 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
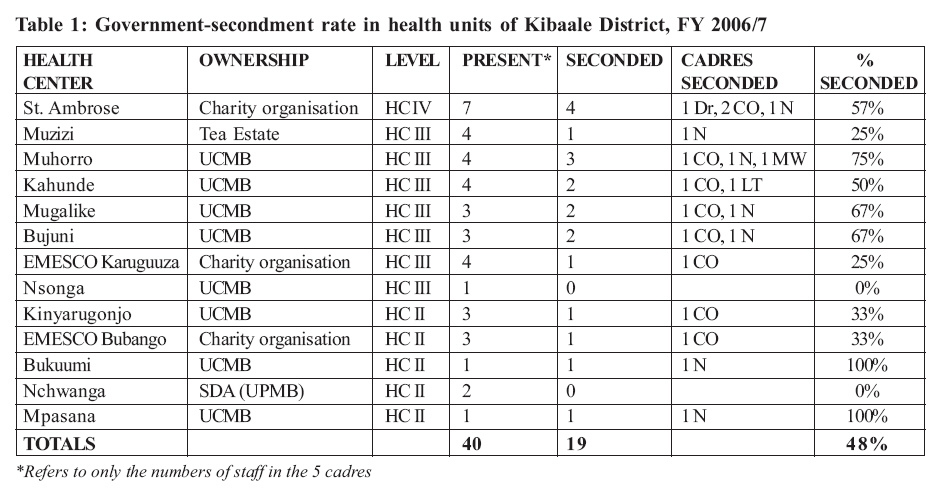
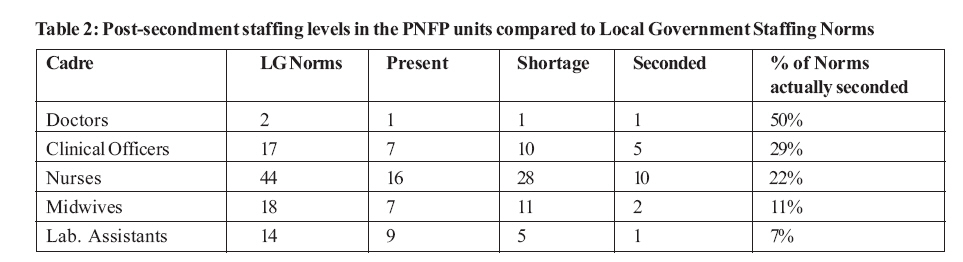
Health Policy and Development Journal, Vol. 6, No. 3, December, 2008, pp. 142-152 THEME TWO: HUMAN RESOURCES FOR HEALTH The challenges of managing government-seconded health workers in private not-for-profit health facilities of Kibaale District, Uganda Peter Barugahara*, Everd Maniple# and John Francis Mugisha# * Corresponding author. Hoima Diocese, P. O. Box 34 Hoima, Uganda Code Number: hp08017 Abstract Private health care providers are an important component of pluralistic national health systems. In Uganda, the public-private partnership for health (PPPH) has led to the government assisting the private health sector in various ways, in recognition of and support to their work. Apart from financial assistance, the government deploys civil servants to work in private-not-for-profit (PNFP) health facilities. Such government-seconded health workers are recruited, deployed and paid by the government but they work under the management of the PNFP health units. In the rural and remote district of Kibaale in mid-western Uganda, government-seconded health workers form 48% of the key professional staff in PNFP health services. However, government secondment raises a number of important managerial and human resource challenges. PNFP health care managers have some workers over whom they do not have full authority and control. The seconded workers have to serve two authorities and satisfy them equally. This cross-sectional descriptive study aimed at identifying the problems arising from this kind of relationship in a district where PNFP health units are heavily dependent on government-seconded personnel, and how such problems may be addressed.It was found that there is unequal treatment of seconded and non-seconded staff, with the former receiving better pay, and having more professional management than the latter. However, they felt there was too much workload in PNFP units compared to government and were not comfortable with the PNFP prohibition of private practice. In addition, they felt that they were not trusted by the PNFP managers and that they had limited or no opportunities for career development and further studies. PNFP managers felt they had no control over seconded staff and felt that they have no possibility to participate in the selection of staff to be seconded to their units. As a result, seconded staff were perceived to have no commitment to work in PNFP units, and to be prone to absenteeism, illegal private practice, demand for big financial allowances, abrupt attrition and pilferage of health care supplies. This paper proposes quick enactment of the PPPH policy to define the relationship between the public and the private sectors. It also proposes that the government gives unconditional funding to the PNFP facilities on a contractual basis, and only demands for accountability on agreed outputs. This would facilitate the PNFP managers to recruit their own staff and endeavour to attain the agreed outputs. Introduction The Ugandan health system is a typical pluralistic system comprising the public government-owned and managed health service; the mainly faith-based facility and non-facility based private-not-for-profit (PNFP) services; the independent individual or group-owned and managed private health providers; and the traditional and complementary medicine practitioners. The faith-based PNFPs are internally sub-grouped under three umbrella organizations viz. the Uganda Catholic Medical Bureau (UCMB) for those founded by the Roman Catholic church (RCC), the Uganda Protestant Medical Bureau (UPMB) for all those founded by the non-RCC Christian churches and the Uganda Muslim Medical Bureau (UMMB) for those founded under the Islamic faith (UCMB, UPMB and UMMB, 2007). The three bureaux together represent 78% of the 490 PNFP health units while the rest fall under other humanitarian and community-based healthcare organizations (MOH Uganda, 2005). Faith-based healthcare services were the first health services in the country and were mainly initiated by religious missionaries at the end of the 19th century. Right from their inception, however, there has always been a form of collaboration between the private providers and the government, with the latter recognizing the pioneering efforts and contribution of the former (MOH Uganda, 2001). Later the Government of Uganda itself started its own health system with hospitals and health centers all over the country. Government facilities were usually located in urban centres or near administrative offices while PNFP services were mainly located in remote, hard-to-reach areas. The two subsystems operated in a complementary manner, side by side without competition. In fact, in 1955, the government created the UPMB in order to assist in channeling government financial assistance to lower level health units. The UCMB was created in 1956 and the UMMB in 1999. During the politically and economically difficult years of the 1970s and the first half of the 1980s, government health services virtually collapsed and stopped operating as a system. The PNFP health services managed to survive largely due to external support. In fact, it is during this time that many of