 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
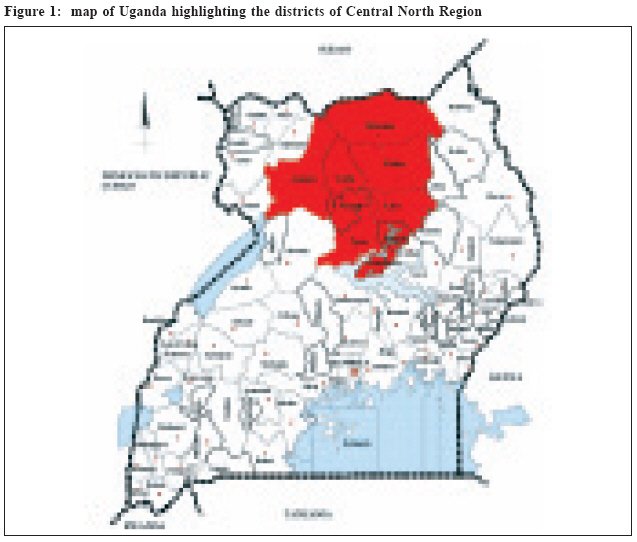
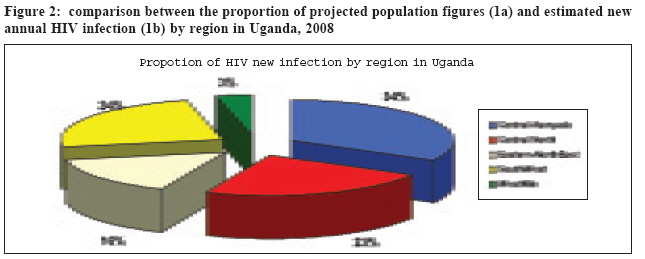
Health Policy and Development Journal, Vol. 7, No. 1, April, 2009, pp. 48-50 Comment: JAMA Article "Risk Factors for Recent HIV Infection in Uganda" Luigi Cicciò Strategic Information Director, Northern Uganda Malaria, AIDS and Tuberculosis (NUMAT) Project, P.O. Box 946, Gulu, Uganda. E-mail: luigiciccio@yahoo.com Code Number: hp09006 An article published in the August 2008 issue of the Journal of the American Medical Association (JAMA) reporting the findings of a secondary analysis of the 2005 Uganda HIV/AIDS Sero-Behavioural Survey (UHSBS) went virtually unnoticed in Uganda and attracted no comment locally, although it contains very significant information on HIV infection trends in the whole country and in Northern Uganda specifically. The article "Risk Factors for Recent HIV Infection in Uganda" (Mermin et al., 2008) analyses the results of the survey with particular focus on the recent HIV infections that occurred among individuals from the survey sample who tested HIV-positive, and factors associated with them. During the UHSBS a total of over 18,000 individuals were tested for HIV, of which 6.4% tested HIV-positive thus attributing the HIV prevalence rate for the whole country (men 5%, women 7.5%). Similarly, the HIV prevalence rate was assigned to different sub-groups based on demographic and socio-economic factors, and for the North Central Region (figure 1) the HIV prevalence was set at 8.2% (men 7.1%, women 9%). The HIV prevalence rate is well known to be just a snapshot of the epidemic situation at a given point in time and it cannot provide accurate information on the actual infection trend, which depends on two difficult-to-measure variables: the number of new infections (incident cases) and the survival rate of those who are already HIV-infected. The study assessed the number of recent HIV infections among 1,023 HIV-positive individuals from the survey sample, using a laboratory methodology able to identify a particular antibody only detectable during the early stage of the HIV infection. A total of 172 HIV infections were actually categorised as "recent", projecting the estimated incidence rate at 1.8 new infections every 100 people per year for the whole country. This is unexpectedly and worryingly high when compared with a stagnant HIV prevalence rate, but it is consistent with the projection derived from a large population-based cohort in Rakai district (Roehr, 2005). The number of recent infections is too small to allow for deeper analysis. Nonetheless the researchers found that some factors were significantly associated to the recent HIV infections. Female sex was one of them, with women having a risk more than double to have developed a recent infection than men; other risk factors included marital status (being widowed or divorced), number of sexual partners in the past year (?2), concurrent HSV2 infection, and geographic region (North Central Region - Acholi and Lango sub/regions - being 2.5 times more to likely have had HIV infection than those living in Kampala and over 7 times higher than those in the West Nile Region). According to the researchers' findings, the incidence rate for the North Central Region could be estimated at around 4.7 new HIV infections for every 100 sexually-active people per year. If this depicts the real situation - the authors warn on some limited validation of their laboratory assay - we should expect around 60,000 new HIV infections per year in the whole region. The actual picture could then be a representation of an increasing prevalence rate, whose initial signs the 2005 UHSBS had just started to display. This would confirm the worst scenario in the estimated future HIV/AIDS burden in Uganda among those hypothesized and compared by the same researchers in another paper (Hladik, 2008). Moreover, this could happen in an environment of extremely mobile populations relocating to resettlement camps or returning to their original places, making social contacts and