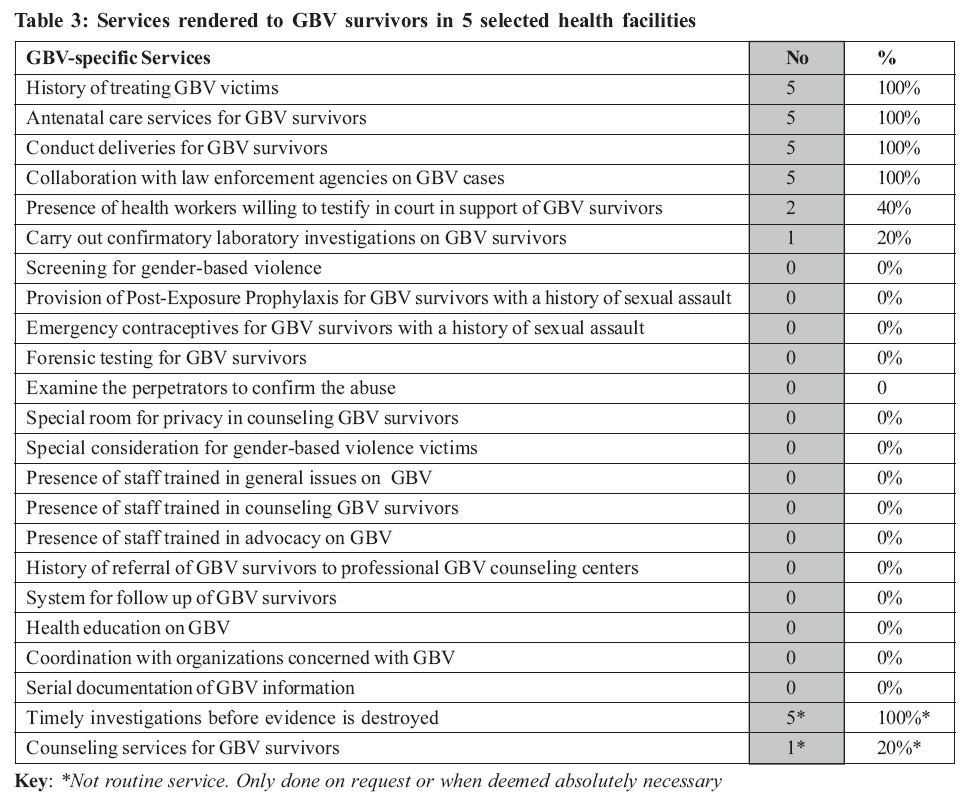
Uganda, e-mail: mtumwebaze@yahoo.co.uk Code Number: hp08014 Abstract Gender-based violence (GBV) is a common problem in many countries, leading to high levels of mortality and morbidity, especially of women. In the health sector, GBV presents in a cryptic manner due to fear by the victims, poor records, culture, inadequate staffing and inadequate equipment. In developing countries, there is also a lack of policies, standards and guidelines for case management. As a result, GBV cases are never recognized and are poorly managed. This study set out to assess the management of GBV victims in health facilities of Kabarole District, western Uganda. It aimed at profiling the common forms of GBV, the lifetime experience of GBV by ordinary residents, the accessibility of health services to GBV victims, the health services rendered to them and to analyse inter-sectoral collaboration on GBV issues. A descriptive cross-sectional study involving 400 respondents, 40 key informants and 2 FGDs was done in May and June 2006. Over 96% of the respondents had ever experienced a form of GBV and women were more likely to have experienced it than men. Most were likely to have experienced physical violence. Female respondents were more likely to have abused their victims verbally while the males were more likely to have abused them physically. Most cases of GBV were domestic and were never reported to any authorities or to the health system unless they had led to severe physical injury. This was due to cultural restrictions on discussing domestic matters publicly. GBV survivors also often lacked funds for transport and processing the cases either with the health services, local authorities or police. They reported long waiting times at health facilities, absence of staff, lack of privacy and lack of medicines as the common problems they faced at health facilities. The range of health care services provided to GBV survivors was very narrow and mostly on request by the police. Apart from being insufficient and absent, health workers were not trained in screening for GBV, management of cases and conducting forensic investigations. They did not probe actively for possible history or evidence of GBV and the data were never disaggregated within the HMIS. Intersectoral collaboration on GBV was limited to preparing police dossiers and court testimony. The paper recommends the formulation of a national policy on GBV, and the setting up of standards and guidelines for case management in the health sector. It also recommends adequate equipment of district level facilities for sufficient forensic investigations as well as training of health workers in case management including counseling. It recommends institutionalization of GBV data collection through revision of the HMIS and Continuing Medical Education. Finally, it recommends wider inter-sectoral collaboration in order to enhance prevention of GBV at community level Introduction Gender-based violence (GBV) arises from discrimination and oppression particularly against women and children but is also experienced by some men. It includes physical and psychological injury due to domestic violence, assault, rape and defilement, conflict situations as well as cultural practices including female genital mutilation (FGM) (Vann, 2004). GBV is both a violation of human rights and a public health problem. It can have serious implications for a woman's sexual and reproductive health. It is associated with increased risk of gynecological disorders, unsafe abortion, pregnancy complications, miscarriage, low birth weight and pelvic inflammatory disease (Vann, 2004). The victims of GBV may be children, especially unaccompanied minors (UAMs), women, mentally and physically disabled persons and economically disempowered people. They may also include junior staff males and females, students and less privileged community members (Directorate of Gender, Uganda, 1998; Vann, 2004). The potential perpetrators include intimate partners (e.g. spouses or friends), influential community members (teachers, leaders, and politicians), strangers, members of the community, relatives and anyone in a position of power (Directorate of Gender, Uganda, 1998; Vann, 2004). Since the survivors of GBV often end up with problems that need medical attention, the health facilities should be able to provide the necessary services. In Uganda, the health sector has not been doing much on GBV. The first time GBV appeared in health policy documents was in the second Health Sector Strategic Plan (HSSP II), where it was hoped to develop and disseminate an integrated strategy to address GBV. The core interventions in the plan are to compile and analyze information available, in order to establish the prevalence of GBV in Uganda; to formulate strategic interventions for the health sector including initiating a campaign to raise awareness about GBV amongst health care workers; to support agencies and organizations that work to address GBV; and to enhance partnership with other sectors on matters of GBV (MOH, 2006). However, to date, not much has been done on the matter. Study area The study was undertaken in Kabarole District in western Uganda, which has had one of the best performing district health systems in national the district rating for some time. It had a population of 384,822 with three large hospitals in a municipality of about 40,605 people in 2002 (UBOS, 2002) in proximity to the famous Mountains of the Moon. Other health facilities are also unequally distributed and only 60% of its population lives within 5 km of any health facility (DDHS Kabarole, 2006). Problem statement Worldwide, health care and social services generally do not recognize symptoms of gender-based violence and do not provide adequate treatment, protection and support to the GBV victims. The many gender-related studies undertaken in Uganda have mainly focused on aspects of GBV and the law. Within the health system, the range of services provided and the level of access to those services that the survivors of GBV receive is not very well known. Even then, the few studies have reported problems in the management of GBV victims in general. Some of the problems reported include lack of health workers trained on gender issues, thus leading to failure to screen for and recognize GBV during history-taking; insufficient facilities like laboratory equipment and counseling rooms for privacy, proper investigation and management of GBV victims; and lack of collaboration with other sectors. The national health management information system (HMIS) is not yet re-designed to capture GBV issues on a routine basis and many GBV cases are simply recorded as injuries without gender-specific analysis. Health workers do not regularly screen patients for history of gender-related abuse in order to investigate the reports promptly before evidence is destroyed and they do not counsel the victims of GBV. It was also not known if the facilities provide sufficient privacy to enable proper investigation of reports. In addition, the readiness of the health workers to testify on such cases in court in defence of the victims, availability of health workers specifically trained on GBV issues, the level of collaboration between the health sector and others on GBV and the problems faced by the GBV victims as they seek medical care were all not known. It was expected that if information about all