the lower level PNFP health units were started in rural areas to fill the gap in services. At national level, whereas the national medicine purchase and distribution mechanisms had collapsed in the 1970s, the UPMB and UCMB came together to create the Joint Medical Store (JMS), a central pharmacy to ensure constant supply of medicines and supplies for their services. Not only did PNFP services survive the turmoil, they also became the main backbone of health care services with a good, reliable and predictable level of quality. It is only in the late 1980s after change of government that efforts to reconstruct the government health system started. Beginning with 1990s, the PNFP health facilities began experiencing serious financial problems due to dwindling external assistance (UCMB, 2001). Many source countries for their financial assistance changed their preferred modes of international aid. Some countries preferred to adopt the sector-wide approach (SWAp) and others preferred large multi-sectoral international NGOs. With SWAp, projects that used to sponsor individual programs in PNFP health facilities were all directed into one national purse thus decreasing funds for the PNFP sector. Some PNFP facilities tried to cope by generating revenue locally through increasing user fees. However, this became a significant barrier especially to the poor and compromised the PNFP mission. In 1996, the PNFP health facilities declared to Government their inability to survive for long in the prevailing circumstances and entered into serious negotiations for official public-private collaboration in 1997. The official Public-Private Partnership for Health (PPPH) started in July 2000 (MOH, 2005b). This collaboration takes various forms: the government contributes funds for operational costs, medicines and personnel to PNFP facilities. The funds are channeled through the districts and the medicines are channeled through the Joint Medical Store. Personnel are seconded to the PNFP facilities by the government, through the District Service Commission. Since healthcare is a labor intensive industry with about 60-70% of the health expenditure going to personnel, the assistance with seconded staff is highly appreciated by the PNFP managers. For their part, the PNFP health services head some sub-districts, and participate in the government's priority health programs such as implementation of the Uganda National Minimum Health care Package (UNMHCP). In addition, they supervise lower level health units in their area and participate in planning, budgeting, accounting, reporting, monitoring and evaluation of all health activities in the districts. To fulfill these duties, they depend either on their own staff or government-seconded staff. Under the secondment arrangement, the staff is recruited, paid and supervised by the government, but is deployed at a PNFP health unit. In doing this government aims for effective coordination of efforts among all partners in order to increase efficiency in resource allocation and to attain equity in the distribution of available resources for health and effective access by all Ugandans to essential health care. The effect of secondment is most felt especially in rural areas such as Kibaale District which have a severe shortage of qualified health workers. Seconded staff receive their full salary from the government are generally willing to work at PNFP units under that arrangement. However, this comes not without challenges for the PNFP managers. Since the local government is responsible for their recruitment, deployment and payment, it is also capable of transferring the seconded personnel. Governing, controlling, daily supervision and discipline lies on the shoulders of PNFP managers. Often, seconded staff demands extra incentives directly from their PNFP employers before they accept secondment. Such incentives include housing, monthly financial allowances and scholarships. The incentives are a high cost to the PNFP services, and may exceed the value of government contribution. Such staff, therefore, has a challenge of dual allegiance. For their part, PNFP owners and managers do not participate in the selection of the seconded staff. Since they also do not pay their salaries, control becomes a challenge. Some seconded staff has shown serious lack of commitment to their health units of secondment. As a result, the utility of seconded staff has become a matter of serious debate in Ugandan health policy circles. Whereas observers agree that there is still strong justification for government assistance to the PNFPs, when it comes to personnel, the focus of the debate currently is on whether staff should be physically seconded or another approach should be adopted. The advantage of government assistance needs to be consolidated and maximized in order to have a well paid and highly motivated and responsible medical staff which is a prerequisite for an efficient and effective health service system (Kisubi and Mugaju, 1999). Most Ugandan PNFP health facilities have a different work environment and ethic from that found in the government facilities. Often, there is direct and obvious supervision and control from the PNFP managers, private practice is often prohibited, there is no pension scheme and the workload is often heavy. As a