 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
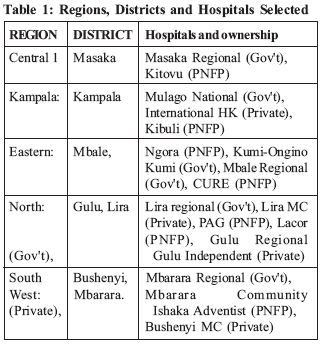
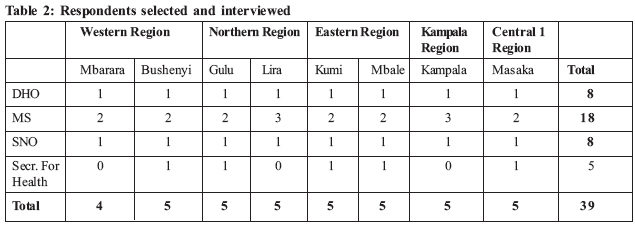
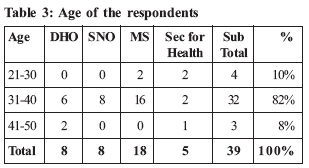
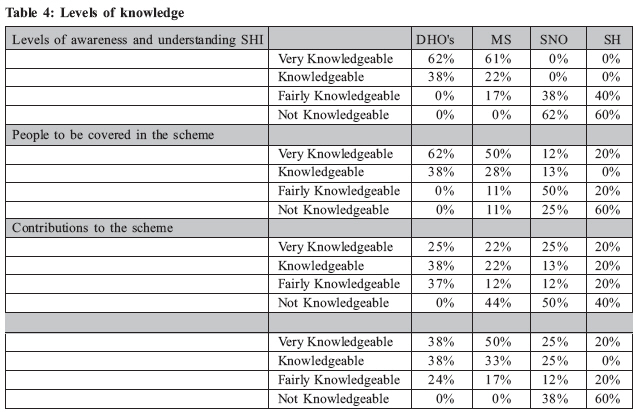
Health Policy and Development Journal, Vol. 7, No. 1, April, 2009, pp. 10-16 Knowledge, Perceptions and Attitudes of Health Managers towards the proposed Social Health Insurance Scheme in Uganda Denis Alyela Omodi Medical Team International (MTI), e-mail: daomodi@gmail.com Code Number: hp09002 Abstract The government of Uganda planned to start Social Health Insurance (SHI) in July 2007, beginning with the formal employment sector, with a view to attain universal coverage in 15 years. Health workers in general and managers in particular, have a crucial role to play in the successful design and implementation of the SHI. This study, conducted in June 2007, meant to assess the knowledge and attitudes of Ugandan healthcare managers about SHI. In so doing, it assessed their readiness to play their role in the implementation of the policy and, generally, gave a clue about the readiness of the country to start the process. The situation does not seem to have changed much in 2009. A cross-sectional survey of health managers in 24 key public, private-not-for-profit and private hospitals, and 8 districts was done. The managers were found to be well aware of the proposed policy but ignorant of its context. They had very high hopes of a large benefit package and yet expected to contribute very little. They felt they had been marginalized in the process of designing the proposed scheme and their roles were not clear. There was no formal training in what they were expected to do once the scheme started. They also had doubts about the integrity of the proposed fund collection and disbursement mechanism. The paper recommended formal training of managers on the policy and its context, their roles, and involving them in the design of the scheme. It also supports postponement of the scheme until key infrastructure and capacity building has taken place. Introduction In developing countries where poverty and lack of access to health care are extremely serious problems, introducing and implementing equitable financing mechanisms and insuring against catastrophic health expenditures should be given high priority in national policy making. Whereas health is regarded as a basic human right, the situation in many developing countries suggests otherwise due to poor funding. However, most developed countries have managed to obtain universal health care coverage due to better funding, some of which is mobilized through social health insurance mechanisms (WHO, 2001). About 1.3 billion poor people still do not have access to effective health care (Carrin and James, 2004). Forty-four countries of the WHO African Region spend less than 15% on their national annual budget on health; 29 national governments spend less than US$ 10 per person per year; 50% of the total expenditure on health in 24 countries comes from government sources; prepaid health financing mechanisms cover only a small portion of population in the region; private spending constituted over 40% of the total expenditure on health in 31 countries; direct out of pocket expenditure constitutes over 50% of the private health expenditure in 38 countries (WHO, 2006). The high cost of health care and the realization that donor funds and tax revenue are not sustainable have alerted governments of developing countries to the fact that the health sectors need more financial resources, and that extra funds have to be sought from other sources. In view of this, many governments in developing countries are considering alternative means to finance their health services, one of which is social health insurance (SHI). Social Health Insurance has been defined as a mandatory scheme of insurance contributions designed to pool financial resources within a designated population to finance a specific package of health care benefits (Hsiao et al., 2001). In Uganda, discussions about SHI date way back in 1987 as part of the recommendations of the Health Policy Review Commission. It was noted then that the health sector was under-financed. Initially, Community Health Insurance (CHI) was introduced in some hospitals as a means of collecting additional funds for the hospitals. Further discussions on SHI in Uganda were resumed in 1997, and heated up after the 2001 abolition of user-fees from public general wards and outpatient services. The Ministry of Health is currently developing and refining the SHI policy and sensitizing different stakeholders, with a view to launch SHI in Uganda soon (Zikusooka, 2007). Whereas, in principle, SHI can make a significant contribution to overall health care financing and support such national goals, its success depends heavily on its design