 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
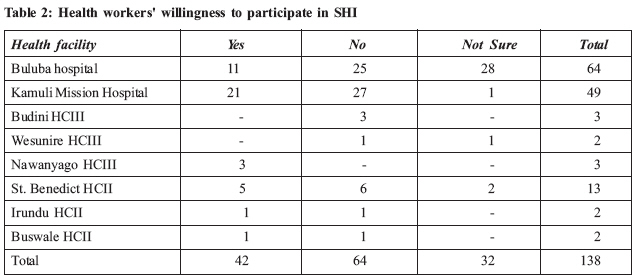
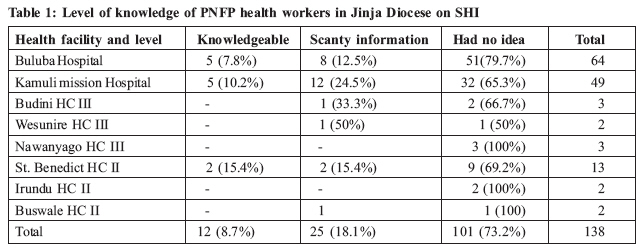
Health Policy and Development Journal, Vol. 7, No. 1, April, 2009, pp. 17-22 Attitudes Of Private Not For Profit (PNFP) Health Workers In Jinja Diocese To The Proposed Social Health Insurance In Uganda Sr. Sarah Nakyesa Senior Nursing Officer, St. Francis Buluba Hospital, P.O. Box 1059 Jinja, Uganda. E-mail: buluba@ucmb.co.ug Code Number: hp09003 Abstract Uganda proposes to introduce Social Health Insurance (SHI). Whereas the idea of SHI is good, the scheme has to be designed properly and carefully, in order to avoid dangers like fraud and especially, cost escalation due to over-prescription. Health workers are, particularly, key stakeholders in preventing cost escalation. Attempting to start a SHI scheme without educating, convincing and winning over the health workers in the country could be disastrous for the scheme. This study was done to determine the knowledge and attitudes of Ugandan health workers to the proposed scheme. It was done in one network of faith-based private-not-for-profit (PNFP) health facilities under the Catholic Diocese of Jinja, in SE Uganda. Despite being done close to the starting of the scheme, the study found that most of the health workers were not knowledgeable about the scheme at all and that they had a negative attitude towards it. The study recommends extension of the period of sensitization, focusing on health workers, but at the same time focusing on improving the design of the scheme to prevent common pitfalls e.g. fraud and cost escalation. Introduction Social Health Insurance (SHI) may be traced back to Germany under Bismarck in the 1880s, when the government enacted legislation to make membership of a sickness fund compulsory for workers earning less than a specified amount. Such membership was funded by employer and employee contributions (Ron et al, 1990). Most European and other upper income countries like Japan, Canada, and Australia had introduced some form of social health insurance by the early 1930s (Roemer, 1991). Within developing countries, Latin American countries have the most extensive coverage with SHI. Since the mid-1980s, there has been growing interest in social health insurance as a health care financing mechanism in developing countries (WHO, 1995) and more recently, SHI has also been introduced in other developing countries in Asia, North Africa and the Middle East. Countries like Mexico, Philippines, Colombia, Thailand, and Ghana have developed Insurance schemes that demonstrate the inherent usefulness of SHI as an important source of supplementary health funding. Some problems associated with the development of insurance schemes have been tackled progressively and their membership continues to grow (Mwesigye, 2006). Social health insurance is one of the health sector reforms currently being discussed in many countries, Uganda inclusive. The consensus appears to be that the poor should be subsidized and that people should be protected from the large financial risk posed by high-cost illnesses. Health and health care are basic necessities for life and equitable access to heath care is a national goal for most countries following the declaration of the goal of health for all (Tarimo and Webster 1996). In Uganda, the 1995 constitution obliges the government to "take all practical measures to provide health care to all citizens" (Uganda, 1995). The subsequent National Health Policy urges the health sector to "develop and support alternative financing schemes such as health insurance to boost health care provision,"(MOH, 1999; p. 20). Several reports show that the majority of the world's 1.3 billion poor people still do not have access to effective and affordable medicines, surgery, and other interventions because of weaknesses in the financing of health care (World Bank, 1993; World Bank, 1997; World Health Organisation, 2000). Low- income populations still rely heavily on out-of-pocket expenditure instead of risk-sharing arrangements to pay for care, thereby exposing themselves to added risk of impoverishment from the multiple effect of income loss during illness, the high cost of health care, and variations in charges by providers (Diop et al., 1995). There is ample evidence to show that the poor are often the disadvantaged, whatever the dimension assessed- that they suffer more ill-health (and death), utilize services less, and pay proportionately more of their income on health care than the better-off (Odaga and Cattaneo, 2004). The introduction of SHI can bring fundamental changes to health systems. These changes have financial implications for health care providers too, for they face changed incentives that could alter their behaviour and impact system costs. Clients also change their care-seeking behaviour, especially if social health insurance and associated reforms succeed at improving access and quality, causing an impact on health care expenditures. Therefore, there will be need for effective regulatory mechanisms for the behaviour of the purchaser and the providers, and strong educative mechanisms for the behaviour of the clients. One particular sub-category of providers that will be affected are the private-not-for-profit (PNFP) providers. In Uganda, PNFP providers are largely faith-based mission facilities located mainly in the rural areas. They depend largely on user-fees and government subsidy for their operations, and donations for capital development. The proposed SHI scheme in Uganda will require people in formal employment to pay 4% of their gross salary and the employers to contribute another 4% for each employee. This could have significant human resources (HR) cost implications especially for PNFP providers with limited income. We considered it important, therefore to explore the knowledge and attitudes of the PNFP providers about the proposed scheme, which was initially due to start in July 2007 but has kept being postponed to July of every subsequent year. There are substantial difficulties in implementing social health insurance. At national level, it requires the creation of new institutions and transformation of some existing ones. New laws and regulations are needed to protect clients and providers. The roles of the government and the Ministry of Health (MOH) often have to change from payer and provider to steward and regulator. The providers must also change their position, from expecting support to working for payment, because under an insurance system, the money follows the patients and those who care for more patients will receive more funds. The clients, too, must get used to making a choice between providers. However, each of these categories must assess and develop its capacity to perform these new roles before the scheme actually starts. In the proposed scheme an independent fund collection and disbursement agency will be created, apart from the Ministries of Health or Finance. Accredited providers will receive payments directly from this agency (Mwesigye, 2006). There are different mechanisms by which reimbursement can be done e.g. fee- for-service payment (providers submit bills for reimbursement), flat-rate payment (specific payments are made either according to age group or depending on classes of diagnoses), capitation payment (payments to the provider, who receives a fixed payment per member for a defined period to provide a defined package of care) and upfront deposit system (an amount of money is deposited with the provider in advance of care and then the excess required is paid after computation, after utilisation of the services). All these mechanisms have inherent advantages and disadvantages and the planners have to make trade-offs and minimize the effects of the selected method. The PNFP health sector in Uganda currently faces a number of constraints that make its ability to participate in the SHI successfully questionable. Yet, it is an important partner, providing about 40% of the health care services and the majority of services in the rural and remote areas. Such challenges include staff shortage due to cannibalization by the public sector. Staff attrition rate doubled from 7.1% in 2003/04 to 16.6% in 2004/05 and 16.8% in 2005/06 (Orach, 2007). Their other key challenge is inadequate funding as government and donor funding have progressively declined to about 23% and 38% respectively (UCMB et al., 2007). Social health insurance therefore stands a chance of further destabilizing the financial and staffing picture of PNFP health facilities because it comes in addition to the National Social Security Fund (NSSF) employer contribution of 10%. Both contributions would be statutory thus seriously raising the employment costs to the PNFP providers. It was feared that this would in the end have negative consequences for the PNFP health workers as well. Therefore, the study wanted to find out their knowledge and attitudes towards the planned SHI. Objectives The objectives of the study were to explore the level of knowledge of PNFP health providers of Jinja Diocese on SHI; assess their willingness to participate in the SHI; find out their planned mechanisms for coping with the challenges of SHI and; to find out their anticipated impact of the SHI on the cost of health care to the providers. Methodology A descriptive cross-sectional study was done and both qualitative and quantitative data were collected. All the seven PNFP health facilities of Jinja Catholic Diocese in south-eastern Uganda, covering five districts, were purposively selected. The units were Kamuli Mission Hospital, St. Francis Hospital Buluba, Nawanyago HC III, Budini HC III, Wesunire HC III, St. Benedict HC II, Irundu HC II and Buswale HC II. The total population of health workers in Catholic PNFP health units in the diocese is estimated to be about 324. A sample size of 138 respondents was determined using Kish's formula and by assuming that 90% of the staff would be knowledgeable about SHI, with the margin of error of 5% at the 95% level of confidence. Selection of health workers from each health facility was done proportionately depending on the number of staff. Thus from Buluba hospital with 150 health staff, we got 64. From Kamuli Mission Hospital with 116 staff, we got 49. From Budini HC III with 8, Wesunire HC III with 5, and Nawanyago HC III with 6, we got 3, 2 and 3 respectively. From St. Benedict HC II with 30, Irundu HCII with 4, and Buswale HC II with 5, we got 13, 2, and 2 respectively. At the health unit, respondents were selected purposively. Findings Of the 138 respondents, 7.3% (10) were managers, 4.4% (6) medical officers, 14.5% (20) nurses, 14.5% (20) midwives, 20.3% (28) allied health professionals, 13% (18) nursing assistants, and 26% (36) support staff. Level of Knowledge on SHI The study assessed the level of knowledge of health providers on Social Health Insurance. The majority of the respondents had no idea about SHI because they had never heard about it. Only 26.8% knew about the planned SHI. Of the hospitals, more of the staff of Kamuli hospital had heard about SHI compared to those of St. Francis Buluba Hospital. Of the HC IIs, more of the staff of St. Benedict's had heard about SHI. This is probably because the two health units are more in urban areas than their counterparts. Knowledge of when SHI is due to start We asked the respondents who knew about SHI for the expected starting date of the scheme. Of the 37 