these aspects is obtained and used b y the relevant authorities, the management of GBV cases in the district would improve. Study objectives The objectives of the study were to identify the common forms of GBV in Kabarole District; to determine the lifetime experience of gender-based violence among men and women in Kabarole district; to find out the accessibility of health services by GBV victims; to establish the range of services rendered to GBV victims and to analyze the level of collaboration on GBV between the health sector and other sectors within the district. The study focused only on determining the range of services offered to GBV survivors without concentrating on their quality. In addition, it did not cover the legal consequences of the GBV cases but looked at whether the medical personnel knew and followed what the law requires when dealing with the survivors of GBV. Literature Review This section describes the common types of GBV, the common victims of GBV, the prevalence of violence in different settings by sex and age and the effects of GBV. It also explains the actions commonly taken by the survivors, the difficulties met in trying to access health services after GBV, the range of services commonly rendered to GBV survivors and collaboration between the health sector and other sectors. Common forms of GBV Gender-based violence can take many forms. It may be physical, sexual, economic, emotional, social and/or psychological abuse. It can also be through neglect, and financial and material exploitation. Most GBV is domestic, between family members. In addition to being at increased risk for physical harm, victims of all forms of domestic violence are at risk for other complications which eventually lead to the need for medical care and other services (New York State Health Department, 2002). The forms of GBV that are most commonly heard of are sexual forms and battery. Sexual violence includes harassment (usually verbal, visual, body language or by stalking), indecent assault (physical unwanted and uninvited sexual contact), rape (including marital rape) and attempted rape, sodomy (unnatural sexual acts), child sexual abuse, forced prostitution, child prostitution, and harmful traditional practices (Directorate of Gender, Uganda, 1998; Vann, 2004; Garcia-Moreno et al., 2005). It includes any actual or threatened unwanted or coercive sexual contact and/or penetration. Sexual abuse also includes sexual contact with a minor child or vulnerable adult, usually by someone responsible for their care. In the case of minors, sexual abuse may be by someone in a position of authority or in a significant relationship with them (Minnesota Center Against Violence and Abuse, 2004). Physical violence includes spouse beating / domestic violence, assault and harmful traditional practices (Directorate of Gender, 1998; Vann, 2004; and Garcia-Moreno et al., 2005). It is the intentional actual or threatened infliction of physical harm ranging from slapping and hitting to using a gun (Minnesota Center against Violence and Abuse, 2004). Emotional/mental/psycho-social violence includes verbal, emotional abuse, humiliation, intimidation, discrimination, denial of opportunities and services, spouse confinement and harmful traditional practices (Directorate of Gender, Uganda 1998; Vann, 2004; and Garcia-Moreno et al., 2005) Gender-based violence is very common. In a World Health Organization (WHO) multi-country study, more than 5% of women reported physical abuse during at least one of the pregnancies. Twenty five to 50% of these women were punched or kicked in the abdomen and over 90% were abused by the biological father of the child the woman was carrying (Garcia-Moreno et al., 2005). The victims of GBV Although the vast majority of reported victims of domestic violence are female, providers should seek to identify and screen all potential victims regardless of their gender or age. Health care providers do not generally recognize men as being subject to domestic violence, even when confronted by evidence of physical or sexual assault. Despite the fact that it is recommended, studies show that assessment for domestic violence is still not a routine medical practice. Many health care programmes do not have systematic strategies to address GBV. Most providers in the programmes do not probe for information from clients on violence (Hardee, 2005). In Costa Rica, a study of 80 battered women who sought judicial intervention against their partners indicated that 49% were beaten while pregnant and for 7.5% it resulted into miscarriage (US National Association of Social Workers, 2001). In Peru and Guatemala, it was found that women who live with violent alcoholic husbands were victims of marital rape on repeated occasions (Heise et al., 1994 in ISIS). In Nacaragua, a relationship was observed between economic dependence and physical violence. For example, 41% of non-wage earning women were victims of serious physical violence (Latin America and Carribean Women's Health Network, 1996; and Salas, 1994 in ISIS) yet only 10% of the wage-earning women were victims (ISIS, 2005). Similar results were found in the South African province of KwaZulu-Natal (Karim and Frohlich, 2000). In Kenya, domestic violence was responsible for most of the violence against women and girls. In Uganda, women's economic dependence and cultural perceptions of women's sexual and reproductive obligations in marriage have put them at risk of violence. In a study by Human Rights Watch (HRW), 68% of women said that their husbands forced them to have sex (HRW, 2003). Although there were occasional reports of male victims of domestic violence, the balance was tilted heavily against females (Mwau, 2000). In Samoa, a survey conducted to determine the extent of violence against men found out that 2% of men experienced physical violence, 3% had had sexual violence and 45% had experienced emotional abuse. In a WHO multi-country study, 1-9% of the abused women accepted to have ever initiated violence against a partner. Demographic and Health Surveys (DHS) show that 4% of women in Cambodia, 13% in Dominican Republic and 5% in Haiti had ever been violent towards a spouse (Garcia-Moreno et al., 2005). Tibatemwa (1999) interviewed women offenders who were in prison in Uganda. Most of them had killed people and they justified their actions on grounds of self-defence. This was common among women who killed men, especially their husbands (Tibatemwa, 1999). Most violence occurred within polygamous unions and most of the other prosecuted women's victims were co-wives, stepchildren, step-siblings and step-mothers. Some studies point out that while men are the biggest perpetrators of domestic violence, they are also victims. However, because they assume positions of authority in society, battered males often fear to come forward due to shame and often refuse to press charges against their female abusers (Canadian Nurses Association, 1992; AHURIO, 2003). A study which was carried out in Uganda found that there was an increase of sexual abuse of young boys by older women (Uganda Law Reform Commission, 2000). The prevalence of gender-based violence Between 20-60% of women in the Americas live in situations of gender-based violence. In Colombia, 41% of the women reported physical abuse in a current relationship (Cambodia DHS, 2000, in International Planned Parenthood Federation WHR). A study in Bangladesh, Brazil, Peru, Thailand