 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 6, No. 3, December, 2008, pp. 126-141 THEME ONE: HIV/AIDS, REPRODUCTIVE HEALTH AND RIGHTS Factors related to the uptake of natural family planning by clients of catholic health units in Masaka Diocese, Uganda Catherine Nakiboneka* and Everd Maniple# *Corresponding author, Advisor on PNFP Health Training Institutions, Uganda Catholic
Medical Bureau, Kampala. E-mail: cnakiboneka@ucmb.co.ug Code Number: hp08016 Abstract Globally and locally in Uganda, family planning (FP) is promoted to enable individuals and couples to space and limit childbirth. FP promotion is based on demographic and health concerns and basic human rights. Clients can use either artificial family planning (AFP) or natural family planning (NFP) methods but none is 100% effective. Whereas NFP methods are known to be free from side effects, with no continuous costs, and widely accepted by most religions and cultures, most clients use AFP methods despite their many side effects and costs. The Roman Catholic Church (RCC) opposes AFP methods on fundamental grounds such as the definition of the onset of life and the purpose of sexual union. Additional reasons fronted by the church include the potential misuse of AFP methods and the false sense of security they impart to the users. This study set out to find out how health services under the RCC promote the use of NFP methods in an area of heavy RCC presence, and how these efforts translate into uptake of the methods. It shows that despite the recommendation of NFP methods, RCC health units did not have staff trained in promoting and offering NFP methods. There were no budgets, supplies, registers, teaching AIDS, and no records of NFP clients were kept. No space for NFP clinics was provided and there was no arrangement for continuous professional education (CPE) for NFP providers. Basic knowledge about NFP e.g. the role of breastfeeding and periodic abstinence was acquired from friends. Knowledge about NFP methods was insufficient among clients to the services and in some health workers. Most of the respondents, of which 76 %( 154/202) were Catholics had more information about AFP methods and knew where to access them. The study recommends that RCC authorities in Uganda, as the main champions of NFP, need to provide political commitment to NFP, invest more in and reinvigorate the teaching of NFP methods through their structures. In addition, there is need for support supervision on NFP access and use within RCC health facilities. Introduction Globally, family planning (FP) is promoted as a mechanism to address the reproductive health needs of men and women, as well as the crucial challenge of rapid population increase (PAI, 1999). The world population passed the six billion mark in 1999 and over three billion people survive on three dollars or less per day (UN, 1999). Reproductive rights rest on the respect of the basic right of all couples and individuals to choose freely and responsibly the timing of conception of their children, the number of children to have, the time spacing of the children and to access the information and means to space them (WHO, 2004). The Alma Alta Declaration on Primary Health Care cited FP as one of the key strategies to achieve a better quality of life for all people (WHO and Unicef, 1978). In 2002, the Uganda Population and Housing Census showed that Uganda had 24.4 million people, with an average growth rate of 3.4% per annum, much higher than the sub-Sahara African average rate of 2.1% (UBOS, 2005). By 2015, the Uganda government is committed to reducing the population living in absolute poverty to 10%, infant mortality rate to 41/1000 live births, child mortality rate to 60 per 1000 live births, and the maternal mortality ratio to 131 per 100,000 live births (MOH, 2005)). It also focuses on decreasing the high total fertility rate from 6.9% to 5.4%, mainly by increasing the contraceptive prevalence rate to 40% and the Couple Years of Protection (CYP) to 494,908 by the year 2009. It is proposed to increase the range of FP services by emphasising an increase in the availability of logistics and accessibility of the services (MOH, 2005). Over time, there also increasing calls for legalisation of abortion in Uganda, partly for population control and increasing the safety of a covert and hazardous practice, but also partly to allegedly enhance the reproductive health rights of women who, if the pregnancy is unwanted or may put their lives at risk, should have the right to decide whether to retain it or not. The latter proposal and the promotion of contraceptives go against the teaching of the Roman Catholic Church (RCC). For its part, the RCC teaches that children are a blessing to married couples basing on the biblical statement of God "….Be fruitful and multiply…" (Genesis, 1:28). Many proponents of artificial birth control have always accused the RCC of insensitivity to the socio-economic challenges due to large family sizes and populations. However, after its second Vatican Council (Vatican II), the RCC officially reaffirmed its acknowledgement of the genuine need for birth control and child spacing. It acknowledged the presence of pregnancy-related risks to the mothers' and the children's health. It also acknowledges the economic difficulties associated with large unplanned families, and the limited resources especially in developing countries (Pope Paul VI, 1968). However, it differs from other proponents of FP over the means by which to achieve the goals of birth control. One fundamental point of disagreement between the RCC and other proponents of birth control is the point at which life begins. Because of this, the RCC officially recognizes natural family planning (NFP) as the only genuine, legitimate and recommendable method of birth control because it does not interfere with the openness of the marriage act to transmission of life and does not interrupt primordial and defenceless life. This implies that if the couple wishes to postpone pregnancy they abstain from sexual intercourse during the fertile period and in case there is unintended pregnancy, it should be preserved as a marriage gift. According to the RCC, all other methods of FP frustrate the natural processes through interruption by mechanical devices, or chemical interventions (Karl, 1985). The natural methods are also morally accepted by the RCC on the grounds that they enhance and intensify the matrimonial relationship between spouses (Sin, 2001). Uganda, about 40% of whose population is Catholic, would therefore be expected to be a haven of natural family planning, with strong and visible opposition to contrary proposals. This study set out to find the practice of natural family planning in the Masaka Diocese region, covering the four districts of Masaka, Rakai, Sembabule, Kalangala and Lyantonde. Due to historic inter-religious conflicts of the late 19th century, it is also one of the most Catholic-inhabited areas of Uganda, with about 60% of its population in following the Catholic faith (UCS, 2004). The area has 5 hospitals (including two of the RCC), 16 health sub-districts and 155 lower level health units (LLHU) among which 26 belong to the RCC (MOH, 2005). Problem Analysis Large families and short birth intervals are closely associated with poverty and poor health. The children are prematurely weaned and deprived of the required antibodies, nutrients, and love from the mother and they are likely to suffer from malnutrition with its attendant poor mental and physical development. Frequent births usually lead to lack