 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
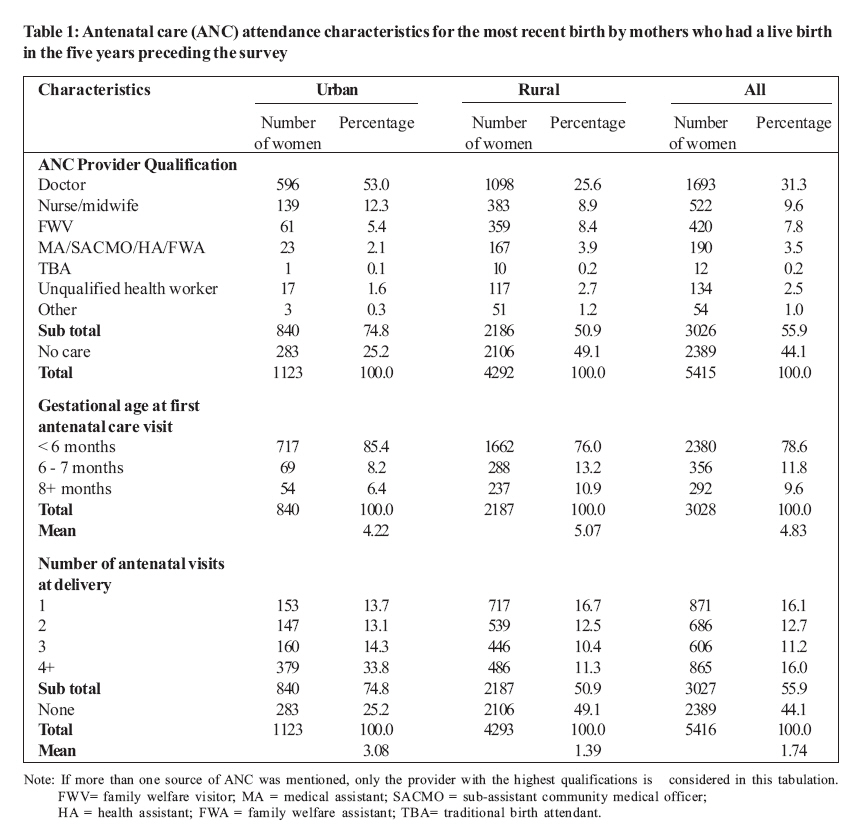
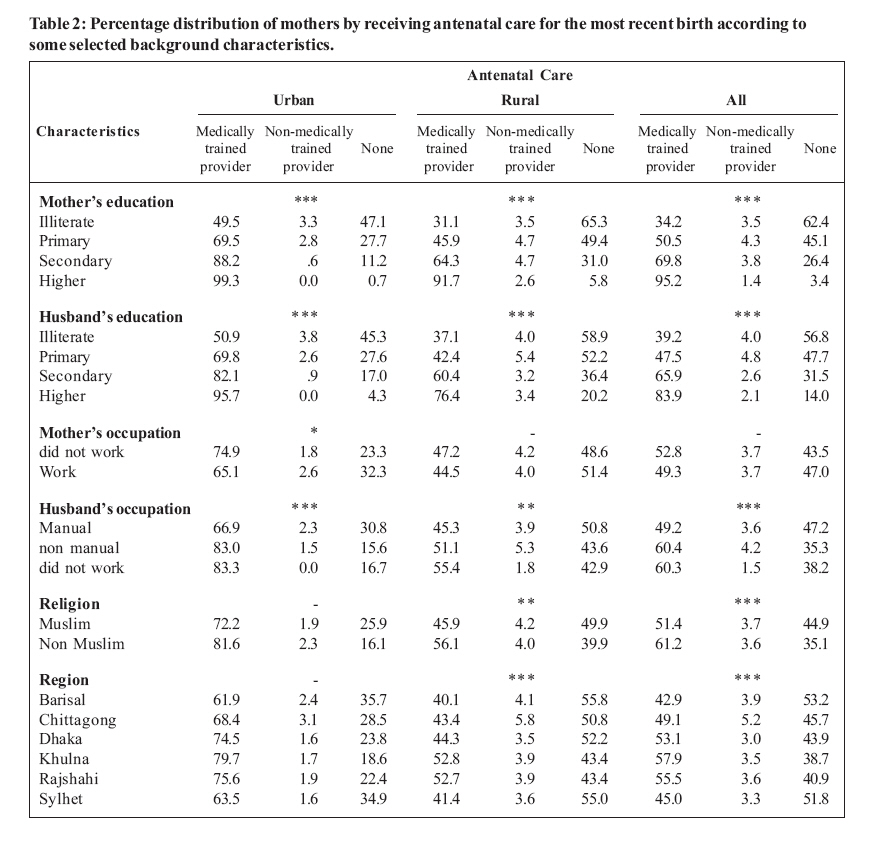
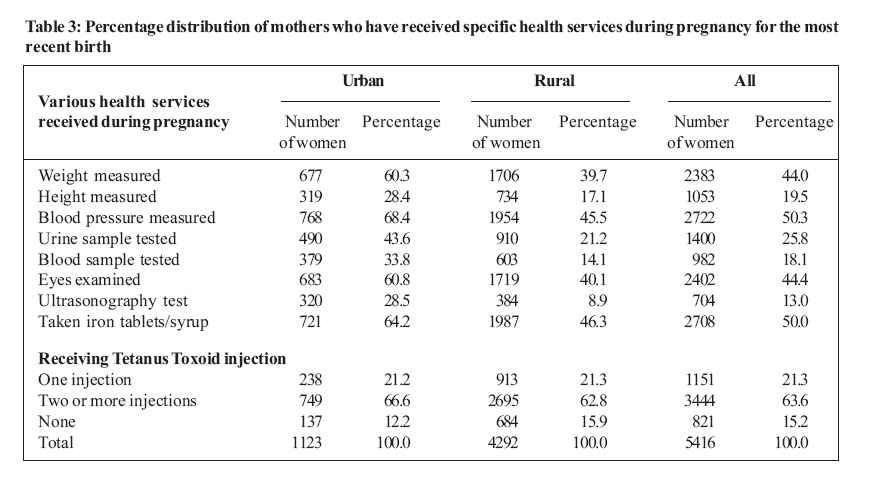
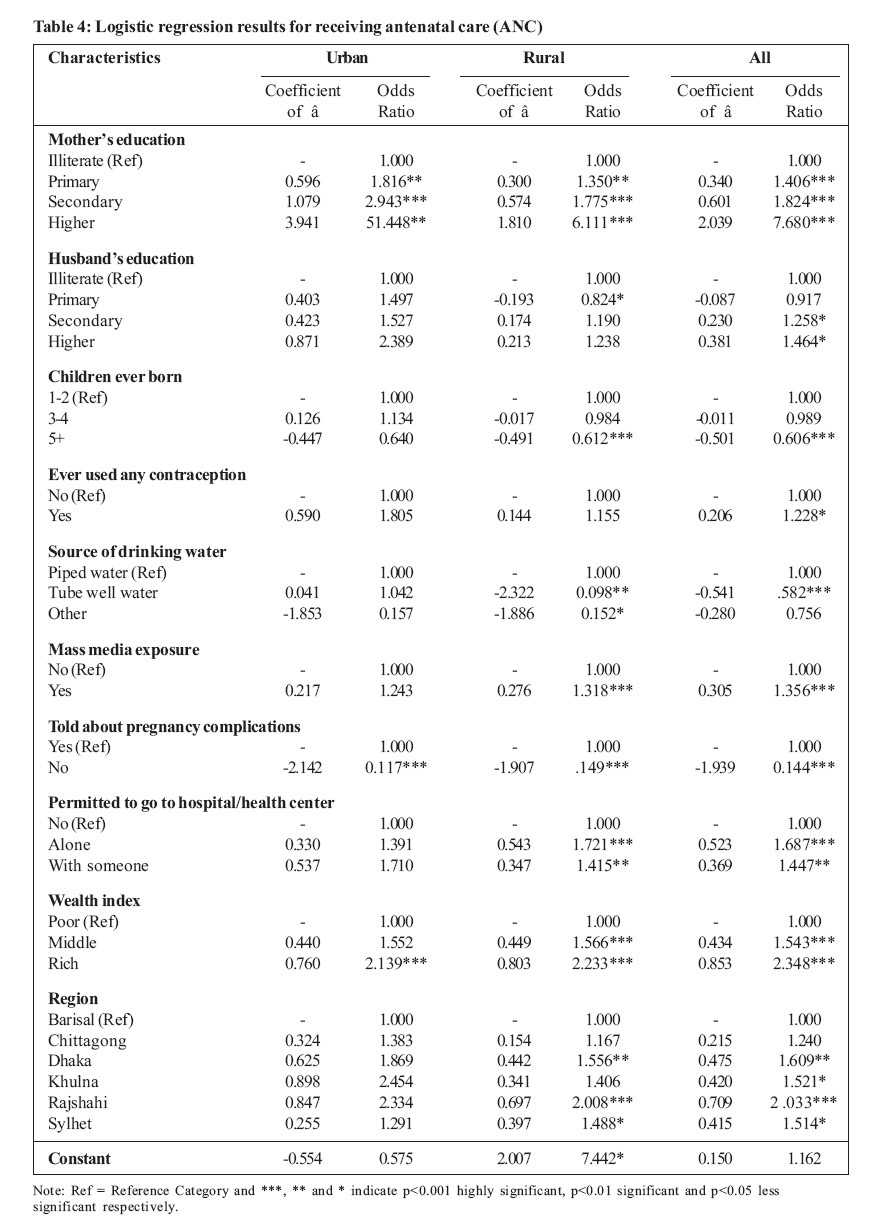
Health Policy and Development Journal, Vol. 6, No. 3, December, 2008, pp. 117-125 THEME ONE: HIV/AIDS, REPRODUCTIVE HEALTH AND RIGHTS Rural-urban differentials of utilization of ante-natal health-care services in Bangladesh Md. Mosiur Rahman, Md. Rafiqul Islam and Ahmed Zohirul Islam Department of Population Science and Human Resource Development, University of Rajshahi, Rajshahi-6205, Bangladesh Code Number: hp08015 Abstract Bangladesh has achieved important health gains over the last decade but there is still an enormous gap between rural and urban areas with regard to utilization of reproductive health care services. The study utilizes Bangladesh Demographic and Health Survey (BDHS) 2004 data to identify the more important factors affecting ante-natal health care services in the urban and rural areas. Findings reveal that there exist strong urban-rural differentials of receiving antenatal care. It was found that three quarters of urban women receive antenatal care compared to only half of their rural counterparts. Doctors form the highest proportion of antenatal care providers. The mean number of antenatal visits is higher among urban mothers than that of their rural counterparts. The study also unveils that the majority of urban mothers have their blood pressure and weight measured during pregnancy period while the corresponding figure for rural mothers is found to be low. Logistic regression analysis shows that a mother's education, children ever born, wealth index, telling about pregnancy complications and permission to go to hospital/health center are the significant determinants of receiving ANC. Other significant determinants include the source of drinking water, the region and the husband's education. Key Words: ANC, Pregnancy complications, Wealth index, Fertility preference Introduction Antenatal care (ANC) is essential for the health of both the mother and child. The risk of maternal mortality and morbidity as well as neonatal deaths can be reduced substantially through regular and proper antenatal care check-up and delivery under safe and hygienic conditions (Moller, et al. 1989, Joseph, 1989). Studies demonstrating the high levels of maternal mortality in developing countries and research identifying causes of maternal death have repeatedly emphasized the need for prenatal care and availability of trained personnel to attend to women during labor and delivery (Maine, 1986; Fauveau, 1988; Fortney, 1988). The importance of maternal health services in reducing maternal and infant morbidity and mortality has received significant recognition in the past decade (Ebrahim, 1982; Rosenfield and Maine, 1985; Herz and Measham, 1987). Data Sources and Methodology This study utilizes the data extracted from 2004 Bangladesh Demographic and Health Survey (BDHS 2004), which was conducted under the authority of the National Institute of Population Research and Training (NIPORT) of the Bangladeshi Ministry of Health and Family Welfare. The BDHS 2004 is a nationally representative survey from 11,440 ever married women of age 10-49 and 4,297 men aged 15-54 from 10,500 households covering 361 sample points (clusters) throughout