result, many government-seconded personnel face problems in PNFP units, especially when their motivation is questioned and they usually have poor interpersonal relationships with the founders. Study area The study was conducted in Kibaale District, located in the mid-western part of Uganda. It is a rural and remote area of the country with difficulties in attracting health workers due to remoteness. Due to this, most of the PNFP facilities in Kibaale District have got health personnel seconded by the District Local Government as part of the PPPH. Problem statement: While government secondment of personnel to PNFP health facilities spares them the hassle of looking for funds to pay them, it also poses several problems to the PNFP managers. The seconded staff serves under various authorities with conflict in allegiance, with the result that they are under no direct control on any one of them. This affects their motivation and performance and breeds conflict with, especially, the PNFP managers who supervise them on a day to day basis. Moreover, the demand by the seconded staff for extra incentives from the PNFP managers creates challenges of equity with PNFP-recruited staff of similar cadres, who do not get the government salaries. Study objectives The study had five objectives i.e. to determine the number and skill mix of government-seconded staff in PNFP health facilities of Kibaale District; to compare conditions of service and terms of employment for government-seconded and non-seconded staff; to assess the perceptions of the government-seconded staff about working with PNFP health facilities; to establish challenges faced by PNFP managers in managing government-seconded staff; and to propose next steps to improve the benefits of government secondment of health workers. Literature Review The Number, Distribution and skill-mix of Health Workers Human resources for health (HRH) in much of the developing world, particularly in sub-Saharan Africa, are inadequate and poorly distributed. Other HRH challenges include skill mix imbalances, mismatch between supply and demand, high mobility across local, national, regional, and international borders (Narasimhan et al., 2004). These challenges pose a serious obstacle to the achievement of the MDGs and to the improvement of the overall health of the poor in Sub-Saharan Africa. Imbalances in the geographical distribution of health workers aggravate the health personnel crisis. Given that the human resource of an organization is its most valuable asset, improvement of the human resource situation should lead to the overall improvement of the entire organization. The number of trained health workers in Africa has historically been inadequate, but in recent years, many countries have suffered from serious scarcities of almost all cadres (USAID, 2003). The expansion of the health-facility network in many African countries has been done in an uncoordinated way, such that the construction and refurbishment of health facilities has not matched with the ability of the national health system to staff and maintain them on a sustainable basis. In Uganda, the recent program to set up health centers at every parish was not followed by increased production and recruitment of health staff to fill them. Thus in countries like Malawi, Zambia and Uganda, there are many standing health centers which are not staffed or understaffed. Therefore, patients' access to functional health services continues to be difficult. To circumvent the problem of staff shortage, some countries have opted to use substitute cadres for duties that were the traditional domain of other more highly qualified professional cadres. Of recent, this task-shifting approach has even received WHO backing (WHO, 2007). Terms of employment and conditions of service for health workers There is need for incentives to retain and motivate health workers, and especially attract them to hard-to-reach areas (Lincoln et al., 2004). One of these is setting up of favorable terms of employment and conditions of service. These include adequate supplies of equipment, medicines and sundries. However, for staff to use these inputs efficiently, they must be motivated, skilled, and supported. For favorable conditions on working hours, workload, leave and rest to be granted, there must be enough health workers on the roster to release the pressure on the existing cadres created by heavy workloads. Increasing salaries is one way of improving the terms and conditions of service for health workers. Even amidst problems being faced, a number of low income countries have dramatically increased the pay of public health workers in recent years. In the United Republic of Tanzania, for example, the Selective Accelerated Salary Enhancement scheme provided an opportunity for ministries to raise levels of remuneration for high priority groups. In Uganda, salaries were increased in 2004 for all health workers following a job evaluation exercise across the whole public service (WHO, 2006). In addition, health workers need to be provided with accommodation facilities which have clean water, adequate lighting and heating, as well as providing vehicles, medicines, working equipment and other supplies (WHO, 2006). The push factors which force people to migrate must be mitigated in the