of material resources, overcrowded housing, and poor hygiene and sanitation for the children. Similarly, frequent pregnancies lead to maternal depletion, anaemia and infection. So, the mother, the unborn child, and the living children are all negatively affected by frequent births, not to mention the entire household and the country. Such consequences strain the country's resources, lead to food scarcity, wars over space and resources, environmental degradation, high school costs, increased pollution and overcrowding (UPPAP, 2003). FP is one way of reducing the maternal mortality ratio, high rates of infant and child morbidity and mortality and promoting optimum individual and family health and wellbeing. However, FP use varies according to religion or cultural values, myths, knowledge, promotion and marketing, effectiveness of the method, marital status, sex, age, policies, social and economic factors, as well as the attitudes of clients and providers. The Uganda government's national FP strategy is to increase access to FP in all public health units and to intensify information, education, and communication for FP (MOH, 2005). However, its approach focuses only on the use of artificial methods of family planning. On the contrary, the Roman Catholic Church, a major partner in health care delivery and development in Uganda, approves the use of only natural FP methods by its adherents and in its health units. It considers natural FP as the only morally legitimate means of birth control and child spacing. RCC health facilities, which operate within the framework of the national health policy and in partnership with the government, are faced with the challenge of delivering NFP only in a policy framework which only recommends and supports artificial FP. With the two bodies recommending divergent approaches, and the government taking aggressive social marketing for artificial FP only, the extent of use of natural FP in RCC health units or even among Catholics is not known. This study aimed at establishing the extent and the factors that affect uptake of natural FP in RCC health units, in the hope that this knowledge would provide information for RCC leaders and health workers to act in support of natural FP. It is envisaged that increased uptake of natural FP complements the artificial FP used by non-RCC adherents and ultimately contributes to the reduction of the problems associated with large unplanned families and frequent pregnancies. Objectives of the study The study, done in mid 2006 had, as objectives: to find out the utilization of natural FP methods in RCC health units of Masaka Diocese; to find out the characteristics of clients practicing natural FP; to assess the knowledge of natural FP methods by the general clients of the RCC health units; to establish the attitudes of the clients and health workers towards natural FP methods; to assess the effectiveness of the natural FP methods used by clients; and to assess the quality of natural FP services in RCC health units of Masaka Diocese. Literature Review The Global Policy Forum reported that, worldwide, roughly 125 million women indicate a desire to plan their families but are not currently using any contraceptive method (Global Policy Forum, 2003). Preventing high-risk pregnancies through increasing the availability of family planning services could also save at least 25 percent of the women's lives and those of their babies currently lost through pregnancy and childbirth. An average woman in the world now bears just 2.69 children in her reproductive lifetime while a Ugandan woman bears 6.9 children (Longman, 2004), yet their average desired fertility was 5.3 in 2001. Uganda's second Health Sector Strategic Plan (HSSP II) set specific targets in Uganda National Minimum Health Care Package (UNMHCP) for Sexual and Reproductive Health and Rights (SRH). In the UNMHCP, FP services specifically target artificial family planning methods as the core interventions for reproductive health (RH) services. It is hoped that they would reduce the total fertility rate (TFR), cover the unmet FP needs and contribute to reduction of high maternal, infant, child morbidity, and mortality respectively (MOH, 2005). However, the RCC has persistently upheld natural FP methods, as the only moral means of spacing or preventing childbirths. According to the RCC, natural FP should be taken primarily in the context of matrimonial love and family life, and not simply as another method of fertility control (Coleman, 1997). The 1994 Cairo international conference on population argued that FP programmes must be part of a wider approach to population growth regulation and health development. FP increases women's control over their own bodies, gender equality and enhances their health levels (Cohen, 1995). During the conference it was also emphasised that rapid population growth, especially in sub-Saharan African countries, cannot keep pace with the available resources. If unchecked, it would result in malnutrition, lack of housing, unemployment, shortage of social services, environment degradation and street children (Cohen, 1995). In response to the conference, Pope John Paul II commented that certain fringe groups within developed societies want to impose a lifestyle that might not be accepted by all countries (Kanyandago, 1994). The consequences of unplanned large families extend to the community and the country at large. High population growth puts enormous burden on the provision of education, health, water and sanitation plus other social services. With limited resources, high fertility depresses savings and makes it difficult for most families to adequately feed, clothe, house, and educate their children (Namara, 2006). Therefore, helping them to reduce unintended pregnancies would slow population growth and reduce pressure on natural resources. Some societies and individuals believe that a large population promotes agriculture, military and political power (Allan and Allen, 1996). As a result, strategies for limiting population growth as a means to acquire good standard of living, are counteracted by the combination of strategies that society, religion, culture and poor people adopt in pursuing their livelihood or the survival of their values. However, if the views above were to be true, Ethiopia and Bangladesh, with populations of over 100 million, would not be in deep poverty (Namara, 2006). In Uganda, successive Participatory Poverty Assessment process (UPPAP) reports identified large families as a cause of poverty (MOFPED, 2002). In fact, high fertility rate wipes out development achievements and without action taken, by 2013/14 the number of Ugandans living in poverty was estimated to increase to 10.3 million (Helmut, 2006). In Asia and South America, success in reducing fertility levels resulted from social and economic development focused on raising the level of education and health services rather than FP programmes (Uche et al., 1994). Similarly, as the problems of Uganda cannot be attributed only to high population growth, they cannot be solved by FP alone. Presently Uganda promotes FP as a human right and as an approach with a key role in reducing the proportion of high-risk pregnancies and births. This is in line with the WHO recommendation about freedom to make reproductive choices (WHO, 2004). Family Planning Methods and their effectiveness WHO defines Natural Family Planning (NFP) methods as those used for planning and preventing pregnancies through observing naturally occurring signs and symptoms of the fertile and infertile phases of a