and Tanzania revealed that violence by a male intimate partner existed in each one of these countries. Physical violence ranged from 13% to 61% of the relationships, sexual violence ranged from 6% to 50%, while emotional violence ranged from 20% to 75% of the relationships. The physical violence due to non-intimate partners ranged from below 10% to 62% of the respondents in all the countries mentioned above. Sexual violence by non-intimate partners ranged from below 1% to 12%. Non-intimate partners included fathers, teachers, other male or female family members or male friends of the family. Five to 14% of women reported that their first sexual experience was forced and the younger the woman at first experience of sex, the greater was the likelihood that it was forced (Garcia-Moreno et al., 2005). In Uganda it is still difficult to establish the levels of domestic violence countrywide. In two Ugandan districts, a study revealed that 41% of women reported having been beaten or physically harmed by a partner. About 41% of the men reported beating a partner. Violence against women, though common, is largely underreported or swept beneath the carpet (Directorate of Gender, 1998). Other sources also reported a prevalence of domestic violence (DV) against women of 41% in Uganda (HRW, 2003). However, no literature has been found on the prevalence of gender-based violence in Kabarole district. According to HRW, Nsambya Police Station in Kampala, Uganda, recorded a rise in complaints of DV from 495 in 2001 to 1009 in 2002 (HRW, 2003). In order to increase the likelihood of uncovering cases of GBV, straightforward, open-ended questions asked in a non-threatening and non-judgmental manner help to decrease the stigma associated with abuse. Clients may avoid discussing the matters because the questions are painful, embarrassing or provoke anxiety. The interview should be structured to systematically elicit more data, thus allowing the client to tell his/her own story (Canadian Nurses Association, 1992; New York State Health Department, 2002). Consequences of GBV The consequences of GBV may be health-related, psychological or social. Health-related consequences may be minor or serious and life-threatening. Fatal outcomes include homicide, suicide, maternal mortality, infant mortality, and AIDS-related mortality. Acute physical outcomes include injury, shock, disease and infection. Chronic physical outcomes include disability, somatic complaints, chronic infections, chronic pain, gastrointestinal problems, eating disorders, sleep disorders and alcohol/ drug abuse. Reproductive outcomes include, miscarriage, unwanted pregnancy, unsafe abortion, sexually transmitted infections (STIs) including HIV/AIDS, menstrual disorders, pregnancy complications/ infertility, gynecological disorders and sexual disorders. For children, there is a strong association between witnessing domestic violence and severe post-traumatic stress disorder (PTSD) (Uganda Law Reform Commission, 2000; Gordon and Crehan, 2000; New York State, 2002); and Minnesota Centre against Violence and Abuse, 2004). A study on HIV-positive women in Uganda meant to ascertain the role that violence had played in their vulnerability to infection showed that violence robbed them of any authority over their own sex lives and denied them ability to preserve their own health. Most of the infected women had been forced to have sex without a condom by their husbands and were beaten when they refused sex (HRW, 2003). In most cases, the survivor of GBV experiences mental illness that requires medical intervention like post traumatic stress (PTS), depression, anxiety, fear, anger, shame, insecurity, self-hate, self-blame, constant anticipation of violence and abuse, sleeplessness, peptic ulcers, mental illness, and suicidal thoughts, behavior, or attempts. For example, in several African countries, 40% of women who went to a community mental health service with acute psychiatric presentation had history of abuse (Edwards, 1996; Green, 1999; and Uganda Law Reform Commission, 2000). In the WHO multi-country study cited above, women who had ever experienced physical or sexual violence or both by an intimate partner reported higher levels of emotional distress and were more likely to have thought of suicide and to have attempted suicide than women who had never experienced partner violence (Garcia-Moreno et al, 2005). Studies have confirmed that family violence increases the risk for mental health problems among family members. In a review of the literature among women who have been abused, mental health problems manifested as depression in 48% (in 18 studies), as suicidal tendency in 18% (in 13 studies), as PTSD in 64% (in 11 studies); as alcohol abuse in 19% (in 10 studies); and as 9% drug abuse (4 studies) (Golding, 1999, in Minnesota Centre Against Violence and Abuse, 2004). In a study in the Democratic Republic of Congo, psychological harm was reported as an effect of rape. The victims of rape feared going to the fields and markets, which led to malnutrition and economic loss (Pratt et al., 2004). The most significant social outcome of gender-based violence is stigma and the tendency by society to blame the victim, especially for rape and other sexual abuses. This social rejection results in psychological and emotional damage including shame and inability to function in the community. Due to their fear of social stigma and rejection, most survivors never report the incident and never receive proper health care and emotional support (Directorate of Gender, Uganda, 1998; Vann, 2004). In Kenya, society also tends to penalize the victims of DV more than the culprits and even when the woman is seriously injured, her family tells her to go back home and be a good wife (Mwau, 2000). What GBV victims should do Knowledge on what to do in case of violence can help victims to seek early medical care and also to have evidence confirmed by health workers. Therefore, the population should be aware of services available for GBV victims. For example, the population needs to know why the rape survivors should seek medical care, where to go for services and what services to expect. The population needs to know that survivors should go for medical examination immediately after the incident without bathing or changing clothes (UNHCR, 1999). If one is raped, she should see a doctor about the injuries and to check against sexually transmitted diseases (STDs) and possible pregnancy. Studies have shown that the victims of DV are unlikely to voluntarily disclose their abuse (Gnanadason et al., 2005). Therefore health workers should also be trained to do active search for gender-based violence on a routine basis. Less than one-fifth of sex attacks are ever investigated by police in USA (Knight, 1997). Some women are reluctant or unable to seek help because they are held captive and not allowed out of the house. Others may not have money or means of transport (American Medical Association, 1992; Bloomberg, 2003). Common barriers to reporting sexual assault and DV include cases where health workers know the victim; when service providers are related to the perpetrator or victim; and long distances to access health care - as days pass, victims find themselves torn between preserving forensic evidence and preserving their hygiene (Chamberlain, 2002). However, in many developing countries including Uganda, the investigative capacity is so weak that