and implementation. There is significant risk that poorly-designed and poorly-implemented SHI could require unexpected government support, increase the degree of market segmentation and social exclusion, and thus impair progress towards priority national health goals, such as the pro-poor health priorities set by the government. Healthcare managers are crucial in the process of design and implementation. This was the motivation for this study, done in June 2007, to assess the knowledge, attitudes and perceptions of Uganda's healthcare managers on SHI. According to the Ugandan Ministry of Health (MOH), the planned SHI will initially cover people in formal employment, with a view of universal coverage in 15 years (MOH, ). Therefore, apart from being managers of services, healthcare managers are also contributors to the scheme and are in a central position. Presently, the policy-makers are busy with preparations for the implementation of SHI, and significant steps have been made in designing the policy. However, there seems to have been inadequate consultation with the key stakeholders such as healthcare managers and service providers, and this is likely to hinder the successful design and eventual implementation of the scheme. Knowledge, Attitudes, and Perceptions of Social health Insurance SHI is always introduced against a background of existing attitudes and traditions in the provision of health services (Zikusooka, 2007). Most advocates of SHI argue that it removes the burden of financing healthcare for employed persons and their dependants from the state, and that SHI members will either no longer use public sector services or will be able to cover the costs of their care if they continue to use state services (Abel-Smith, 1991). In this way, scarce tax-based funds can be released to improve the delivery of cost effective services for the poor (Shaw and Griffin 1995; Griffin and Shaw 1996). Normand and Weber (1994) also urge that health workers' perceptions, attitudes and knowledge ought to be sought before the decision on the provider payment mechanism is made because it has a bearing on their professional behavior -whether they over-treat or over-charge. As with all forms of insurance, SHI is prospective financing (Saltman et al 2004). This means that funds are collected in advance, mainly in the form of regular contributions (or premiums), without knowing when or for whom they will be needed. These contributions come from the insured households and also often from employers and from government. In some countries SHI is universal, i.e. every household is covered, and so every citizen must make contributions, although government may do so for the poorest and the unemployed. In other countries, only parts of the population are covered (e.g. formal sector workers may be compulsorily covered). The contributions go to one or several SHI Funds, which are separate from government but which are generally established by statute, on a not-for-profit basis. The Funds use the contributions to purchase health care services from providers for insured households (often called Fund members). The providers who treat members may be owned by the Fund itself. Or they may be separate public or private facilities, with which the Fund has a contract, and which may also treat other non-member patients too. The services provided to members may be free, or members may have to pay some proportion of the cost when they are treated. SHI systems can operate successfully with either a single Fund or with multiple funds. Where multiple funds exist, they may or may not compete for members (WHO 2006). A single fund will tend to enjoy the advantage of lower administrative and related costs, economies of scale, and will probably not have to advertise for members. It will have strong market power when negotiating service prices with health care providers. Having a single fund also makes it easier to ensure that all citizens receive the same range and standard of treatments. In many ways, a single SHI Fund system is close to general taxation-based healthcare financing. Having multiple Funds will tend to immediately weaken Fund bargaining power with any separate providers. However, even if households cannot choose between the several Funds that exist, it also introduces an element of yardstick competition in that Fund performance can be compared. Where Funds compete for members, administrative costs are likely to rise, as more will be spent on marketing and advertising. This, competitive pressure may force the Funds to be more efficient or, in an attempt to attract and maintain custom, to improve the level of quality offered to members. An important issue is whether Funds should be allowed to compete on price (i.e. contribution level). The views of Ugandan health managers on these issues were not known. An SHI system must be