woman's menstrual cycle, and Artificial Family Planning (AFP) methods as those which prevent conception by application of any mechanical, chemical, surgical and pharmaceutical methods (WHO, 1988). NFP methods include abstinence, the Cervical Mucus Method (Billings' method), the Basal Body Temperature (BBT) Method, the Sympto-thermal (Multiple indicator) method, the Rhythm (Calendar) Method, the Standard Days method (SDM), the Lactation Amenorrhoea Method (LAM) and Coitus Interruptus. AFP methods include Hormonal Methods such as Oral Contraceptives (Pills), Injectable Contraceptives, and Implants. They also include Barrier Methods e.g. the use of physical barriers like diaphragms, condoms and cervical caps or chemical barriers like spermicides. Of these, the condom is also the only method that may prevent sexually transmitted infections (STDs) including HIV/AIDS if used correctly all the time. Other AFP methods include Intrauterine Devices (IUDs) and Long-Term Permanent Methods (LTPM) e.g. Bilateral tubal ligation (BTL) and Vasectomy. The proliferation of both natural and artificial family planning methods suggests that none is fully effective. Regarding natural FP methods, Dicker et al., (1989) noted that the success of a family planning method depends on the indicators and validity of the rules that are used to apply it; the type and quality of teaching given to the users; the ability of a woman to observe and interpret her fertility signs; the time allowed to learn the method; record keeping; partner cooperation; ability to observe periodic abstinence; the age of the users; level of education; culture and religion of the client. McSweeney (1992) also pointed out the importance of alcohol and drug abuse in the failure of abstinence-supported methods. Trussell and Kost (1987) explained that failure of a method may result from the technical limitation of the method or simply from improper use. User factors, contribute a lot to the failure of the methods. They also depend on the teaching the client receives. Incorrect teaching usually results into clients' misunderstanding of the instructions. After failure of contraception, a couple may still choose to use the same method to prevent subsequent pregnancies if the circumstances of failure were understood and were under their control. The effectiveness of natural FP methods largely depends on accurately predicting when ovulation will occur, or detecting when it has happened, so that the couple can abstain from sexual intercourse, and on the willingness of both partners to abstain. Roman Catholic Church Position on Natural Family Planning The RCC bases itself on the papal encyclical Human Vitae (Pope Paul VI, 1968) to teach that every sexual act of a married couple must remain open to the transmission of life. To postpone pregnancy, married couples are advised to have sexual intercourse only during the infertile days when no mature ovum is expected and to abstain from sex when the period is unsafe (Karl, 1985). This is the natural way of planning the family size. Zimmerman (1998) notes that observation of natural FP leads to self-control and a spirit of sacrifice in consideration for one's own spouse. Accordingly, natural FP is considered a fulfillment of God's laws with gratitude for the graces one receives in marriage. However, Aguilar (1998) observed that some people use sexual intercourse for exploitation, conquest, humiliation, and anger, whereas it should be an expression of the deeper human emotions of love, joy, and spiritual closeness. Jaime Cardinal Sin (2001) disagrees with the arguments that both artificial FP and natural FP methods aim at preventing pregnancy, and that if contraception is inherently sinful so is natural family planning. A contraceptive act involves the choice to do something before, during, or after the sexual act, which destroys the possibility of conception (Karlen, 1991). In the human and Christian vision of marriage, Pope Paul VI stated about abortion that:
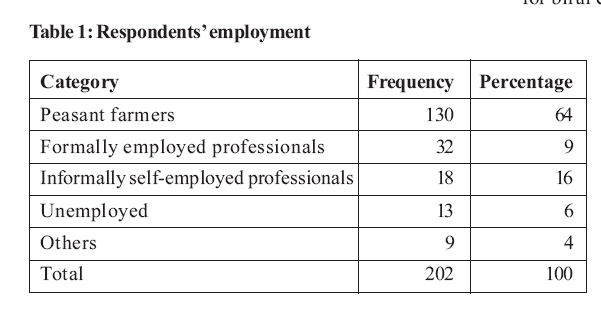
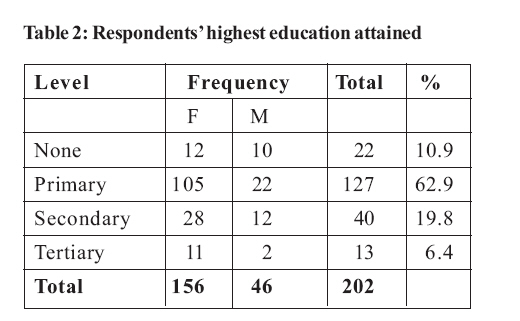
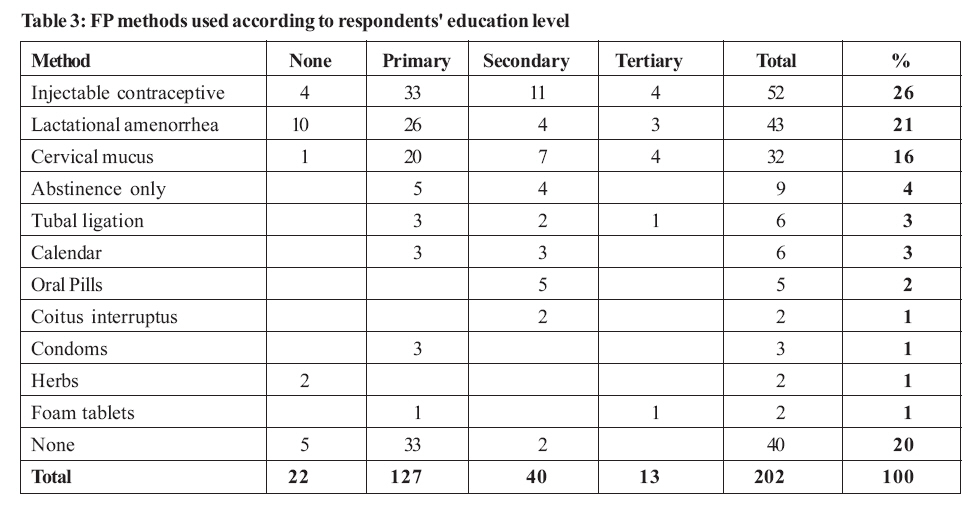
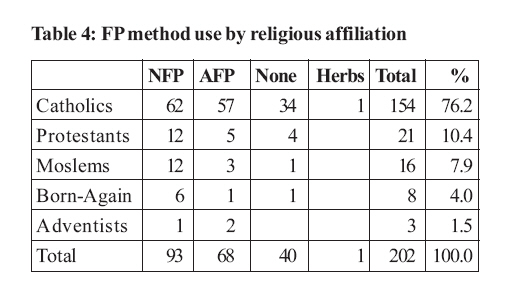
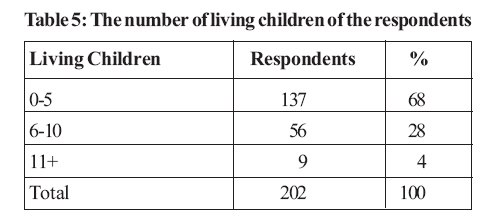
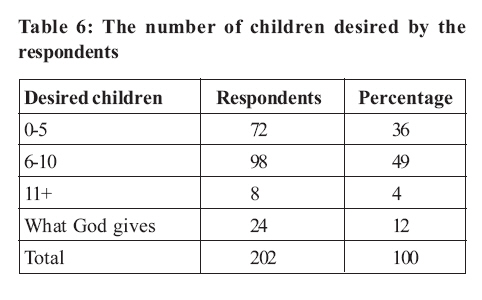
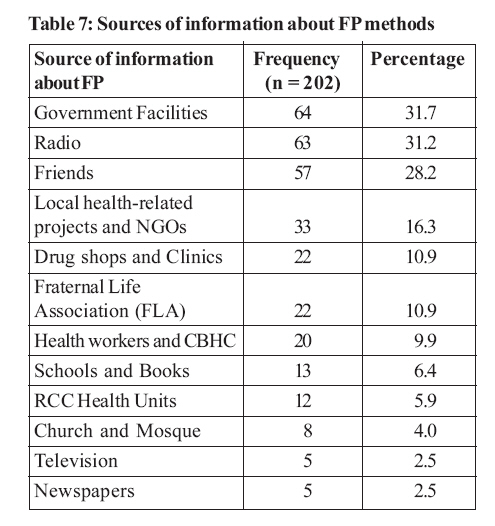
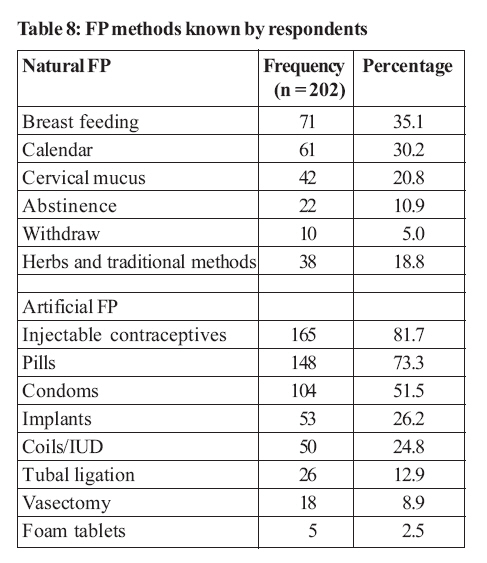
Of all RCC moral teaching, none is more disputed, misunderstood, and rejected than its persistent condemnation of contraceptives. In fact, not all Catholic teachers of faith and morals hold a similar position on contraception. Cardinal Lustinger of Paris and Bishop Jacques Gailot of Eureux, France, have ever supported the use of condoms against AIDS (Marx, 1996). Nuwagaba (2001) also wrote that even Ugandan Bishops are puzzled with the challenge of HIV/AIDS and the need for a manageable family. If the church's hierarchy is also divided on the issue, this probably hinders the efforts to provide natural FP methods in church facilities. Catholics in Ibanda Parish, Mbarara Archdiocese, reported using contraceptives without any feeling of guilt (Nuwagaba, 2001). In the same study, Catholic couples expressed the difficulty of using NFP methods because their husbands could not abstain from sex until the end of the fertile period. Women attributed this to alcohol consumption by the husbands. Other women claimed to have the highest sexual urge during the fertile period while others simply confessed ignorance of NFP methods. Most NFP teaching is expected to be given by priests during pre-marital counselling. However, in the same study, respondents also doubted priests as a source of reliable information on NFP methods since they are celibate (Nuwagaba, 2001). Cooke (1998) noted that today's world looks at each birth in economic terms without any measurement of the intangible benefits that accrue to parents, family, and society from the birth and raising of a child. Yet, the RCC calls upon Christian parents to examine their consciences constantly, to prevent materialistic and selfish values in decisions concerned with limiting their children (Steinbock, 2002). The RCC also approves the limitation of the number of children based on the mother's health, hereditary defects, low income, continued danger of unemployment, and lack of housing. It also considers the national needs conditioned by limited resources especially in less developed countries (Karl, 1985). In fact, Coleman (1997) noted that the RCC does not glorify uncontrolled procreation, nor praise any procreation of children without educating them. Rather, it encourages that Christian spouses have to harmonize matrimonial love, be open to procreation, properly care for their children and if necessary control their family size but with NFP methods. Given that the RCC recommends NFP, one would expect its leaders to be very knowledgeable on the matter. In America and Mexico, many Catholic priests were found to be un-informed about NFP or were actually informed by the laity that NFP methods do not work (Marie, 1998). Other priests blamed the doctors for not teaching NFP while the doctors wondered why the priests did not explain the church's teaching about NFP. Whereas the RCC strongly stands for NFP, little has been done to teach NFP methods to the potential or married couples. A study in Fort Portal, Uganda, indicated that most Catholic married couples were not instructed about NFP and instead privately consulted their friends who were using NFP (Nyarwa, 1993). NFP methods and HIV/AIDS Despite the HIV pandemic, the RCC has persistently promoted abstinence for unmarried people and faithfulness