conditions of service offered. In search of a better livelihood, health workers are moving within countries from rural to urban areas; within regions from poorer to better-off countries and across continents (WHO, 2006). Health workers in poor countries, regions and areas need to be assured of promotion and career development prospects for better remuneration, upgrading qualifications, gaining experience, transport, a safer environment and education of family members; and to be relieved of the heavy workload (WHO, 2006). If this were done, even remote areas like Kibaale would be assured of qualified health workers. Other incentives such as affordable child care, financial support or children, and provision of leave adapted to family needs can encourage entry into the workforce, especially nursing. Perceptions about public-private partnership It is noted that the Public-Private Partnership for Health (PPPH) at district level has not yet taken off in parts of Uganda. Many stakeholders see it with a lot of pessimism and with no foreseen benefits. In addition, there is still a lack of appropriate organizational structures to give the driving force to the partnership. Some government officials do not see the need for collaboration between PNFP health facilities and government. They see the problems of PNFP health facilities as belonging to them alone. Others even look at the current financial assistance given to PNFP health facilities as wastage of resources. On the other hand, some PNFP stakeholders view the partnership with suspicion and fear that it could lead to compromise of identity, mission, independence and quality of service (UCMB, 2001). Government secondment of health workers to PNFP health units is an endeavour to work together with the private sector to improve the performance of the health system in general (Lochoro et al., 2006). In the partnership, PNFP units provide a significant resource input and health care outputs. They have a network of hospitals and health centers accounting for 42% of the 99 hospitals, and 28% of the 1,617 lower level units in the country with a considerable percentage of these units located in rural areas. They combine provision of healthcare and training of health workers and own 19 of the 27 health training institutions (HTI). In fact, they are a more efficient point of investment compared to public services (UCMB, UPMB and UMMB, 2007). The PNFP health sector brings complementarity, non-duplication and non-competition to the partnership. Therefore, allocation of resources to the PNFP increases the efficiency of resource allocation, while at the same time achieving equity in the distribution of available resources. Among all these health providers, the leadership in Kibaale district chose to second health workers only to Facility-based PNFP services because they, too, are of public interest and have a concern closer to that of government i.e. the welfare of the population. The benefits of public-private partnership for health, on the whole, and of the government secondment of staff in particular, can be seen in terms of equity, access, efficiency, quality and sustainability of health care. The most vulnerable groups in society are given financial and geographical access to health facilities with good quality health care. Financial assistance to the PNFP has actually led to significant reduction of user fees (Guisti et al., 2004). Within their networks, PNFP units have established mechanisms to strive for better quality, through establishing minimum standards and internal self-regulation (Lochoro et al., 2006). The quality of care provided by PNFP units has progressively improved, as evidenced by the increased number of health facilities with qualified health staff. This has largely been due to better payment of staff, made possible by government subsidies and secondment of health workers. It is also assumed that since the majority of PNFP health facilities are found in the rural areas, the secondment of health workers to PNFP health facilities has addressed the equity concerns of health care as 85 percent of the poor reside in rural settings (Lochoro et al., 2006). The shift in the allocation of resources from hospitals towards lower level health centers seems also to address the issue of equity and efficiency (Ssengooba et al., 2006). Other benefits that have accrued from the cooperation between the PNFP and the government sectors include joint policy formulation and development, planning, resource mobilization for health, the joint training, joint deployment and management of the human resources, joint monitoring, reporting and evaluation of health care outputs as well as the management of health care delivery especially at the Health Sub-District level (Lochoro et al., 2006). As noted by several authors, there are numerous challenges that come with government secondment of health workers to the private sector. At the district level, there is still mutual suspicion and a spirit of competition with the PNFP health facilities. Subsequent unilateral salary increases by the government in response to industrial action has created serious imbalances in pay and led to staff attrition from the PNFP (Onzubo, 2007). Currently, the human resource constraint is probably the biggest test for the success of the