even preserving evidence may not add value to the investigation. For example, preserving the perpetrator's hair, seminal fluid or blood stains in the absence of DNA testing facilities may not help the case. Many survivors never contact the police or anyone at all (Edwards, 1996). In a WHO multi-country study, 20% to 66% of women had not told anybody about the violence before the interview. Between 55% and 80% of women reported that they had never sought help from health services, police, NGOs, local leaders and religious leaders due to the limited availability of formal services and fear of stigma (Garcia-Moreno et al.,2005). During the interviews with women offenders, Tibatemwa asked them if they had ever sought medical attention. One woman who had killed her husband had several scars as a result of long term violence by him. She had gone to hospital only once in 13 years of marriage because her husband never allowed her to go out of the house after his assaults on her (Tibatemwa, 1999). Accessibility to health services by GBV victims In a study on constraints to accessing reproductive health (RH) services in Kenya, India and Guatemala, issues identified rotated mainly around beliefs and limitations on women's mobility, lack of decision-making power, and gender-based violence (Hardee, 2005). In Uganda, for reported sexual offences, medical evidence is required to prove that someone was raped. The medical examination is carried out either by doctors or clinical officers using official Police Form 3 (PF3). Unfortunately, PF3s are not easily available and victims or their relatives may have to provide the police with funds to obtain a blank photocopy and for handling the case. The process may take as long as four days (Uganda Law Reform Commission, 2000). Such payments, which are illegal, may be made to the police or local authorities and may be an additional significant barrier to access. Even in health facilities, thorough investigations are not done due to lack of the staff legally accepted for the procedure (medical doctors), laboratory equipment and training. The victims are often asked to pay for the medical report and some medical officers are reported to falsify the reports after receiving payment from the perpetrator's side (Uganda Law Reform Commission, 2000). The range of services rendered to GBV victims Whereas the services for GBV victims should be available in most health facilities, if a case has not been identified as such, it is usually difficult for the survivor to receive integrated and comprehensive care. Therefore, most survivors who report to hospital are treated for their injuries only, but not the psychological aspects or disease screening. In Uganda currently, there are no national standard guidelines on the range of services that should be offered to survivors of GBV. This hampers the detection and management of the cases. In general, the package of services for survivors of GBV should cover screening, medical examination, treatment and adequate equipment. The city of New York gives the following as a general guide on the range of services for GBV victims: screening and assessment of the medical context of abuse including taking photos of the injuries; medical and surgical treatment for the presenting injuries; assessing the safety of the victim; counseling the victim regarding available resources and management options; documentation of findings; facilitate women's access to other service delivery programmes through referral; ensuring privacy, even from family members and friends; collection of forensic evidence; provision of testimony to police or court when needed; contribution to efforts that aim at raising community awareness of GBV; coordination and sharing information with concerned Organizations (New York State Health Department, 2002; Bloomberg 2003; Guedes, 2004; Gender-based Violence Global Technical Support Project, 2004; Vann, 2004; ISIS 2004). Screening helps health workers to identify those victims of GBV who are not willing or capable to voluntarily report their condition. In the US, the American Medical Association (AMA) gave guidelines on diagnosis and treatment of GBV. It advised that due to its prevalence and its medical and psychiatric consequences, all women in all departments of the hospital should be screened for GBV (AMA, 1992). It advises that women should routinely be asked direct specific questions about abuse. Such questions may be included in the social history, past medical history, review of systems or history of present illness as appropriate. The client should be interviewed while alone. Clinicians should consider the possibility of assault when the woman's explanation on how an injury occurred does not seem plausible or when there has been a delay in seeking medical care. Because of the risk to the mother and the fetus, assessment for abuse should also be integrated into routine pre-natal and post-natal care. Assessment of DV should also be included as a routine part of psychiatric case management (AMA, 1992). The Canadian Nurses Association recommends incorporation of family violence screening questions into all history-taking forms (Canadian Nurses Association, 1992). Handling sexual abuse cases Examination of the victims and offenders in alleged sexual offences is a task for any doctor, if there is no practitioner with more experience. For female clients assaulted by a male, the examination should preferably be done by a female health worker to avoid apprehension due to recall of the incident in which they were molested (Knight, 1997; UNHCR, 1999). A third party should always be present when a female is to be examined by a male doctor (Knight, 1997). The examination must be performed in good surroundings, for the comfort and reassurance of the victim and to ensure optimum conditions for observations. The room should be well lit, clean, well furnished and equipped with a proper examination couch and instruments. The clothing the survivor was wearing at the time of sexual abuse should be subjected to forensic science examination. The forensic science laboratories should provide a kit to doctors for the collection of trace evidence for scientific examination. The kit should a large sheet of new clean paper, on which the survivor stands while undressing, so that any foreign material falling from clothes is caught and retained for examination. Injuries on other parts of the body are noted. For females, both upper and lower vaginal swabs are taken. Signs of recent injury to the hymen such as bleeding, tearing and edema are noted. If a liquid is seen in the vaginal tract, it should be collected by a pipette into a small tube or picked up on a swab for screening for STDs and DNA. The suspected assailant in a sexual assault should also be examined. All samples taken must be labeled and given to a police officer for transmission to the forensic laboratory (Knight, 1997). In the Western Cape Province of South Africa, the health care facilities were supposed to implement the programme on management of rape survivors. Despite the availability of procedural guidelines for health workers, an evaluation found that only 5 out of 29 (17%) facilities were providing comprehensive health care to survivors of rape. The medical officers felt that they did not have the necessary medical or forensic expertise to provide the best possible care to survivors. Health workers reported that some medical officers