for married couples. Coleman, (1992) argues that the contraceptive mentality of separating sex from procreation leads to moral decay and increases the spread of HIV/AIDS since people indulge in sexual acts without worrying about pregnancy. Coleman also adds that if sexual intercourse leads to the spread of HIV/AIDS, spouses must be morally willing to limit the expression of their sexuality and also respect present or potential human life. Homeier (2005) argues that consistent abstinence is the only method that always prevents pregnancy and sexually transmitted disease. Couple relationship during use of NFP Methods For NFP to be effective, it requires the agreement and cooperation of both partners (Aguilar, 1998). Aguilar further notes that once sexual energies are stored and released at the appropriate time, the woman does not feel being used. A study in Kenya compared indices of couple relationship before and one year after beginning the use of NFP. Before the study, most of the women thought the purpose of sexual intercourse was producing children and releasing emotions. A year later, the primary purpose of sex was interpreted to be for personal friendship. Eventually, wives shared equally with their husbands in decisions concerning children education, family income, and expenditure (Kimani, 1986). In a study by WHO (2005), it was reported that FP and reproductive choices are supposed to be joint decisions within couples but that scant attention was given to couple-focused approaches in many African countries. The Uganda Demographic and Health Survey (UDHS) of 2000-2001 showed that only 57% of women had had extended FP discussions with their husbands and that 40% had never shared their FP ideas with their husband (UBOS and ORC Macro Int., 2001). This signifies existing important communication and empowerment gaps among couples, whose real impact is felt when they use NFP methods which require the partner's cooperation. Poor communication is also blamed for couple insecurity, which leads to failure of NFP methods. Some men fear that if their wives are left not pregnant for sometime, they might have sex with other men (Mbabazi, 2000) Factors affecting Utilization of FP methods According to WHO (1996), FP utilization may be influenced by the likely rate of effectiveness, least side effects, ability to take a pill everyday or insert a diaphragm before every sexual act, availability and cost of the method. A study in southern sub-Saharan Africa (SSSA) found that both government and non-government agencies educated the population about the various modern FP methods and free contraceptives were offered in almost every institution. However, Catholic institutions only counselled about natural FP methods (Rutenberg and Baek, 2004). In these units, clients found it difficult to ask health providers who were nuns, about other methods. In addition, HIV-discordant couples were not offered condoms. In Uganda, UDHS data of 2000-2001 showed that 3.5% of married couples did not use artificial FP because of religious reasons (UBOS and ORC Macro Int., 2001). Low use of modern contraceptives due to strong adherence to the Catholic faith was also reported in some parts of Uganda by Ayella (2005). Another factor with an effect on the use of family planning is the client's knowledge of reproductive physiology. In particular, NFP methods rely on a good knowledge of the menstrual cycle and its associated symptoms and signs. The UDHS 2000-2001 shows that whereas 96.4% of the respondents showed good knowledge about modern methods and 66.1% knew at least one natural FP method, only one third of the respondents knew the fertile period of the cycle correctly. Though the availability of new educational techniques has made it easier to train large numbers of couples in FP methods, including NFP, many married couples still lack this knowledge (Cooke, 1998). In a diocesan development program survey on NFP in the U.S, 60% expressed a religious motivation for NFP use although only a third of the couples had received clergy support (Boys, 1989).It is also now recognised that education level positively correlates with use of FP. In Uganda, 13% to 21% of women with primary school level of education used FP compared to 49% of those with secondary level education (UBOS and ORCMacro Int., 2001). Educated and employed women rely less on their children for economic security, so they tend to produce fewer children (Allan and Allen, 1990).They are also more likely to care for their children's health better, which contributes to the reduction of both infant and child mortality rates (Serunkuma, 2002). Therefore, increasing a woman's capacity to acquire education and employment has a powerful effect on her fertility. Availability of information, communication, and education about FP through health units, radio, television, books, and the internet could widen the accessibility of the knowledge of FP. In Pader District of Uganda, most health units did not have signposts, posters, leaflets, FP Books, policy documents on reproductive health (Ayella, 2005). The staff was inadequate in number and training. Sensitisation on FP, especially on NFP methods, was inadequate. Hubley (1993) emphasises that one-to-one communication is the most effective approach to use in FP counselling because it gives the counsellors the opportunity to clarify clients' misconceptions better. UDHS 2000 _ 2001 data showed that 86% of FP non-users had never discussed FP with health workers (UBOS and ORC Macro Int., 2001). Quality of NFP Services in Health Units Quality is an important factor in encouraging the utilisation of health services. Some elements of a service enhance client perception of quality. These include reliability, accessibility, communication, competence, infrastructures and process outcomes (Berry, 1985). The availability of qualified staff, reduced waiting time, and client satisfaction are also some of the indicators Uganda Catholic Medical Bureau (UCMB) uses to evaluate quality in hospitals within its network (Lochoro, 2003). For successful application of a NFP method, instructors need to teach clients for at least six sessions and make follow- up (McSweeney, 1992). Methodology The descriptive cross-sectional study was conducted in the area of Masaka Catholic Diocese, covering the districts of Masaka, Rakai and Sembabule. All the RCC health units in the dioceses formed the population. The two hospitals were selected purposively. Eight (or 31%) of the twenty six Lower level Health Units (LLHU) were selected proportionately after all the units were stratified by district and sampled on the basis of the proportion of the number of health units within the counties per district. From Masaka District, the two hospitals and three (3/12 or 25%) lower level health units were selected. From Rakai District, three (3/11 or 27%) lower level units were included and from Sembabule District, two units (2/3 or 67%) were included. The lower level units to be studied were selected conveniently on the basis of ease of access due to limited time. A total of 200 respondents were planned to be interviewed, i.e. 40 per hospital and 15 per lower level unit but in the end, 202 were actually interviewed. Interviews were held with clients on exit from the health units using interviewer-administered questionnaires. Systematic random sampling was used to interview every 5th client exiting. Key informants for the study, numbering 72, included the diocesan bishop, health coordinator, and the HIV/AIDS focal person, the managers of the selected health units, staff responsible