partnership (Lochoro et al., 2006). One of the reasons why health workers do not lie to work in or leave the PNFP services is the prohibition on dual practice. In government, health workers often do private work, especially in private clinics and use other coping strategies to supplement their salary (McPake et al., 2000; Van Lerberghe et al., 2002; Berman and Cuizon, 2004). The Ugandan HRH Policy suggests that all registered health workers should be allowed and even encouraged to do private practice, subject to licensing, registration and regulation (MOH Uganda, 2006). However, the policy recommends that private work should only be undertaken after working hours, and that this should be registered and declared (MOH Uganda 2006). There are a number of challenges associated with this practice: health workers may be tempted to make services poor in public setting and refer patients to their private clinics where the charges could be too high for the poor; given poor supervision, they may also use publicly-paid for inputs such as time, medicines and equipment for private practice. In fact it is argued that private practice undermines the very spirit of public health care delivery by charging fee-for-service thus encouraging provider_induced demand (Berman and Cuizon, 2004). In addition, regulation and licensing are impossible especially in rural areas, and that private practice by public health workers would result in absenteeism and corruption (Berman and Cuizon, 2004). Another challenge regarding the public-private partnership concerns salaries. Often, seconded staff receives better pay than their equivalent counterparts in the same institution who are directly recruited by the PNFP units. This creates equity problems in the institutions. This was noted by Van Lerbeghe and Ferrinho (2000) and by WHO (2006). Accompanied by the possibility to do private practice, these incentives put a seconded health worker well above the earnings of a similar worker recruited directly by the PNFP unit. Doctors in Portuguese-speaking Africa could earn the equivalent of one month's salary within one to seven hours of private practice (Ferrinho et al. 2000). Since medical practice can only be lucrative where there is a reasonable population density and adequate disposable income, health personnel would continue to want to be posted in urban rather than rural areas. This therefore makes attraction of health workers to rural areas very difficult and to rural PNFP health units even more difficult. Policies on management of health workers Government secondment of health staff to PNFPs in Uganda did not start recently with the public-private partnership policy. It has been around since the 1970s, when the government started working with the PNFP sector as partners in health in a spirit of cooperation, complementarity and mutual support for a better and efficient provision of health services to the population. Currently, this is implemented through the districts, whereby health workers to be recruited are all interviewed by the decentralized District Service Commission. Their salaries are paid directly to their accounts, although the district has to submit the monthly payroll indicating presence, exits and entrants. This also applies to staff seconded to PNFPs and means that the local managers have no say about their salary, whether they work or not. Although all HRH functions had been initially decentralized, the payroll function for health workers was recentralized in Financial Year 2001/02. This was done to ensure that all properly appointed staff received their salaries regularly. There had been many reports of districts diverting staff salaries to other priorities and some staff had spent over one year without pay. New recruits took over two years without accessing the payroll (Murindwa et al., 2006). Within a decentralized arrangement, it has been observed that the ability to recruit and fill vacant posts for health workers varies from district to district. Some districts are capable of attracting qualified health workers more easily than others depending on their location and incentives provided by the local administration. The government is currently in the process of assisting those which find it difficult to recruit, through instituting the hard-to-reach incentives. Such incentives have, in the recent past, included financial contribution of an equivalent of six months salary (MOH Uganda, 2007). In a spirit of partnership, even the health workers in PNFP health facilities in the hard-to-reach areas were included on the pay list. In other areas, they have included car and housing loans, scholarships with bonding etc. Kibaale District also gives financial support to health workers undergoing extra studies with a bonding contract to serve the district for at least 2 years after training. However, although bonding ensures coverage especially for the rural areas, it has been shown to be associated with low performance among workers and high turnover rates (WHO 2006). It is difficult for health managers at district level to control their staff because of public service rules which make disciplinary action very difficult. It is even harder if such staff is seconded to PNFP facilities. As a result, seconded staff is generally very difficult to manage. This is