resisted the provision of medical and forensic care to rape survivors. Few facilities had set up a designated room/area for rape survivors. In the facilities where such rooms were present, they were poorly equipped (Guedes, 2004). A similar study in Uganda indicated that the doctors examined the genital organs but they rarely took specimen of the vaginal fluid at the time of examination after rape. Most of the victims of rape were examined by male doctors and yet the medical practitioners lacked the knowledge to conduct a thorough and proper examination that could be used to give evidence in court (Uganda Law Reform Commission, 2000). Moreover, comprehensive social history was never taken in hospitals and those with injuries were never asked about possibility of GBV (HRW, 2003). Counseling GBV survivors Normally counseling should take place in a quiet and private environment, where clients feel safe and free to talk about her problems. In South Africa which has the highest rate of rape in the world, statistics from Guateng Province Department of Health revealed that less than 27% of women who take HIV antiretroviral post-exposure prophylaxis (PEP) after a sexual assault completed a full 28-day course of the medication (Centre for the Study of Violence and Reconciliation - CSVR, 2004). Some of the reasons for this were poor counseling and support services provided to the survivor; poor relationship between staff and survivors; limited information for survivors; and stigma attached to sexual assault and HIV. Even where Voluntary Counseling and Testing (VCT) services are provided for HIV case management, the counselors may be dealing with cases where GBV is a feature. They should therefore know whether their client is in a violent relationship and how to counsel and refer such cases. Counseling programmes in Kenya have tried to empower women with information and skills during counseling so that they make informed decision and be prepared to change the situation they were in. This was mainly by helping them identify their potential, making them feel as equal partners with men in development and reproductive health and empowering them to negotiate safer sex practices (Hardee, 2005). Collaboration between the health sector and other sectors on GBV Gender-based violence has many consequences. Since not all of them are of a medical nature, the health sector alone cannot purport to manage GBV cases satisfactorily. The management of GBV cases needs action in the areas of health care, social acceptance and reintegration, security and safety, and legal and judicial support. All these sectors must work in collaboration with one another (Vann, 2004; Gordon and Crehan, 2000). Every time a risk of gender-based violence is detected, providers should ensure that all appropriate support services are involved and that a more comprehensive assessment of risks and needed services is done (Canadian Nurses Association, 1992; New York State health department, 2002). In Uganda, there was no practice of automatic reporting of GBV cases to the police after they were treated (HRW, 2003). However, in the HSSP II, the health sector promises to support agencies and organizations that address GBV, through appropriate partnership (Ministry of Health, 2006). Methodology A descriptive cross-sectional study was carried out in Kabarole District. Qualitative and quantitative data were collected from all three hospitals in the district and the headquarter units of health sub-districts. At each health unit, the respondent was the officers in charge. At the hospitals, the psychiatrists and other mental health care staff were interviewed. Focus group discussions were held with adult men and women in two peri-urban villages. Key informant interviews were held with survivors of GBV, one police surgeon and one police officer responsible for family protection at the district police offices. Reviews of records were held at the health units. The study population was all the people of Kabarole District. Four hundred clients found at the health units on the day of the visit were interviewed. men from the selected parishes, and survivors of gender-based violence who presented at the health units for treatment during the study period. Other respondents were and adult men and women from the two peri-urban villages who participated in the FGDs. The study covered all the health sub-districts and hospitals in Kabarole district, namely Bukuuku, Kibiito and Fortal Portal municipality. All the sub-counties purposively included in the study. Forty mothers were interviewed per health facility. The information to be collected being sensitive, privacy and confidentiality were ensured for the participating clients. The clients who were not at the health units on the day of the study were identified from the records and followed up through contacts with the local authorities in their village. Findings A total of 440 people were interviewed. They were 400 hundred community respondents (200 men and 200 women) and 40 key informants (16 Survivors of GBV, 13 LC chairmen, 1 police officer, 1 psychologist, 1 police surgeon, 2 psychiatrists, 2 general medical doctors, 3 clinical officers and 1 nurse). Their mean age was 32.4 years. Most of them were peasant farmers by occupation. Most of the female respondents (58% or 116/200) of the females had only attended primary school while 13.5% had never gone to school at all. Life time experience of GBV The respondents were asked whether they had ever experienced any of the forms of GBV. Table 1 below, shows the number and percentages of people who had ever experienced the forms of GBV. Generally, both females and males had been affected by GBV. Overall, the commonest form of violence was physical intimidation followed by verbal abuse. For females though, the commonest forms of violence ware sex-related i.e. defilement, indecent assault, verbal abuse, physical abuse, and marital rape. For males, the commonest forms of violence were physical threats, verbal abuse and physical beating. Of the 93 women who had been verbally abused 37.6% (or 35/ 93) had been abused by their partners, while 20.4% (or 19/93) were abused by their stepmothers. Among the males, seventy two (55.4%) of the 131 who had been verbally abused were abused by their wives. Of the 81 women who were beaten, 96.3% (or 78/81) were beaten by their partners. Others were beaten by a step mother, an aunt or a co-wife. Of the 56 men who were physically beaten, 67.9% (38/56) were beaten by their partners, 10.7% (6/56) by step mothers and 7.1% (4/56) by government leaders. At least 37% (74/200) of the women had ever experienced marital rape, while 13.5% (27/200) of the men had ever experienced marital rape. Rape had been attempted only in at least 20% (40/200) of the women and the perpetrators were mostly (77.5% or 31/40) village mates, relatives (10% or 4/40), and strangers (5% or 2/40). Others who attempted rape were a step father, a schoolmate and a friend. Ten percent (20/200) of the men had also experienced attempted rape, especially by older women (45% or 9/20), village mates (40% or 8/20), relatives (10% or 2/20) and friends (10% or 2/20). Almost two thirds of the females (124/200 or 62%) had had sex before the age of 18 years, and therefore been defiled, according to Ugandan law. These included those who got married before age 18. The defilers of females were male village-mates (56.5% or 70/124), husbands (33.1% or 