for FP clinics in the selected health units, priests who are members of health unit management committees and NFP promoters in the diocese. The study tools were pre-tested in one of the units in the diocese excluded from the study. Qualitative data were collected and analysed manually and by computer using Microsoft Excel. Preliminary reports of the study were disseminated to the diocese through the diocesan health coordinator. One limitation was that some clients found it initially difficult to discuss reproductive health matters with the researcher, being a Catholic nun, until after lengthy explanation of the purpose of the study. This ate into valuable study time. Results The 202 respondents comprised 46 males (23%) and 156 (77%) females with a mean age of 31 years and none below 15 years of age. Their employment categories were as follows: The majority of the respondents were peasant farmers. Lack of paid employment may be an important factor in relation to reproductive behaviour and attitudes towards FP. Poor families tend to produce many children to provide labour, and are relied upon as security in old age. However, employed women may want to control their fertility in order to accommodate the demands of their work. The level of education has also been shown to influence attitudes towards the use of FP. The table below shows the highest education level attained by the respondents. The majority of the clients (63%) had only attained up to primary school level of education. In a FGD, many health workers stated that NFP methods require some formal education in order to count days and make daily recording of symptoms. However, an FGD of married Catholics in the Fraternal Life Association (FLA), argued that the cervical mucus method requires only the ability to feel, touch and see. According to them even illiterate people can use the cervical mucus method provided they are taught properly and they cooperate in marriage decisions. They referred to adult education as an opportunity to equip them with the skills necessary to access those FP methods that require ability to write. The majority of the clients (42%) used NFP methods for birth control, followed by those who did not make any attempts to control births. However, the most popular single method was injectable Depo Provera (depot medroxyprogesterone acetate) followed by breast-feeding. The most preferred method for respondents with no formal education was breast-feeding. Those with primary and tertiary education preferred Depo Provera while those with secondary education preferred the cervical mucus method. In terms of religious affiliation, Catholics were the majority by far (76.2% or 154/202). In all religious categories, the majority preferred NFP methods except for Seventh Day Adventists as shown below. The number of children living or desired might determine the choice of FP methods. The following tables summarise the respondents' desired number and actual living children. The majority of the respondents had less than 6 children, while a small number had more than 11. Overall, their average number of living children was 4.5. The average number of children desired by the 178 respondents who had made up their mind was 5.8. Those who had no specific desired number were 24 as shown in the table below. In an FGD with health workers, staff disclosed that mothers with the 12th pregnancy or more usually ask for permanent FP methods like tubal ligation irrespective of religion because they no longer desire any more children. In addition, clients with history of side effects of artificial FP methods e.g. prolonged or irregular menstruation periods or palpitations usually seek natural FP methods. Staff added that men recognize only condoms as a family planning method and reject vasectomy for fear of becoming impotent. Knowledge and Use of NFP methods The respondents were asked their sources of FP information to capture the likely sources of information about NFP methods. The following sources were cited: The most common sources of FP information were government health units, radio and through friends. RCC health units ranked very low in frequency as a source of FP information. Clients explained that health projects and NGOs such as World Vision, Rakai Health Sciences Programme and other NGOs teach them about FP methods but with much emphasis on artificial FP methods (AFP). AFP methods are available in most government health units and in most private clinics. This was true especially in Rakai District. Therefore, most people in those areas are likely to use artificial FP methods. During a FGD with staff, it was mentioned that marketers of AFP methods had identified their major side effects and can clearly explain to the clients which ones to expect, and how prevent and handle them. This had calmed many people's fears and promoted uptake of AFP. In clients' FGDs, members of Fraternal Life Association (FLA), a RCC-based organisation, explained that every year some of the Catholic couples attend the "Cana course" to renew their marriage relationship. So it is in this forum that they were introduced to NFP methods and they continued to meet in their various localities to discuss marriage and NFP methods. In all the ten FGDs held, only married Catholics from Kitovu, Makondo and Mbuye health units reported pre-marriage NFP education by lay leaders of married Catholics or by health workers. A Catholic priest, who is also a member of a health unit management committee (HUMC), admitted that pre-marriage NFP education was neglected in current marriage preparations. The respondents reported to know various FP methods as shown in Table 8. Most respondents had information about artificial FP methods than about natural FP methods. Of the NFP methods, most respondents knew breast-feeding and the calendar methods, while of the AFP methods, most knew about the injectable hormonal method, oral contraceptive pills and condoms. Herbal and traditional methods mentioned included drinking herbal potions, tying around their waist some herbs, a piece of the son-in-law's clothes, or a dried piece of the umbilical cord of the last child. The respondents were asked for the FP methods they use to space or limit childbirth. Table 9 shows the FP methods actually used. Most respondents used the injectable hormonal contraceptive, followed by lactational amenorrhea. Overall most people used natural FP methods (46% or 93/202 compared to 33% or 67/202 who use AFP methods). About 20% (or 40/202) did not use any FP method. The main reasons for this were religious (8% or 17/202), side effects (6 % or 13/202). Knowledge of the RCC Teaching on Family Planning by Catholic respondents Respondents who identified themselves as Catholic were asked whether they have ever had any teaching on Family Planning from any sources. About 50% (or 76/154) of them had ever heard about the teaching and ever received it, while 73/154 had only heard about it but had not received it. A few (5/154) had never heard about the RCC teaching on FP at all. In the various FGDs, many participants said that the RCC only discourages use of AFP methods but rarely teaches about NFP. Knowledge of the fertile period To assess the respondents' knowledge of the menstrual cycle, they were asked for the fertile period. According to the American Pregnancy Association (2005), the fertile period ranges from 10-14 days after the period. Only 7.4% of the respondents (or 15/202) knew the fertile period correctly. Attitudes towards Natural Family Planning Some respondents approved the use of artificial FP methods while