Bangladesh, of which 122 were from urban areas and 239 from rural areas. Out of 11,440 ever-married respondents, 2,586 women and 8,854 women were taken from urban and rural areas respectively. The data were collected from six administrative divisions of the country- Barisal, Chittagong, Dhaka, Khulna, Rajshahi and Sylhet. Data collection took place over a five-month period from 1 January to 25 May 2004. In this study we considered only those women who had a live birth in the five years preceding the survey. To meet the objectives, this study uses bivariate analysis. Chi-square test is performed among the variables to identify interrelationship between the variables. Binary logistic regression model is used to examine the effects of demographic and socio-economic characteristics on the dependent variable. Findings Utilization of Ante-natal Health Care Services Antenatal care is the care for women during pregnancy. The reproductive health care services that a mother receives during her pregnancy and at the time of delivery are important for the well-being of the mother and her child. Antenatal care can be more effective in avoiding adverse pregnancy outcomes when sought early in the pregnancy and continued through to delivery. It can contribute significantly to the reduction of maternal morbidity and mortality because it also includes advice on the correct diet to the pregnant woman and the baby's medical care. The Bangladesh Maternal Health Strategy recommends at least three visits during pregnancy. The first visit is to be made soon after the woman realizes that she is pregnant. The second visit should be made between the fifth and seventh month of pregnancy. The third visit should be made at the ninth month of pregnancy. Additional visits should be made if any problems or danger signs arise. Antenatal care (ANC) utilisation was assessed according to the type of service provider visited, the number of visits made and the stage of pregnancy at the time of the first visit. The findings are presented in Table 1 below. Table 1 shows that whenever mothers sought antenatal care outside the home, doctors were the providers most commonly used by both urban mothers (53 percent) and rural mothers (25.6 percent), followed by nurses/midwives (12.3 percent for urban mothers and 8.9 percent for rural mothers). Half of the rural mothers (49.1 percent) and a quarter of the urban mothers (25.2 percent) still do not receive ANC. This may be due to low awareness of the importance of having antenatal checks or because services by qualified staff are too expensive or not available in the rural areas. The findings also elucidate that 85.4 percent and 76 percent mothers receive ANC before the sixth month of gestation in the urban and rural area respectively. Among all women who have received ANC, the mean number of months at first visit during pregnancy is 4.83. Urban mothers are thrice as likely to have four or more antenatal visits as rural mothers. The mean number of antenatal visits is 3.08 and 1.39 in the urban and rural areas respectively. A bigger percentage of rural mothers make only one antenatal visit before delivery and about 44 percent of all mothers did not receive any antenatal care at all. Urban - Rural Differentials in Receiving Antenatal Care In this section we present and discuss various impacts of some selected background