41/124), schoolmates 8% or 10/124), friends (1.6% or 2/124) and a stranger 0.8% or 1/124). Only 11 (or 5.5%) males were defiled. The defilers of males were mainly (54.5% or 6/11) female village-mates of similar age, followed by older women (18.2% or 2/11), and a relative (9.1% or 1/11). As many as 16% (or 32/200) of the females had ever been raped compared to 9% (or 18/200) of the males. Of those females who had ever been raped, 81.3% (or 26/32) had been raped when they were between 10-18 years of age. Only one was below 10 years and 5 were above 18 years. The 32 females were raped mainly by village-mates (56.3% or 18/32), current husbands but before marriage (25% or 8/32), and one case each of a friend, a house-boy, a relative and an older man. Of the 18 males who had been raped, (83% or 15/18) were raped when they were between 10-18 years. Two had been raped at ages above 18 years and only one had been below 10 years. Males were raped by female village-mates (69% or 11/18), older women (12.5% or 2/18), and one case each of an aunt, a relative and the current partner but before they married. At least 77 (or 38.5%) of the women had ever been threatened physically and 28.6% of these (or 22/77) were threatened by their partners, and 7.8% (or 6/200) by co-wives, while for men, 8.4% (or 13/155) of the men who were threatened had been threatened by female relatives. Indecent assault was more common among females than males and it was mainly perpetrated by village-mates and school-mates. For 14.5% (or 29/200) females, their first sexual encounter was by force, compared to 8.5% (17/200) for males. Only 9 females (or 4.5%) admitted that to having ever caused any gender-based violence compared to 57% (or 114/200) of the males who admitted. Five women (or 2.5%) admitted to ever forcing their husbands into sex, and only two (or 1%) admitted to having verbally abused them. Two (or 1%) admitted to having beaten co-wives. Thirty two (or 16%) of the men reported ever beating a partner, but no woman accepted to have ever beaten a partner. A few women only accepted to hitting back when attacked. Males admitted to have caused the following abuses: verbal abuse (24% or 48/200), beating (22% or 44/200), indecent assault (5% or 10/200), defilement (6% or 12/200), marital rape (3.5% or 7/200), attempted rape (3% or 6/200), intimidation (1% or 2/200), rape (0.5% or 1/200) and threats (0.5% or 1/200). Their victims were their wives (30.5% or 61/200), village-mates (18% or 36/200), children (6% or 12/200), relative (7.5% or 15/200), mother (0.5% or 1/200) and their boss (0.5% or 1/200). During the interviews, some women broke down into tears. Some of the pregnant women had left their husbands simply because of violence, and they were staying with their parents at the time of the study. Some men were also on tension during the interviews and kept peeping outside to make sure their wives did not hear what they were saying. According to the psychiatrist in one of the hospitals, women were the most affected by GBV. They presented to him with depression and stress. Actions taken by the survivors after gender-based violence The respondents were asked the action they took in response to the abuse. Table 2 shows what they did. Generally, most respondents never reported GBV incidents to anybody. Some reported to local elected authorities. Some women also reported to their relatives, especially if abused by their husbands. A few, most likely those who got injuries, reported to a health facility. Only one woman reported to have had no money to pay to the LC court at the time of the violence. Some women had left their former partners because of violence and had acquired new partners at the time of the study. For the females who reported to local authorities, 69.5% (or 16/23) reported to have received satisfactory assistance such as a letter referring them to the police or settlement of the case altogether. However, 34.8% (or 8/23) were not satisfied with the handling of their case. Most of the females who reported to police reported satisfaction with the assistance received. Police assistance included arrest of the perpetrator, settling the case and giving police forms to the victim to go for medical examination. Survivors' experiences at the health facilities Some three of the twenty females (or 15%) who reported to health facilities found difficulties obtaining money to go for medical check up compared to 40.6% (or 13/32) males. Most of the survivors who went to a health facility reported to have received assistance satisfactory to their expectations (100% for women and 90% for males). Satisfactory assistance at the health facility included medical examination, treatment or being given a prescription. Those who reported lack of satisfactory assistance at the health unit reported lack of free medicines, absence of doctors, long waiting time and lack of information by the health workers. Only four female survivors had been admitted to a health facility after the violence and only 5 survivors reported to have received counseling. Even then, only three of them received counseling in privacy. Services actually rendered to GBV survivors in health facilities Table 3 shows the distribution of services rendered at 5 selected health facilities in the district, including the three hospitals. Of the 23 required conditions listed above, only 5 (or 21.7%) were fulfilled by all the health units studied. Most of the conditions were not fulfilled by any unit at all although some were fulfilled by some units. Although Family Planning services were provided in all the units studied, none of them gave emergency contraceptives to rape cases. The health workers explained that most survivors reported late when most of the evidence was already destroyed through bathing and change of clothes. Laboratory investigations like vaginal smears were only rarely carried out in one hospital due to lack of facilities in other units. Counseling of GBV survivors was rarely done and documentation of GBV information was only done by the doctors and clinical officers who filled the police forms. Even then, it was done for police purposes and no copies of the detailed records were kept at the health units. Records for assault by partners or relatives were simply included in general registers and there was no further GBV-specific sub-analysis. The situation was the same at the police station and it made identification and retrieval of GBV records difficult. The records were not used for policy development or action to prevent GBV or improve the management of cases. According to the two psychiatrists in two of the hospitals, they sometimes assessed abuse in psychiatric management. A psychiatric assessment tool was used in one hospital, whenever it was suspected that a patient had a psychological problem. Patients were usually identified by chance and most of them escaped unnoticed. Where systematic screening was tried, the victims were not open and the scheme was not successful. The survivors were not open especially if they came to the health facilities with their relatives. They mainly came in with depression and were only identified through detailed analysis of their social history. The survivors so identified were usually counseled. Most of them were women. The health workers reported that GBV counseling requires plenty of time which they could not afford due to a shortage of staff. They reported that in case of GBV against