others preferred natural FP methods. Those who preferred artificial FP methods gave poverty and HIV/AIDS as their main reasons. They argued that using NFP does not reduce the risk of producing children and yet they wanted to be very sure that they will not conceive. They argued that those who have used natural FP methods have ended up producing many children. They also reported that some of them have HIV infection and they did not want to produce infected children because it was very expensive to look after them and yet they were poor. Others reported that frequent pregnancies affect mothers' health more than artificial FP methods. Others argued that many families cannot afford the space for physical separation of the couple during the unsafe period. As a result, they use the same beds continuously and since the women's sexual urge increases during the fertile period, it is difficult for them to exercise abstinence. In an FGD for male clients, one member revealed that some husbands keep their wives away from other men by frequent pregnancies. In an FGD for female clients, one member revealed that the fact men want their wives to stay pregnant is one of the reasons why many women prefer to use artificial FP methods, because it is possible to use them secretly without the knowledge and cooperation of their husbands. In regard to HIV/AIDS, a key informant said:
Respondents who Use the NFP Methods Proponents of NFP methods said, they do not have side effects or continuous costs and that they increase love and cooperation between couples. Some FGD members stated that ever since they started practicing NFP methods, they enjoy sexual intercourse more than before and their husbands first ask whether it is safe to have sexual intercourse. This had increased opportunities for communication in their marriages. One key informant said:
Catholic Respondents and Use of AFP Methods Catholic respondents were asked whether they use artificial FP methods. Most of them 44% (68/154) agreed that they use artificial FP, while 33% (51/154) denied its use and 23% (35/154) were non-committal. One of the proponents even argued that God blessed the AFP methods by giving scientists the wisdom to make them. Providers' perceptions of barriers to use of NFP methods The health workers reported that the common reasons for low use of NFP methods were clients' inconsistency with guidelines, HIV/AIDS, lack of knowledge, doubt over the effectiveness of the NFP methods. Staff argued that most pregnant women do not remember their last menstrual period, and that NFP methods are impossible for peasant couples who live together continuously. High parity was also pointed out as a factor, given that mothers with over 12 children find it difficult to grasp NFP techniques. Effectiveness of NFP methods reported by Clients In several clients' FGDs, there were mothers who said that breast-feeding for between one and two years had effectively protected them from pregnancy while others said that they had ever conceived within less than six months after delivery despite exclusive breast-feeding. Regarding the mucus method, members of FLA praised its effectiveness provided the partner is cooperative. However, some women said that NFP methods are hard to use consistently because it is at the time of ovulation that they most desire to have sexual intercourse. For their part, many health workers reported that NFP methods would be effective but men do not always accept to abstain from sexual intercourse, even if it is during the fertile period. Quality of NFP services in health units The provision of NFP in the health units was assessed by use of several key elements of a quality service. Table 10 shows the results. The findings above show that NFP is not a priority service in most health units studied, and that even where it is provided, the service is of poor quality. Most health workers provide health education on NFP and stop there. There is poor record-keeping and follow up of the NFP clients. Staff has not been trained in NFP counselling and provision. They do not feel confident enough to assist clients and some of them still think that any FP method is artificial and thus forbidden by the RCC. Only a small minority of staff had referred clients who wanted artificial FP methods to Government health units and clinics. Discussion Utilization of the Family Planning methods In the sample studied, NFP users were more than AFP users, while breastfeeding and injectable hormonal contraceptives were the most used FP methods. These findings are consistent with the national picture of access to FP services. Before the advent of HIV/AIDS, every mother was expected to breastfeed her baby for a certain period. In the process some women were protected from conception. However, the presence of HIV has made it inadvisable for HIV-positive mothers to breastfeed. The contraceptive benefit of breastfeeding has therefore also been lost. This therefore has negative implications for the efforts of health services to prevent vertical transmission since the mothers are likely to conceive again. Among the AFP methods, the injectable contraceptive method was the most used. In general, artificial FP methods have been widely marketed as convenient, effective and safe, and the required commodities made widely available through social marketing. Condoms and oral contraceptive pills are available in many shops, even though there are frequent stock-outs of the same in public health facilities. The injectable contraceptive hormone is the most preferred method partly because of the secrecy and convenience it affords the women. They do not have to take in the presence of their husbands, and therefore it allows the women to exercise their right to decide, without undue pressure or lack of cooperation from the husband, when or whether to have children or not. In addition, there is little risk of forgetting to take it since it is given once every three months, and administered by a qualified health worker. This gives it a lot of advantages compared to all the other methods whether natural or artificial. This is the rights-based approach that the Ugandan Ministry of Health is using to empower women. Moreover, the injectable method is also very effective. In addition, given the low literacy level especially among women, their commonly weak domestic position in making decisions over child-bearing and weak economic power, the injectable hormone is a very opportune method for them. Other artificial methods like oral pills, spermicides and condoms require overt actions that require the acceptance and cooperation of the partners. This also applies to NFP methods, which require a lot of understanding and cooperation from the partner. Although RCC teaching emphasises that understanding, cooperation and self-restraint are virtues to be cultivated in marriage, the situation of the couples on the ground is quite difficult. Since RCC discipline is tolerant to alcohol consumption and yet one of the major reasons expressed by the respondents in the study is that when the husbands are drunk, they will not listen to any plea to wait for the safe period, even RCC adherents find it difficult to respect the teaching of their own church. In a way, therefore, RCC discipline unknowingly facilitates the perception of inappropriateness of NFP methods for the target population of the rural poor. Education level, Employment and Family planning Formal education is known to delay the marriage age and the commencement of childbearing. In addition, employed women tend to control their fertility in order to