characteristics on receiving ANC. From different literature sources, we selected those variables which are known to be associated with seeking for ANC. Table 2 above reveals that the higher the education of the mother, the higher the chances of seeking ANC services. In the whole country, while only 34 percent of illiterate mothers receive ANC, the level increases to 69.8 percent and 95.2 percent to women with secondary and higher education respectively. The proportion of mothers who receive ANC from medically trained providers also increases steadily with an increase in the education level of the mothers both in the urban and rural areas of Bangladesh. This study also indicates that the educational level of their husband has a clear influence on the attendance of ANC services by women, and that this effect is consistent for urban and rural women. Caldwell has suggested that men with higher educational attainment may play a more important role in child care decisions than men with less schooling (Caldwell, 1990). Only 39.2 percent of women whose husbands are illiterate receive ANC from medically trained providers. The proportion increases to 47.5 percent among those whose husbands have primary education, to 65.9 percent if they have secondary education and to 83.9 percent for those whose husbands have an educational level higher than secondary school. This could be because education influences the husbands' attitude towards modern medicine which, in turn, influences the wives' ability to use modern health care facilities. The result shows that the husband's occupation also has an effect on the likelihood of a woman to seek antenatal care. Women whose husbands have occupations other than manual labour are more likely to receive ANC (60.4 percent) from medically trained providers. However, the area of residence seems to modify this effect since manual labourers in urban areas also influence their wives to receive more ANC than their rural counterparts. Religion also seems to affect mothers' choice. The study depicts that non-muslim mothers attend ANC more than Muslim mothers (64.8 percent compared to 55.1 percent). Urban Muslim and non-Muslim mothers (72.2 percent and 81.6 percent respectively) attend ANC from medically trained providers more than their rural counterparts (45.9 percent and 56.1 percent respectively). Table 2 also shows that ANC attendance from medically trained providers is highest in Khulna Division and lowest in Barisal Division. In each division urban women attend ANC more than their rural counterparts. Women who access mass media (television, radio, newspapers) are more likely to obtain their ANC from medically trained providers than their counterparts who do not. In addition, urban women, who access mass media are more likely to attend ANC from medically trained providers compared to their rural counterparts and even their urban counterparts who have no access to media. The study also shows that the socio-economic status also affects the mothers' ability and choice to attend ANC. Utilisation of ANC seems to increase with the wealth index. Most (82.6 percent) of the rich women attend ANC from medically trained providers in the urban area as opposed to only 46.1 percent of poor women. Age also seems to be related to use of antenatal care from medically trained providers. Utilisation of ANC is higher among