who knew something about SHI, only 17 (or 49.5%) knew the correct proposed starting date at the time. Knowledge of the proposed individual contributions All the 37 respondents who were knowledgeable about SHI knew what percentage of their salary was to be deducted towards SHI. Knowledge of the provider reimbursement mechanisms Explanation of the proposed SHI scheme was given to those who were not knowledgeable about it initially and even those who were knowledgeable received an opportunity to ask questions for clarification. Afterwards, they were asked about the reimbursement mechanism they would prefer for their health unit. All the respondents preferred upfront deposit to be made, and then the balance to be paid after computation of actual usage to avoid stock-outs of medicines. They also preferred that such funds should be deposited directly on the health facility accounts for proper accountability. Willingness to participate in SHI Even after the explanation of the scheme, the majority of the respondents (64/138 or 46.4%) were not willing to participate in the scheme as shown in table 2 below while 23.2% (or 32/138) were reluctant. The main reasons given for reluctance to participate were complaints of low pay, too many taxes and lack of adequate information on the scheme. Preferred benefit package Most respondents preferred that SHI funds be used to cover Outpatient services instead of Inpatient, arguing that inpatient services would quickly consume their funds. In terms of disease conditions to be covered, the majority (65% or 90/138) preferred to have all conditions covered. However, 25% (34/138) preferred that only chronic conditions be covered as they tend to be very expensive, while 10% (14/138) preferred to have only emergencies covered. Institutional readiness for the SHI scheme(a) Legal and Accreditation requirements: The study investigated only the presence of documents required by the law for operation as a health facility and those for accreditation as PNFP health facility under the Uganda Catholic Medical Bureau, the umbrella body of all Catholic health services in Uganda. All the health facilities studied had the legal and accreditation requirements such as a valid health unit charter/constitution, employment manual, manual/ guidelines for the management of financial Resources, Operational License, a comprehensive report for every financial year, and evidence of having their annual contribution to UCMB. (b) Accounting system for SHI funds at health unit level: All the hospitals already had their functional accounting systems which could handle the relevant financial transactions necessary for the SHI scheme. However, all the hospital-based respondents preferred to have accounting systems for the SHI clients separate from those of other revenues of the hospitals. To facilitate this, a separate bank account, books of account, and patients' registers would be kept. The commonest reasons the respondents gave for this preference were to ease claiming for reimbursement, proper accountability, avoid stock-outs, maintain quality services and, generally, avoid making losses on SHI clients. All the respondents from lower level health units preferred to have the funds mixed. (c) Cost control: In the hospitals, most respondents expressed fear of increased costs if they were required to recruit, train and retain more qualified staff in order to provide care for SHI clients. Most respondents also preferred the introduction of a financial contribution to deter the clients from over-using the services. Asked as to how they will cope with potential irrational prescription of medicines, 90% (9/10) of hospital manager respondents reported that they would improve the skills of clinicians through Continuous Professional Development [CPD], close monitoring, and support supervision. Some also suggested the use of a maximum limit of what the clients can receive in a year. Expected impact of SHI on the cost of health care to the providers: All the respondents expected SHI to increase the cost of health care due to increased utilisation of services and increased expectations from the clients. In addition, they expected the health care cost to rise due to increased recruitment costs because they thought that many health workers would leave their units due to heavy workload with low salary in PNFPs. Therefore, the PNFP health facilities would have to recruit new staff. Discussion Level of knowledge of health workers on SHI The study, which was done just before the supposed date of commencement of the SHI scheme, found that the majority of the respondents, who were expected to be contributors, were unaware of SHI. This was mainly due to the fact that sensitization of all stakeholders was very inadequate. The 12 knowledgeable respondents were hospital managers who had just been for workshop organized by the UCMB, this contributed to their being well informed. Health workers are an important stakeholder category in the proposed scheme because they are contributors as well as providers. Therefore, all efforts should have been made by the champions of SHI to educate, win over and involve the health workers in the planning and sensitization of the general community. Lack of knowledge among key stakeholders can be a source of lack of commitment and, eventually, sabotage for the scheme. Most of the staff who were knowledgeable about SHI were those from urban and peri-urban health facilities. This was probably due to better access to current information through the media and access to mobile people. Institutional readiness The study found that the PNFP health units had the basic legal requirements to be accredited for provision of services under SHI. However, an assessment of the scope and