children, the parents were also affected and they too needed counseling, thus doubling the workload. In some cases, the extra investigations to be done required money because they had to be undertaken in private laboratories. Those survivors who lacked the funds, about UGX 10,000 (US$ 5.5), were not able to get full investigations. This made the health workers in public facilities only treat the victims without filling the police forms, which require details of laboratory results. In other cases, the survivors were required to and could not afford to pay funds to facilitate the health workers to go to testify in court. Since only the doctors were allowed to examine the victims and fill the police forms, health workers in the rural lower level health units tended to refer the survivors to the hospitals, and some survivors could not afford the transport costs thereof. Another challenge was that most health workers were not properly trained to carry out forensic examination and could often miss crucial evidence or did not feel confident to testify in court. As a result, they tended to avoid such "police cases". Even in the hospitals, since most of the doctors were engaged in administrative duties, the survivors were always examined by clinical officers who have limited or no training in forensic examination. At the police, records were hard to come by and were GBV records were scattered in different sections and hard to retrieve and aggregate. The officers reported that that most rape cases did not report to police and most of them were solved by the local authorities on a cultural basis. Those who reported were examined by the police surgeon or sent to a government hospital. The survivors were supposed to be escorted by a police officer to the hospital. Female victims were supposed to be accompanied by female police officers but this was not always possible due to shortage of staff. The victims were never sent to private hospitals and clinics because their doctors never responded to court summons. The police found it easier to trace doctors from government health facilities to give witness in court. However, the government doctors needed to be paid some (unofficial) money before they could do the forensic examinations and accept to testify in court. This made matters difficult for the survivors. There was only one police surgeon who could provide free services but he was responsible for a large region covering the five districts of Kasese, Kamwengye, Kyenjojo, Bundibugyo and Kabarole, with a population of about 2 million people. Therefore, the police surgeon was not always available at any one station to do timely investigations since he had to move to other districts. Sixteen GBV survivors (2 males and 14 females) were followed up for specific interviews. Eight of them were below 18 years, including two children below 10 years. Eight of the victims had been raped, five were defiled, 2 were beaten and one child was deliberately burnt in a house. Five survivors had been raped by village-mates, two by their house-boys and one by a brother-in-law a few weeks after the death of her husband. Defilement cases were mainly committed by village mates (3/8), a cousin (1/8) and a house-boy 1/8). Among those defiled, there was one mentally handicapped girl who had been repeatedly defiled by their house-boys. The mother now had difficulties in looking after her and her children resulting from the rapes. From the FGDs, men reported that gender-equality and mainstreaming policies of the government of Uganda had given the women "too much liberty, which makes every woman do what she wants" (FGD of men, Burahya). This, according to the men, includes the ability to beat men up, in collusion with the children. Discussion The study shows that gender-based violence was very prevalent in Kabarole District, although many cases were not reported to health workers or any authority. Most cases were handled by the local authorities in a cultural context and out of the formal legal and health system. As a result, many cases are suppressed by the cultural approach which is somewhat tolerant of some practices e.g. wife-beating. This is exemplified by advice to a battered woman to "go back home and be a good wife". However, apart from trampling on the rights of the victims, some of the violence could result in serious bodily injuries which go untreated if cases have been solved privately, or into long-term psychological effects on the victim or their parents. Although there were some male victims of GBV, most were women. This is in consonance with what has been seen in many other societies. In Samoa, it was found out that only 2% of men experienced physical violence, while it is 19% in this study. However, this higher percentage is possibly due to the fact that most men who reported physical abuse, referred to the injuries they sustained while fighting their wives. It was most likely that women injured their victims in self-defence as earlier noted by Tibatemwa (1999). More women (37%) had ever experienced marital rape, compared to 13.5% of the men although only 2.5% of the women admitted ever forcing their husbands into sex and 3.5% of the men admitted ever forcing their wives into sex. In Samoa, 3% of the men reported sexual violence by their partners (Garcia-Moreno et al., 2005). Marital rape by men was also reported by Heise et al (1994, in ISIS). In several Ugandan cultures, marital rape is neither recognized nor acknowledged. It is possible therefore that even the figures in his study are under-estimates of the reality. As a result of this cultural framework, many women have been put at risk injury and infections like HIV. This study reveals the case of one woman who was raped by her brother-in-law, possibly due to the cultural practices of wife-inheritance. Many people have acquired HIV due to such cultural practices. For a number of female and male respondents, their first sexual encounter was by force. This is similar to what was found by Garcia-Moreno et al. (2005) who found out that the first sexual experience of 5-14% of women in different countries was forced. The perpetrators of GBV were mainly people close to the victims e.g. relatives, partners, spouses, schoolmates and village-mates. Some of them were significantly older than the victims. This is in agreement with what was found earlier in Uganda that sexual abusers of young boys were usually older women (Uganda Law Reform Commission, 2000). After violence, some respondents were more likely to keep quiet about it than report to authorities. Instead, some survivors reported to their parents and relatives or just run away from their partners. Some of the respondents feared to report physical violence because of shame or for fear of retaliation in case the perpetrators were arrested. As a result, some people live in perpetual captivity to their spouses and some simply get bonded in the relationship, something akin to the famous Stockholm Syndrome, in which a captive feels safer with the abuser than with the formal protectors. Fear as a cause of Victims' keeping quiet was also reported in another study by Knight (1997) in USA. In many other studies, victims were also reported to have kept quiet over the abuses (Edwards, 1996; Garcia-Moreno et al., 2005). The police also reported that men never reported especially physical abuse by their partners, probably for fear of being ashamed. This fear was also reported in other