younger women than their older counterparts. Especially in urban areas, women in the age group 20-34 years attend ANC more than their counterparts in other age groups. A consistent negative relationship is observed between the parity of the mother and using ANC services. This effect is observed in both the urban and rural areas of Bangladesh. Both discussing about family planning with the husband and the desire for more children in the future are shown to lead to increased utilisation of ANC. We also observe from this study that the utilisation of ANC varies between those who have ever used contraception and those who have not. Mothers, who have used contraception, tend to use ANC than those who have not. The results also show that mothers who have attended ANC are more likely to describe pregnancy complications than those who have not. Health Services Received during Pregnancy Pregnancy complications are the important causes of maternal and child morbidity and mortality, and monitoring these complications is a crucial component of safe motherhood. A number of health care procedures is recommended to be performed to monitor and check the development of pregnancies. For women who had a live birth in the five years preceding the survey, the 2004 BDHS included a series of questions on whether they were told about the signs of pregnancy complications, whether they were weighed, whether their height and blood pressure were measured, whether urine and blood samples were taken, whether their eyes were examined, and whether they received iron tablets or syrup at any time during the pregnancy of their most recent live birth. Table 3 shows the various health services reported to have been received. Table 3 shows that the urban-rural differentials in receiving health services during pregnancy are quite large. In the urban area, 68.4 percent of mothers had their blood pressure measured and 60.3 percent have their weight taken during the ANC. The corresponding figures for the rural mothers are 45.5 percent and 39.7 percent respectively. Only 19.5 percent of the mothers had their height measured, while only 25.8 percent had their urine tested and 18.1 percent had their blood sample examined. The results also show that 88 percent of urban and 84 percent of rural mothers respectively receive tetanus toxoid (TT) injection during pregnancy. Factors Predicting the Use of Antenatal Care: Multivariate Analysis Binary logistic regression is the multivariate analysis technique used to predict the presence or absence of a characteristic or outcome based on values of a set of predictor variables. It is similar to linear regression model but it is suited to models where the dependent variables are dichotomous. Since our dependent variable is dichotomous, we employed the binary logistic regression model. Here, the model fitted considers antenatal care during pregnancy as the dependent variable and it is coded as 1 if the mother receives antenatal care from medically trained providers, otherwise it is 0. The corresponding results are presented in Table 4. Maternal education appears to be the most significant determinant of using ANC. Furthermore, the parity, the husband's education, exposure to mass media, hearing about pregnancy complications, permission to go to hospital or health center, geographical region of residence, wealth index and even the source