interactions and therefore HIV transmission easier to occur (Spiegel, 2004). In such context where transactional sex, multiple partners and inconsistent use of condoms are still common (IRIN, 2009), it is not surprising that women are expected to bear the brunt of new infections, further widening the already existing HIV prevalence gap between genders. How bleak the situation is for the North Central Region is epitomised by the fact that the region which has only 11% of the entire population of Uganda is estimated to contribute nearly 25% of all the new HIV infections in the country every year (figure 2). Such a scenario would dramatically overstretch the already frail health system, exacerbating its constraints in the provision of HIV-related health services, namely: the low proportion of pregnant mothers accessing quality HIV testing and ARV prophylaxis; the small number of infants born to HIV-positive mothers who can access infant diagnostic services early; the delayed identification of TB/HIV co-infected cases (whose potential reservoir of HIV-infected individuals would steadily increase); the deepening gap between people in need of ARV therapy and those actually receiving it; and the inadequate coverage of an effective and simple intervention as cotrimoxazole prophylaxis. We should take these estimates cautiously, considering the limitations of the study the authors themselves acknowledge. However, there is documented evidence from south-west Uganda that those declining trends of HIV prevalence (and - supposedly - incidence) in the country are no longer occurring and that the "Uganda model" for an effective control of the epidemic might no longer work (Shafer, 2008). This has to be taken into account in the design and execution of HIV-related interventions, regardless of the precise magnitude of the actual rise in HIV prevalence and incidence. Currently, it is crucial to be vigilant in detecting any abnormal or unexpected change in the trend of HIV-positive rates from those units where HIV Counselling and Testing and prevention of mother-to-child transmission (PMTCT) take place routinely. Apart from surveillance through the analysis of results from testing sites, it is paramount to increase the proportion of the sexually-active individuals that access HIV testing and become aware of their sero-status. This applies also to ante-natal clinics where PMTCT intervention is being conducted and where the component of counselling on and provision of family planning services to HIV+ women should be strengthened. Additionally, intensified prevention efforts to slow down HIV transmission should unambiguously include effective approaches targeting high-risk behaviours especially in areas like bars, discotheques and lodges where casual sex is likely to happen (Sandøy, 2008). It is more controversial whether suppression of HS2 infections can help: though it is well associated with an increased risk of acquiring HIV infection and the prevalence rate for HS2 in the North Central region is close to 50% (Ministry of Health, 2006), there is still no evidence that such an intervention is worth to be scaled-up (Watson-Jones, 2008). However, proper diagnosis and treatment of sexually-transmitted infections should be encouraged, given the high occurrence of these infections among sexually-active individuals revealed by the 2005 UHSBS. Sustained surveillance efforts are needed to demonstrate the true trend in HIV incidence and prevalence and prevent these unpromising predictions for Northern Uganda from materialising. Uganda's HIV epidemic has already experienced a significant decline in its prevalence due to many factors, including concerted efforts in preventive activities. The unique humanitarian, environmental and socio-political situation in the north requires the same synergy and commitment from all concerned health-related actors to anticipate such a powerful threat to this delicate phase of recovery and reconstruction. References:
© Copyright 2009 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp09006f1.jpg] [hp09006f2.jpg] |
| |||||||||

{kind=link}
{kind=link}