studies (Canadian Nurses Association, 1992; AHURIO, 2003). Some GBV victims never reported to health facilities because of difficulties in access such as lack of funds and long distance. This stresses the importance of socio-economic status in influencing the management and outcomes of gender-based violence. Women who have reliable sources of income are more likely to report their violence to both legal and medical authorities for attention. This is likely to lead to timely intervention and hence minimization of complications of violence. The study also exposes the inadequacy of GBV services in the district. The infrastructure and staff (whether medical or police) are insufficient. Medical staff is not trained to screen for and manage GBV issues. Moreover, there is no policy and no standard guidelines for the management of the different forms of GBV. Currently, the management depends on the provisions in the law, which mainly address the legal concerns, but not medical and psychological aspects of gender-based violence. In Uganda's HSSP II, little mention is made of GBV. However, the strategic content seems to be focused on situation analysis. There are no concrete actions to be taken within the 5-year period until 2010. This suggests low priority attached by the Ugandan Ministry of Health to GBV issues, yet GBV is a common cause of morbidity and mortality in the health system. Generally, the quality of GBV care was poor, right from record-keeping to case management. The plausible explanation is lack of training, lack of motivation, inadequate staffing and lack of facilities. This is similar to what was reported in South Africa (Guedes (2004) where shortage of health workers had limited the provision of services like screening for GBV during ANC and counseling of HIV patients. A shortage of doctors was also reported in a study in the DRC by Pratt et al., (2004). There was no private space which could be used for handling GBV survivors and the laboratories were not well equipped for forensic examination. These findings had also been earlier highlighted in another study in Uganda (Uganda Law Reform Commission, 2000). In the study, GBV services were part of routine care and there were no special clinic days for it. This is also in line with the guidelines of the American Medical Association which recommends that (1992), assessment for abuse should be integrated into routine ante-natal care and psychiatric management (American Medical Association, 1992). However, in Kabarole, assessment for evidence of GBV was only done when abuse was suspected, even then, due to legal constraints, only doctors are allowed to do the assessment. Given that there are very few doctors especially in rural areas, the services are insufficient. Finally, the study observed that the only sector with which the health sector collaborates on GBV issues is the Justice, Law and Order sector (JLOS). Others like education, gender and culture, ethics and integrity, local government and administration are not in collaboration with the health sector in the fight against gender-based violence. Gender-based violence is a multi-sectoral problem which the health sector cannot manage to solve alone. Whereas the health sector can equip itself to manage the cases effectively, prevention needs to be handled with many other stakeholders. Therefore, there is need for proper stakeholder analysis before the health sector's policy on GBV is enacted. Thereafter, there need to be good and feasible plans for inter-sectoral collaboration on gender-based violence. Conclusion and Recommendations The study showed that because the Ugandan health system lacks a national policy, plan and guidelines for the management of gender-based violence, lower level health services such as those in Kabarole District are not sufficiently oriented to cater for victims of GBV. Gender-based violence was found to be very common in the district with 96.5% of a sample population of 400 people having experienced one form of GBV or other. The common forms of GBV identified in Kabarole district were physical, sexual and emotional abuse. More women had experienced GBV than men. GBV was most likely to take place between family members, especially spouses. Whereas women were more likely to abuse verbally, men were more likely to abuse physically. Victims did not always report violent abuse to authorities because of fear of shame, lack of money to process cases or because of cultural restraints to solve matters domestically. Victims would occasionally inform the police, inform their friends or relatives and were more likely to report very late to the health services, long after incriminating evidence had been destroyed. The health services were inadequately staffed and the staff did not have training in handling GBV cases. The health units were not capable of providing key services required to investigate GBV cases. Collaboration between the health sector and others in the management of GBV cases was limited to reports to the police and court testimony. There were no GBV preventive activities carried out by the health sector. There was no active screening for history of GBV and cases were discovered mainly after serious physical injury. The HMIS was not GBV-sensitive and data in the health system and the police were never analysed to determine the magnitude of the problem. In general, unless there was physical evidence of injury, GBV was not a priority in the district health system. Suggestions to improve the situation included that to the Ministry of Health to enact a policy on the prevention and management of GBV, accompanied by investments in the health system for that purpose. Investments could include specific training of staff to do health education, proper case management and counseling, conducting forensic investigations to preserve and collect evidence for use by the police and research on GBV; equipment of the health facilities _ at least at district level, with sufficient facilities to conduct forensic investigations; staffing the health facilities adequately, to reduce on staff workload and ensure improvement of the quality of patient care. In addition, the Ministry could revise the HMIS to demand for GBV data, in order to ensure that the data are collected, aggregated and analysed right from the lowest levels of the health system. District health services could expand intersectoral collaboration beyond the police, to include other stakeholder sectors e.g. education, probation, local government and other human rights organisations in the area. These could contribute to sensitizing the community on GBV through various means e.g. the media. The health services could also institute active search of GBV cases through probing history-taking and a generally raised index of suspicion. The health services could also open up examination of GBV cases to other staff cadres, in order to increase the possibility of prompt care and investigation. In the meantime, the managers of health facilities could include GBV training in the Continuing Medical Education (CME) to sensitize health workers on the identification and management of GBV cases. They could also allocate space to ensure privacy for investigation, counseling and follow up of GBV cases in their facilities. References
© Copyright 2008 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp08014t1.jpg] [hp08014t3.jpg] [hp08014t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}