of drinking water also significantly influence the likelihood of antenatal care utilisation. These are true only for rural women. For urban women, only the mother's education, wealth index, and hearing about pregnancy complications show significant effect on using ANC. Table 4 shows that, in the urban areas, mothers with primary, secondary and higher education were 1.816, 2.943 and 51.448 times respectively more likely to attend ANC from medically trained providers than illiterate mothers. About 88 percent of mothers who cannot describe pregnancy complications were less likely to have taken ANC from medically trained providers than their counterparts in the reference category. Urban middle class and rich mothers were 1.552 and 2.139 times respectively more likely to receive ANC from medically trained providers compared to their poor counterparts. In another model, in the rural area mothers with primary, secondary and higher education were 1.35, 1.775 and 6.111 times more likely to receive ANC from medically trained providers compared to their illiterate counterparts in the reference category. Mothers who have 5 or more children were 39 percent less likely to receive ANC. Mothers who drink tube-well water are 90 percent less likely to take ANC from medically trained providers than those mothers in the reference category. Mothers who access mass media were 1.318 times more likely to attend ANC than those who had no access. Mothers who can not describe pregnancy complications were less likely to have taken ANC from medically trained providers than their counterparts in the reference category. Rural women, who were permitted to go to hospital / health center alone, were 1.721 times more likely to attend ANC than those women in the reference category. Middle class and rich mothers were 1.566 and 2.233 times more likely to attend ANC from medically trained providers than their poor counterparts in the reference category. The respective odds ratios indicate that mothers of Rajshahi, Dhaka, and Sylhet divisions were 2.008, 1.556, and 1.488 times respectively more likely to attend ANC by medically trained providers compared to those of Barisal division. Discussion In this study we considered only those women who had had a live birth in the five years preceding the survey. There existed strong urban-rural differentials in receiving antenatal care in favour of the urban woman. Rural women were more vulnerable because only half of them received ANC. Among the antenatal care providers, doctors were the most utilised in Bangladesh. The mean number of antenatal visits by urban mothers is higher than that of their rural counterparts. The observations above could be related in that the cost of medical consultation is usually high and could be a barrier to rural poor women's access to ANC. Most urban and rural mothers begin attending ANC before the sixth month of pregnancy. This suggests that the level of awareness of the need to attend ANC is high, but that there should be other barriers. However, the quality of ANC offered leaves a lot to be desired. For example, in the urban areas only 68.4 percent of mothers have their blood pressure taken and only 60.3 percent have their weight taken. The corresponding figures are worse for the rural mothers at 45.5 percent and 39.7 percent respectively. It is also possible that the quality of care offered