also true in Uganda irrespective of the fact that the local governments have powers to recruit (Murindwa et al., 2006). Methodology A descriptive cross-sectional survey was done in Kibaale District and qualitative and quantitative data were collected. The study population was made up of all the 13 faith-based PNFP health facilities in the District with government-seconded health staff. A study unit was a faith-based PNFP health unit in Kibaale District with at least one government-seconded staff. At each health unit, the respondents were the government-seconded staff, the members of the health unit's core management team (HUMT) (comprising of the staff in charge of the unit, senior nursing officer and the chairperson of HUMC). Key informants were the members of the Diocesan Health Management Board, staff of the UCMB and UPMB, the District Director of Health Services (DDHS), members of the District Service Commission (DSC), the District Personnel Officer, and the Chief Administrative Officer (CAO) of Kibaale District. The study tools were first pre-tested in a PNFP health unit in the neighbouring Hoima Diocese, outside the area of study but within the same diocese. Respondents gave their verbal informed consent before the interviews commenced. Results The number and skill mix of government-seconded staff There were 13 PNFP health units altogether, including 1 non faith-based unit which belonged to a tea plantation. By level, they were all Lower Level Health Units (LLHUs) i.e. one Health Centre IV (HC IV), seven HC III and 5 HC II. Of the 13, health units, 8 fell under the UCMB, 1 under the UPMB network, 1 under a private Tea Plantation Scheme and 3 to charitable organizations. There was a total of 19 staff (7 males and 12 females) seconded by government to the PNFPs in the district, falling under 5 staff cadres i.e. 1 medical doctor, 5 clinical officers, 10 nurses, 2 midwives and 1 laboratory assistant. Of these, 15 had been recruited by the government and seconded while 4 had been recruited by the PNFPs themselves and forwarded to the government for secondment. The proportion of seconded staff in each health unit was calculated and the results are summarized in Table 1. The table shows that overall, government-seconded formed 48% of the key staff in all the PNFP health units. However, in some cases they were the only key staff present in the health units. Despite this secondment, the staffing levels were still lower than what was expected according to the Local Government Staffing Norms as shown in Table 2. Terms of employment for seconded and non-seconded staff In terms of job security, we compared the possession of appointment letters from the employer by seconded and non-seconded staff. We found that 18 out of the 19 (or 95%) seconded staff had appointment letters compared to only 7 out 21 (or 33%) among the non-seconded staff. Regarding social security, all (100%) seconded staff were permanent staff and guaranteed of government pension, whereas only 5 out of 21 (24%) non-seconded staff were registered with the National Social Security Fund (NSSF). In terms of salary, all (100%) of the seconded staff got a take home salary higher than that of the ordinary government staff of the same cadre due to extra incentives from the PNFP employer. Non-seconded staff received less than that of their ordinary government equivalent staff. In terms of other benefits, neither the seconded nor the non-seconded staff received transport facilities, and they all received housing facilities when available. Presence of housing was a precondition for secondment of government workers, whereas it was not a condition for direct recruitment by PNFP managers. Concerning disciplinary procedures by the HUMC, only 42% (or 8/19) of the seconded staff felt that the HUMC has the power to discipline, suspend or even dismiss them, compared to 95% (or 20/21) among the non-seconded staff. Of the seconded staff, the rest felt that the HUMC only has the power to reduce their top-up allowances. Both groups equally reported to have received equal treatment from the management when they had social problems. However, seconded staff reported being discriminated against with regard to sponsorship and entrusting with responsibilities. They felt they were not trusted. Perceptions of seconded staff about working with PNFP health facilities None of the seconded staff interviewed had ever been promoted and none of them expected to be promoted on duty. This is because they felt they were not trusted by the PNFP management. All (100%) seconded staff knew that their job-related conflicts were solved by the HUMC. However, only 63% (or 12/19) of the seconded staff reported that the conflicts and disciplinary issues are handled fairly. The rest said that the conflicts are solved unjustly and the disciplinary procedures are unfair. Their main complaint was that the PNFP management did not give seconded staff a fair hearing before dismissal. Most (18/19 or 95%) of the seconded staff said that they were not allowed to do private practice. They maintained that this was unfair since the salary they get is not enough although it was better than that of the non-seconded staff. Moreover government salaries sometimes delay and so they felt that they needed to obtain an alternative source of income.