compulsory for a certain segment of the population, if not everyone. Like a taxation-financed system, SHI is built on cross-subsidies (Van de Ven, 2003). Resources flow from the richer to the poorer members of society, as well as from the healthy to the sick. For these cross-subsidies to work, adverse selection must be kept to a minimum. It is easy to enforce compulsory membership amongst the formally employed, as governments can put pressure on employers to reveal their employees' details and extract contributions at source. However, governments in most countries are unable to force informal sector workers, who may be subsistence farmers or work in the cash-only 'black' economy, to make contributions. This is especially true in countries with less well-developed administrative infrastructure such as Uganda. This study also tried to assess managers' views concerning the applicability of SHI in Uganda. Some of the main challenges of SHI include coverage, design and operation, large deficit rates and high enrollees' demands. Governments are frequently tempted to step in to save the schemes, thereby draining public funds meant to serve the rest of the uncovered public. SHI schemes need to assure their members that they will in fact receive the promised health insurance benefits. This implies that the health services that are part of the health insurance benefit package need to exist before the scheme starts or be created by the health insurance Fund. The quality of services and their availability need to be guaranteed. Short of that, it makes little sense to start an SHI scheme. Objectives: The objectives of the study were to determine the level of knowledge healthcare managers about social health insurance in general and of the process being planned in Uganda. We also wanted to understand their perceptions of and attitudes towards the policy and the process. Methodology An exploratory descriptive cross-sectional survey was done. Qualitative, in-depth information about the knowledge, attitude and perceptions of the healthcare managers was collected. It was conducted in five of the nine regions of Uganda used by the Uganda Bureau of Statistics (UBOS) for the 2006 Uganda Demographic and Health Survey UDHS) (UBOS and Macro, 2006). The regions were randomly selected and a total of eight districts were purposively selected from the country on the basis of availability of large private health facilities with many health care managers. Three key health care facilities were purposively selected in each District. These were the government hospital in the district, the largest Private-Not-for-Profit/NGO hospital and the largest Private hospital. The study population comprised of all the health managers/service providers working in government, NGOs/PNFPs and private hospitals and health units in the selected regions. They were also purposively selected. The respondents were District Directors for Health Services, Medical Superintendents of Hospitals, District Nursing officers and the elected secretaries for health at district level. In total, 48 respondents were targeted for interview (8 DHO, 8 Nursing officers, 8 district secretaries for health and 24 Medical Superintendents) but only 39 (or 81.3%) were actually interviewed as shown in table 2. Knowledge of SHI was taken to mean the understanding of its operational concepts and what it entails. We determined the managers' knowledge of the prospective beneficiaries, the level of contribution and the benefit package. This information was collected with self-administered questionnaires and responses were analyzed and ranked basing on the number of questions answered correctly out of 10 knowledge-related questions put to the respondent. "Very knowledgeable" respondents were those who answered 8-10 questions correctly. Those who got right 5-7 questions were rated as "knowledgeable", those who got 4-6 as "fairly knowledgeable" and 3 and below as "not knowledgeable". For attitude, we asked about the respondents' feelings and thoughts about the need for SHI in Uganda, their level of contribution, and the availability of managerial competence and infrastructure to handle the scheme. For perceptions, we asked questions about the likely success of the scheme, the potential involvement of health managers in the design, the potential for universal coverage and the likelihood of achievement of the goals of raising additional funds and equity in access. We used a master-sheet in MS Excel to group responses into relevant themes. The study tools were pre-tested in Mukono Health Center IV, outside the selected districts between 18th and 22nd June 2007. Findings Of the 39 healthcare managers interviewed, 63% were male and 37% were female. Table 3 shows the age distribution of the respondents: Only 10% of the health managers were aged below 30 years and none was above 50 