is another `push' factor for mothers not to attend the ANC. It had already been demonstrated that older, poor, and less educated women are less likely to seek ANC (Thomas et al. 1997). This study therefore also confirms those earlier findings. The observed reduction in utilisation of ANC with age and parity might be because of a perception of development of "experience" in giving birth. However, health care personnel should always take it upon themselves to educate the mothers that each pregnancy is a unique experience that comes with its own challenges. Further investigation needs to be done on other socio-economic variables that can explain the differences in ANC attendance which is highest in Khulna and lowest in Barisal divisions. In each division urban women attend ANC more than their rural counterparts. This may be related to the availability of health personnel which is more in urban areas than rural areas. The study also shows that as the wealth index goes up, ANC attendance also increases among both urban and rural women. The general perception is that the wealthy are able to use ANC more than the poor (Hadi and Gani, 2005). This latter observation suggests that financial barriers are significant in influencing the utilisation of ANC. A study by Ahmed and colleagues (2003) found that educated mothers were much more aware about ANC than less educated and illiterate ones. We also observe from this study that the utilisation of ANC increases steadily with an increase in education level of the mothers both in the urban and rural area of Bangladesh. This goes further to affirm what is known that education increases the awareness on causes and consequences of ill-health, and thus increases the demand and utilisation of health services. Women whose husbands are non-manual workers are more likely to receive ANC from medically trained providers as compared to those women whose husbands are manual workers in both the urban and rural areas. Non-Muslim mothers receive more ANC from medically trained providers than their Muslim counterparts among both urban and rural mothers. Socio-religious prejudice seems to be a significant barrier to pregnant women about receiving treatment from male doctors. Conclusion The overall scenario of ANC utilization in Bangladesh is not satisfactory. In addition, there exist strong differentials in utilisation such as education status, urban/rural residence, and socio-economic status. However, most of the ANC utilisation seems to be heavily skewed to the rural areas. The study therefore concludes that the Bangladeshi Government needs to act deliberately to address the variables responsible for the observed rural-urban maternal health care differentials. There are a number of measures that can be taken to this effect, including increasing the number of visits by FWV/FWA to rural women during pregnancy, establishment of Union Health & Family Welfare Centers, appointment of doctors in these centers, training and recruitment of female doctors, provision of sufficient education for both urban and rural women and men, which will increase their knowledge about reproductive health, among other benefits. References
© Copyright 2008 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp08015t2b.jpg] [hp08015t1.jpg] [hp08015t4.jpg] [hp08015t3.jpg] [hp08015t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}