Despite some areas of discomfort, 14 out of 19 (or 74%) of seconded staff said that they are contented working in the PNFP health facilities and wanted to stay while 26% (or 5/19) said that they were unhappy and were considering to leave. Their main point of disagreement was due to the prohibition of private practice by the PNFP managers. The seconded workers were asked for what they would like PNFP managers to do for them in order to keep them longer. In order of frequency, the following were their main suggestions: hiring more staff to relieve the workload; increase salary top-up; sponsorship for further studies; opening up avenues for promotion to include seconded staff; improved PNFP managers' attitude towards seconded staff; provision of accommodation; allow private practice; provide for more time off-duty; provide transport means; and ensure terminal benefits also for seconded staff. Problems faced by the managers of PNFP units in working with seconded staff The problems faced by PNFP health unit management in employing government-seconded staff in Kibaale District include the fact that seconded staff put more effort and time on their private clinics instead of PNFP health facilities; frequent absenteeism from work; abrupt exit of seconded staff from PNFP facilities without notice; frequent disappearance of materials and medicines from the PNFP stores; limited control over the seconded staff; little commitment to PNFP work by the seconded staff who often leave their patients unattended at the end of official working hours; demand for high allowances for every extra work done. Benefits from staff secondment The benefits of government secondment of staff to PNFP health facilities included reduced operational costs due to the salaries being paid by government to the seconded staff; more services offered to patients; and increase of skills learned from the seconded staff by the non-seconded staff. Problems faced by seconded staff in PNFP units These included harsh treatment by the PNFP unit management, lack of interest in seconded staff; unnecessarily strict management of seconded staff; exclusion from some activities e.g. meetings because the management does not consider them to be their staff; lack of consultation on important issues; prohibition of private practice; discrimination; low incentives; heavy workloads; lack of freedom of speech and expression; little or no off-duty time; lack of transport means; insufficient accommodation; refusal to pay the utility bills for seconded staff; lack of good education facilities for the children of staff; and inability to access scholarships provided by PNFP health units to other staff. Benefits enjoyed by seconded staff The benefits that seconded health workers enjoy in PNFP health centers include being paid salary top-ups from PNFP management in addition to a full salary from government; receiving good incentives and allowances. Proposals on improving the policy on staff secondment to PNFP health facilities Several proposals were advanced by the respondents and key informants on how the secondment of staff to PNFP may be improved. Some stakeholders advocated for increased budget support to PNFP health facilities, to enable them to be able to pay, instead of direct payment of salaries to seconded staff. Others would like to see government meeting 100% of the PNFP wage bill so that all the workers in the PNFP health facilities are paid by government the salary at the government scale. This, they argued, would eliminate inequality in handling employees doing the same job. Some stakeholders wanted the government to second only those health workers who had been recommended by the HUMC of the particular PNFP health facility where the staff is expected to work. This would be after the HUMC had analyzed the qualities, commitment and character of the staff in question. Several others advocated for a memorandum of understanding between the government and the PNFP health sector to stipulate the terms and conditions of seconded staff. Such a memorandum would also cover issues regarding their commitment, hours of work, off-duty hours, over-time and weekend work. It would also delineate the powers of the PNFP management in hiring, firing and disciplining the seconded staff. Some stakeholders recommended a total ban on private practice by all health workers in public and PNFP health facilities. Others recommended that the government should allow flexibility in the spending of allocated funds provided that they are transparently accounted for. Accountability could be in form of realizing jointly agreed output indicators. Discussion The study found out that government secondment is a major source of qualified health workers in PNFP health units of Kibaale District. This is possibly a unique position in the district, since the neighbouring Masindi and Hoima districts do not have similar proportions. It is therefore an indicator of the good collaboration between the PNFP services and the government. This non-uniformity in collaboration has been observed in other studies on the same topic before. It has been attributed to the quality of leadership skills at district and at diocesan levels. Such leadership skills include the ability of the leaders at the two levels to look at the district health system in an integral manner rather than as competing sub-components. They also include good negotiating skills especially on the part of the PNFP managers. Finally, they also include political commitment from the political leaders of the district, but which is subject to the two skills above. However, the proposal of a memorandum of understanding to cover the relationship between the two sub-sectors is a good one. In fact, it was reported that one was already under preparation in the district. The study also found that 79% of the seconded staff were recruited by the local government. This is important for the district have control over the