accommodate their work demands. As a result, educated and employed women are more likely to have fewer children in their reproductive life than their uneducated and unemployed counterparts. This study shows that the majority of the respondents had attained only up to primary school level of education. Although this is sufficient to expose them to lessons on reproductive health, it is insufficient to increase their demand for reproductive health services. It is also certainly insufficient to keep them in school long enough to delay pregnancy and increase their chances of formal employment which would force them to regulate their fertility. For example, the majority of the respondents had an average of 4.5 children, although they desired 5.8. Moreover, the Uganda government target is 5.4 children (MOH, 2005), all of which are higher than the world average of 3.1 children (Cohen, 1995). Although their desires are higher than the global average, no respondent mentioned the need to have many children for domestic or farm labour. This seems to refute what Allan and Allen (1996) wrote that high population was desired because it promoted agriculture, military and political power. On the contrary, the mainly rural women in this study mentioned that families with many children could not afford the high education needed to compete for important societal positions. This also implies that despite conflicting positions on population at the national level in Uganda, economic reality has started compelling individual families to space and limit their children, with the increasing view that an additional child is a burdensome blessing. However Cooke (1998) points out that this interpretation of births in economic terms excludes the intangible benefits that accrue to parents, family, and society from the extra children. Poverty and physiology also make NFP methods difficult to use. Many couples cannot afford the space for physical separation of the couple during the unsafe period and due to physical proximity end up having sex. In a separate study, Nampala (2006) says that sex is regarded as the only affordable form of entertainment for the poor. Coupled with alcohol, the reproduction process seems unstoppable unless interventions which can take the prevailing conditions into consideration are put in place. In this study, although clients acknowledged the side effects of using artificial FP methods, they argued that the risk of illness, death and economical consequences resulting from an additional pregnancy are much greater than those due to use of artificial FP. This shows their determination to control their fertility and indicates that there is a degree of unmet need as far as FP methods acceptable to their religion are concerned. Religion, Marital Status and FP Methods Use Even before Humanae vitae, the teaching of the RCC on FP was controversial. It is therefore not surprising that despite Humanae vitae, many RCC religious leaders do not strongly advocate for NFP. One would have expected them to be the very knowledgeable champions of the teaching and to use any appropriate occasion such as marriage preparation and wedding days to further the teaching. This study shows that priests did not give the expected teaching to the intending couples. In fact, many respondents had never heard about the official position of the RCC on FP and several religious leaders and health workers did not feel confident enough to explain the position and NFP to the clients. In a few cases, priests invited health workers to conduct the prenuptial teaching on NFP on their behalf, yet only two health workers had been trained to do so in the whole diocese. This is consistent with the findings by Nuwagaba (2001) in which 80% of Catholic couples were using artificial FP methods. Knowledge of NFP Methods by the Clients Individuals who are informed about the options of FP may develop a rational approach in planning their family. The RCC health units were among the least common sources for FP information. It is not surprising, therefore, that most respondents knew artificial FP methods and very few knew natural FP methods. The would be main source of natural FP information (the RCC health units and system) is not well prepared, equipped, staffed, facilitated and motivated to deliver the information to their clientele. Successful use of any NFP method depends primarily on proper detection of fertile and infertile phases of menstrual cycles (Dicker et al., 1989). In this study, correct knowledge of the fertile period was lacking among the majority of the respondents. In fact, earlier UDHS (2000-2001) data showed that only 18% of women correctly knew their fertile period. Cooke had also found that despite new educational techniques to train large numbers of couples in NFP methods, many married couples still lacked the knowledge of NFP (Cooke, 1998). Nyarwa (1993) had also noted that Catholic married couples in Fort Portal were not instructed about NFP, but instead, they individually consulted their friends who were using NFP. The failure of the majority of respondents to predict the most likely fertile period definitely indicates a low level of knowledge of NFP methods and is an indictment about the quality of training and health education. Perception towards Natural Family Planning Although the majority of the respondents expressed the desire to space or limit children citing poverty, high educational costs and HIV/AIDS, they also mentioned the complexity of the NFP methods as a significant barrier. Many respondents in this study, irrespective of their religious affiliation, use artificial FP methods despite knowing their adverse or side effects. This implies they have a high demand for FP services which is unmet, partly because they are challenged by the complexity of some of the methods. This is a specific challenge to the promoters of natural FP methods because they need good knowledge of the menstrual cycle. For the promoters of NFP, the negative attitudes held by the respondents against some of the artificial FP methods, especially condoms and oral contraceptive pills, should serve as a window of opportunity and an entry point for health education on NFP. Although the RCC teaches that sexual abstinence during the fertile period is a manifestation of self-sacrifice and love for the partner, this view was not felt strongly among the respondents. The findings also indicated that some Catholics had no idea of the RCC teaching about contraceptives use. In fact, some praised God for the wisdom granted to scientists to make contraceptives, while others used contraceptives in the hope of being forgiven their sins. This suggests that the health education on FP that takes place in RCC health facilities lacks the theological and spiritual aspects that the RCC would like to see imparted in its adherents. This could be due to the lack of a strong chaplaincy function in most RCC health facilities. Such a function could complement the efforts of the health workers by giving the clients the official position of the RCC on FP matters. Although in this study the respondents insinuated lack of trust in priests as sources of credible information on FP matters, their credibility as sources of the official RCC positions cannot be doubted. It has been shown that natural FP relies heavily on partner cooperation. However, this declines when one or both partners abuse alcohol. This study also shows that alcohol use is common among the spouses of the respondents. The RCC position of tolerating "reasonable" consumption of alcohol sets ground for alcohol