quality of care would have been needed to determine the functional readiness to meet the service delivery expectations of customers. In terms of operations, the basic financial infrastructure necessary to handle the transactions of the scheme seems to have been in place in all the units studied. Most of the respondents preferred to have upfront payments for care to avoid medicine stock-outs. In a way, this would also provide some form of assurance to the providers of, who normally operate with limited reserves. However, relevant arrangements would need to be put in place to ensure that even customer interests are taken care of. Upfront payment could predispose to poor quality of care and cost escalation. A lot of negotiation and preparation still has to be undertaken to agree on the conditions of participation as a provider to the scheme. Staff willingness to participate Many staff members were not willing to participate in the scheme, largely due to scanty information about the operations of an insurance scheme. Despite the short time left between the period of the study and the starting date of the scheme, many people still confessed total ignorance of the scheme whereas some had scanty information. This affected their willingness to participate as many people saw the scheme as an extra tax on the meager salaries. This is also a reflection of the inadequate sensitization about the scheme. One would have expected key players to be aware so that they can take informed decisions. Benefit package The study showed that most respondents preferred to have full access to all services they would need. However, given the low salaries in Uganda, this would be an unrealistic expectation because even the contributions would not suffice to cater for the package. There are very few schemes, if any, that provide full access to all the services. More respondents also preferred to have outpatient care compared to inpatient care, arguing that the latter is too expensive and would exhaust the contributions. However, this reflects a poor understanding of one key purpose of an insurance scheme, which should be to prevent against catastrophic expenditure. Most families can afford to pay for outpatient care. It is mainly inpatient care which leads to catastrophic levels of expenditure and which should, therefore, be insured against. Therefore, this further confirmed that the level of sensitization was still poor, even among the educated. Expected impact of SHI on cost Most respondents expected SHI to increase the providers' cost of service provision, because of the increase in number of patients. Some also mentioned the likely increase in costs due to inappropriate use of services and irrational prescriptions of medicines. These are realistic challenges in any health insurance scheme and may be prevented through careful planning of the scheme. A lot of sensitization still has to go on to enable the stakeholders to won the scheme. In community health insurance schemes, it is easier to control aspects of over-use of the scheme because the clients know each other. They can control fraudulent use by non-members and can easily identify those who unnecessarily use the services. However, for a national scheme e.g. SHI, this tight control would be difficult. In the proposed scheme, the beneficiaries would be only the contributor, a spouse and four dependants. A leak-proof system would have to be created to prevent over-use through fraud. Currently, there are reports of over-prescription in health facilities in Uganda. There are no mechanisms for controlling this problem. Therefore, if the country starts a system of reimbursement which does not include tight control over prescriptions, it could soon face financial problems. Conclusion The study found out that there was limited knowledge about the proposed social health insurance scheme in all the PNFP health facilities of Jinja Diocese, especially at lower level health units. Only a few hospital managers were knowledgeable about the Social Health Insurance, having attended a workshop on the matter, and a few peri-urban health workers. Partly due to lack of information and misinformation, most of the respondents were not willing to participate in the scheme. The health facilities had the basic necessities to participate in the scheme although there were fears of cost escalation due to over-use and excessive prescription. Yet, there were no proposed mechanisms, even in the proposed scheme, to prevent and control these challenges. Recommendations We support the idea that commencement of the scheme should be postponed until more efforts are put into designing the scheme properly and educating the stakeholders appropriately. This would reduce resistance, sabotage and the chances of failure. Among the key stakeholders to be thoroughly educated, health workers take a priority. They are key determinants of the quality of care to be provided, the cost of the care that will be provided and they are also contributors. Specific training must, therefore be designed to educate them in their role within the SHI scheme. If the national sensitization strategy is to pass through umbrella bodies e.g. UCMB, we propose that they should be facilitated to ensure that their message reaches the low level health workers, not just the managers. Providers, especially PNFP providers, need to invest in strengthening their systems, in order to be able to capture data to claim for accurate reimbursement of their costs. This entails that they need to know their true cost of service delivery, in order to avoid making losses on the scheme. References:
© Copyright 2009 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp09003t1.jpg] [hp09003t2.jpg] |
| |||||||||

{kind=link}
{kind=link}