years. All the respondents were married and had children and dependants. In terms of family size, 12 respondents (29.6%) had from 1 to 3 children, and 22 respondents (55%) had 4 or more children. The rest did not indicate the number of their children. Knowledge of SHI Table 4 shows levels of knowledge Health Care Managers have on various SHI issues identified in the study. District Health Officers were the most knowledgeable about SHI. District Secretaries for Health were the least knowledgeable on the policy. There were no regional differences in level of knowledge on the policy and scheme. Most of the Health Managers who were aware of the social health insurance scheme was as a result of workshops, seminars, meetings and interaction with people involved in designing the scheme. Attitudes to SHI There were no regional differences in attitudes to the policy. The majority of the health managers welcomed the social health insurance scheme as a good idea that government should advocate and pursue, because they felt that it will improve health service delivery by increasing finances to the sector and that citizens will no longer have to look for money to take to health units in times of emergencies. However, they were disappointed that the scheme will not cover the poor who actually need it. They also felt that lack of infrastructure, shortage of manpower and mismanagement, particularly corruption, will be a great hindrance to the success of the SHI Scheme. Most of the health managers in the public and PNFP sectors felt that the employees are already over-taxed and they should not pay more. Some of them said that, moreover, as health workers they already have access to the planned package without contributing. Only a minority were willing to contribute less than 2.5% of their salaries to the scheme (a flat-rate amount of 20,000 Uganda Shillings - about US$ 10 per year - was suggested several times). The managers in private (for profit) facilities were more willing to see the scheme start. Perceptions A majority of the District Health Officers and Secretaries for Health viewed the SHI Scheme as a good policy by the government because it will provide more funding for the health sector and that it will reduce the individual patients' cost of the healthcare, enabling even the poor to access good quality health services. However, they felt that all citizens should be covered from the start since illness is a random event and that only a handful of individuals actually fall sick at a time. According to them, therefore, the scheme would not be in danger of collapsing. The main concern for most of the respondents was the suspicion that there was a lack of sufficient management capacity for SHI scheme in the country. They also expected that since they were to be involved in the implementation, they should have also been directly involved in the planning of the social health insurance scheme to ensure that there is harmonized understanding between various stakeholders about the functioning of the SHI Scheme. However, to their surprise, they were not involved and they wondered how they were going to learn about it. Most managers in the private sector reported that they are already under some kind of scheme financed by the employers where they access free or subscribed healthcare, at times with contributions from employees. They therefore wondered whether they were not going to be taxed twice for the same service. The health managers expected easy accessibility of quality, effective and efficient health care, equal provision of healthcare to the population regardless of their incomes and proper compensation incase of death of a beneficiary. They also expected reduction in stock-out of medicines and better salaries for staff due to improved funding Discussion The study shows that there was a high level of awareness about the impending SHI among the majority of the managers, but most pronounced among the DHOs and Medical Superintendents. However, for effective implementation of the scheme, all managers need to be very conversant with the different key aspects of the scheme and policy. Apart from the managers, efforts need to be made to educate the other health workers on the matter. Most of the respondents knew the level of contribution, the beneficiaries, the providers and the scope of the benefit package. However, most also felt that they had been marginalized in the design process. A SHI scheme involves many managers at many levels in the health system. It requires all of them to be adequately trained for their roles. Such roles include client mobilization, customer care, managing the risks of insurance especially fraud and over-prescription, and in guaranteeing quality standards as expected by the customers. The fact that there was only a short time left before the insurance could begin and yet the majority had