staff and to be able to re-deploy them wherever need has been identified within the district. However, as seen, it distorts the working relationship between the seconded staff and their PNFP managers. However, it is a source of learning for the PNFP managers that the government does its work professionally, by giving their staff appointment letters. PNFP managers were found wanting in this aspect. In addition, most PNFP staff were not registered with NSSF yet registration is a statutory requirement for all private employers with 5 or more employees. This different treatment is clearly one of the reasons that leads PNFP staff to leave and join government where there is a promise of terminal benefits. It is compounded by differences in take-home salaries between the two categories of staff. Seconded staff had some wrong and negative perceptions about working with PNFP health facilities. However, some were genuine and need to be addressed by the PNFP managers. For example, the lack of career advancement and higher education opportunities for seconded staff needs to be addressed. Prohibition of private practice was often mentioned as one of the reasons for the exodus of health workers from PNFP health facilities who join government where there is more freedom and time to do private work. The reasons for this prohibition may be genuine such as conflict of interest over patients, possibility of pilferage of medical supplies and divided loyalty. However, in the face of inadequate salary, PNFP and government managers need to work hard for a solution that will satisfy the health workers in their employ. In the meantime, PNFP managers need to ensure that there is not inequity in salary levels between seconded and non-seconded staff. The study shows that non-seconded staff has some other opportunities not accessible by the seconded staff. Such opportunities need to be valued and the non-seconded staff educated about them, for inclusion in the determination of their total package. They may then realize that they too actually have some advantages over their colleagues. The various proposals on improving the secondment of government personnel to PNFP units also deserve mention. The proposal of government meeting 100% of the PNFP wage bill is probably not acceptable to the key stakeholders of the PNFPs, for fear of an eventual government takeover. However, this has been tried in Tanzania where a contractual arrangement is in place for the purpose. This is probably the most optimal approach to stop attrition between the two sub-sectors. It would guarantee that whenever the government increases the salaries for their staff, then PNFP staff would also benefit. However, the political history of Uganda may negate this. When government systems collapsed in the past, independent PNFP existence managed to maintain the services going. Therefore, apart from the fears of government takeover, fears about the resilience of totally government controlled services are genuine. The proposal to give PNFPs unconditional budget support gives the PNFP management financial power and increases their control over their staff. It also guarantees and enhances their identity. However, government fears over accountability capacity also need to be addressed by the PNFP stakeholders. This is a major concern, especially at lower level units. Previous studies have shown that funds meant for PNFP units were handled outside the official guidelines from the government. PNFP managers would have to guard against this if such an arrangement were to be taken up. Conclusion and Recommendations The study shows that government secondment is a major source of qualified health workers, and implies that the public-private partnership in health (PPPH) in Kibaale District is on the right footing. The majority of the seconded staff were recruited by the local government and deployed at the PNFP facilities, largely without their involvement in the selection. Seconded staff has better terms of service than non-seconded staff, a matter which seems to cause disquiet among the staff. However, other benefits obtained by non-seconded staff are not quantified for comparison. The major challenges faced in managing seconded staff include absenteeism while the seconded staff goes for private practice, abrupt attrition, pilferage of supplies, limited control over seconded staff, little commitment to PNFP work, and demand for huge allowances. However, there are clear benefits of secondment such as reduced operational costs and a wider range of technical skills in PNFP units. PNFP managers seem to be concerned especially over their lack of control over seconded staff. A suitable arrangement needs to be put in place that will balance the managerial and independence needs of PNFP services with the accountability and resource envelope abilities of the government. In view of the foregoing, this paper proposes that the Ugandan Ministry of Health, expedites the public-private partnership for health (PPPH) policy enactment process, and that such a policy should cover the secondment of government workers to PNFP health units. The support model recommended for adoption in the policy is where the government gives the PNFPs the available funds unconditionally, with a clear contract on the desired outcomes. The PNFPs would then have leeway to recruit staff of their choice and manage them accordingly. This would also give guidelines to the districts to follow up the contracts and ensure that the PNFPs fulfill them to the letter. The paper also recommends that PNFP stakeholders develop the capacity of their staff, especially at lower levels, to manage human resources properly, to account for financial resources and to manage contracts. These skills would be very crucial in the new arrangement proposed above. References
© Copyright 2008 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp08017t1.jpg] [hp08017t2.jpg] |
| |||||||||

{kind=link}
{kind=link}