abuse and hence failure of use of natural FP methods. This is also possibly responsible for the high use of artificial FP methods by Catholics. Similar obstacles such as lack of partner collaboration due to alcohol, attitudes, gender perceptions and lack of knowledge have been found in this study as the case was in Ibanda (Nuwagaba, 2001). Health workers felt the main obstacles to the use of natural FP methods to be lack of knowledge, inconsistency with guidelines and high failure rates of NFP methods. Their perceptions have strong implications for the uptake since they are the providers. Any efforts by the RCC to increase the uptake of the natural FP methods must therefore involve training the health workers and providing them with the knowledge, skills, facilities and support to enable them to get convinced and confident to provide the methods. This also involves providing them with the necessary technical evidence of the effectiveness of natural FP methods, in order to match the volume and quality of available information about artificial FP. Health workers and chaplains need to collaborate on the issue. St. Marie (1998) noted that often, the church tends to blame health workers for not teaching NFP methods while the health workers also blame the church for not adequately expounding its position to all its faithful. In this study, only one health unit reported pre-marriage NFP induction by the religious. This implies that the majority of married Catholic couples, who are the potential users of NFP, did not have official induction yet, in the U.S., the majority of NFP users cite a religious motivation and a third had received the support of the clergy (Boys, 1989). Effectiveness of NFP Methods Reported by Respondents Effectiveness of an FP method is a major determinant of its use. The study shows that the majority of the respondents were using natural FP methods, although they did not have much information about their effectiveness. Hatcher et al (1997) estimated more than 20% of method failures occur due to method misunderstanding, inadequate teaching, or failure to abide with guidelines. This highlights the need for RCC health facilities to ensure that clients are taught very well. Quality of NFP Services in Health Units Only one half of the units studied provided FP education. However, they were not adequately staffed and facilitated to provide FP services of good quality. McSweeney (1992) recommends that for effective learning of natural FP methods by clients with low education, instructors have to teach them for not less than six sessions and make follow- up supervision. This study shows that these rigorous requirements were not followed in the study area. Insufficient staffing precluded this rigorous teaching. Poor record keeping made client follow-up difficult. The national Health Management Information System (HMIS) also provides for only artificial FP methods. Therefore, there is a systematic lack of useful information for planning and decision-making regarding natural FP. Lack of reference materials for staff, teaching AIDS such as posters, leaflets and books also casts doubt on the quality of information given, where natural FP is provided. This is similar to what Ayella observed in Pader District of northern Uganda (2005). Conclusions While Uganda's population is rising at a very fast rate and government population control strategies focus on the use of artificial family planning methods, the Roman Catholic Church (RCC) insists on the use of natural family planning methods on moral and value grounds. However, the study has shown that even in the most Catholic-inhabited areas, the church does not come out strongly to initiate, support and facilitate the use of natural family planning. It has also shown that clients would be willing to adopt natural FP methods more if evidence of their effectiveness can be provided, to the level currently used by the marketers of artificial FP methods. The study reveals that the key factors that influence uptake of natural FP methods include support from the church, presence of health workers trained in natural FP methods, support follow-up from health workers and fellow users, partner collaboration and education status. The study also shows that the knowledge of NFP methods among health workers, the religious leaders and the clients was deficient, and that the health units are not adequately staffed and equipped to provide NFP methods. Recommendations As the sole champions of natural family planning, the local leaders of the Roman Catholic Church need to design strategies to ensure their adherents use the approach. Such strategies could include overt acceptance that family planning is important for social and economic reasons, especially in a developing country with a fast population growth rate like Uganda; reviving the RCC teaching on natural family planning; revival of the production of contemporary and up-to-date guidelines on natural family planning for religious leaders and health workers in RCC health facilities; giving political support to natural family planning through public teaching by the top leaders of the church, and through the appointment of chaplains trained in natural FP to the health facilities; and monitoring the utilisation of natural family planning by the adherents of the church. Other policy makers within the RCC health services such as diocesan health coordinators and the Uganda Catholic Medical Bureau need to implement the appropriate monitoring and evaluation strategies for natural family planning within the RCC facilities e.g. through the HMIS. They also need to incorporate natural family planning as an integral function of the health facilities, rather than the current parallel arrangements such as the Family Life programme. They need to plan for and provide training in natural family planning methods to health workers, teachers, priests (especially parish priests and chaplains) and other religious leaders, as well as peer support groups of natural FP user couples. They need to design a communication strategy to spread the teaching on natural FP in order to counter the negative publicity and to promote natural FP. Such a strategy could involve the use of mass media (print and electronic) as well as open dialogue and individual couple approach. This would be done in various languages including local ones for each area. Existing volunteer resource groups like Maternal Life Uganda and Fraternal Life Association could be supported to expand their activities to various places. The managers of the health facilities need to ensure that the quality of family planning services is assured through continuous medical education (CME), update of the evidence on the effectiveness of natural FP, regular research on natural FP and provision of the required supplies for natural FP education and monitoring. They need to budget for and allocate resources for NFP activities and provide staffing and suitable space for the activity. For its part, the Ministry of Health needs to be open about Family Planning, and allow room for natural family planning to flourish as well, through including it in the HMIS reports and supervising its utilisation as a complementary but integral activity to the population control and reproductive health rights activities. References
© Copyright 2008 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp08016t6.jpg] [hp08016t10.jpg] [hp08016t5.jpg] [hp08016t9.jpg] [hp08016t8.jpg] [hp08016t7.jpg] [hp08016t1.jpg] [hp08016t3.jpg] [hp08016t2.jpg] [hp08016t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}