only received information (not training on their roles) means that the chances of success were limited, despite the goodwill. The study also shows that most of the respondents had very high expectations from the scheme in terms of quality of care and the amount of funds to be raised. Some were not happy with the narrow range of targeted beneficiaries and preferred universal coverage from the start. They also felt that some self-employed individuals could be allowed to become members. These were genuine expectations of a national scheme but given the circumstances in the country, they were unrealistic and suggested that the respondents had not contextualized their knowledge. An earlier feasibility study by a team of consultants unearthed low capacity for a SHI scheme to survive, given the small number of people in formal employment, the low salaries and the weak capacity of government to collect contributions from the private informal sector (Hsiao et al., 2001). This perception also reflects the poor quality of the education and sensitization that has taken place in preparation for the scheme. If managers of this level were not aware of the existing challenges of the scheme right from its start, then the ordinary contributors are expected to have been worse off. Most of the respondents welcomed the idea of starting SHI in Uganda although they had reservations about infrastructure and technical capacity to manage the scheme. This is understandable because in Uganda, there has been a long history of insurance companies defrauding contributors. This was partly due to political instability, which led to breakdown of all government and private sector systems whenever there was regime change. Many insurance companies would simply collapse and the contributors would never have anybody to have recourse to. Moreover, the largest insurer was a government company which would always collapse and change hands after regime change. In addition, there were no regulatory mechanisms for the insurance sector and some private companies started the business when they had no capacity to meet the requirements of the customers. They always had high administration costs and suffered severely from fraud. As a result, they failed to pay the providers and the customers were denied services, thus eroding the population's confidence in the insurance business. There were also few companies which entered the life and health insurance business, although of late there have been some private insurance companies which have made access to care possible. However, people are still wary of a government company or ministry managing the health insurance business. This is largely because of recent major instances of corruption involving contributors' funds or donor project funds channeled through government. Therefore, although the champions of SHI need to invest a lot of time and other resources in designing a good system, they also need to spend equally much in building contributor confidence in a government-mooted insurance programme. In addition to image-building, measures need to be put in place to prevent the much-feared corruption from actually taking place, for if it occurred within the scheme, it would crash the public confidence and prevent further expansion to ensure universal coverage. Although the government has the option of using the law to coerce membership and contribution, such a course of action could have negative political consequences and should be avoided. Conclusion The study showed that although the managers had a good knowledge of the proposed SHI scheme, their knowledge was not contextualized in the reality of the country. They had very unrealistically high expectations of the scheme, thus suggesting poor sensitisation by the policy champions. Although they are key to the successful implementation of the scheme, the managers have not been involved in its design and do not have full information. No training has been done and only information-giving sessions have taken place. All the above suggested serious lack of readiness in the country for starting the scheme at the proposed time of July 2007 and justified subsequent postponement. Since the situation does not seem to have changed in 2009, the justification for further postponement is still valid. In view of the above findings and observations, it is suggested that, in addition to the SHI awareness efforts currently ongoing, training to impart specific skills needed in the SHI programme be carried out for the different levels of managers in the health system, before the scheme can start. A false start will preclude chances of subsequent successful re-starting of the scheme. References
© Copyright 2009 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp09002t3.jpg] [hp09002t1.jpg] [hp09002t4.jpg] [hp09002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}