 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
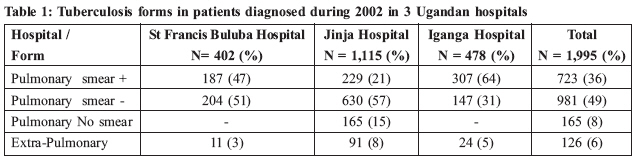
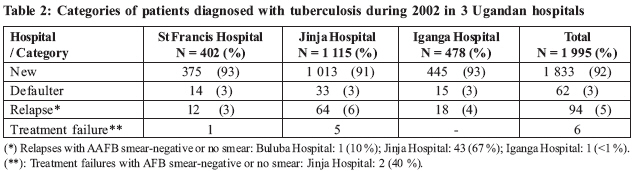
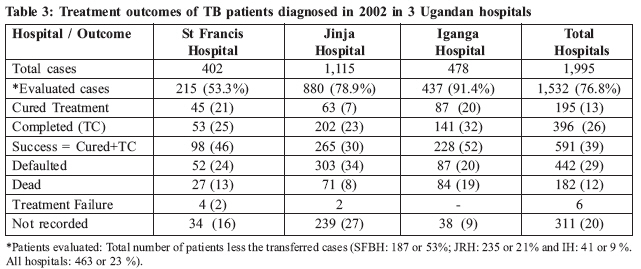
Health Policy and Development Journal, Vol. 7, No. 1, April, 2009, pp. 60-62 Poor Quality of Data and Care Cast Doubts on Reported Success of Uganda's TB Programme: A study of the Unit Tuberculosis Registers of three Ugandan hospitals Jaime E. Ollé-Goig 1,2,3 MD, MPH. Alter Santé, B.P. 190, Djibouti. E-mail: olleuganda@yahoo.com, Telephone: 253 886090 Code Number: hp09008 Abstract With the global resurgence of TB as a public health threat especially in association with HIV-coinfection, accompanied by mismanagement which has led to the emergence of multi-drug resistant TB disease, it is important that care for patients and record-keeping be enhanced. The objective of this study was to analyze the recording of TB cases in Unit Tuberculosis Registers of three Ugandan hospitals in order to identify and quantify the deficiencies in the data registered, for improvement. The design was a retrospective study of the Unit Tuberculosis Registers, with interviews of the staff responsible for entering the data. The setting was three hospitals in the South-Eastern zone of the National Tuberculosis and Leprosy Programme of Uganda - St Francis Buluba Hospital in Mayuge District, Jinja Regional Referral Hospital in Jinja District and Iganga Hospital in Iganga District. All the patients records of cases of tuberculosis entered in the Unit Tuberculosis Registers during 2002 were analysed for the standard TB programme indicators. The Main outcome measures were errors, misclassifications and missing data for each patient registered. The study identified areas for intervention to improve data accuracy. Many so-called cases were diagnosed clinically and never confirmed by laboratory sputum smear examination. Most cases had pulmonary TB. Despite a highly-rated national TB programme, these key field sites showed a cure rate of only 13%, a treatment completion rate of 26% and a treatment-defaulter rate of 29%. These findings are much worse than the reported national figures at the time and suggest a need for the national level to strengthen lower levels further, in order to improve case management, follow-up and reporting. Introduction Uganda is one of the 22 countries with the highest incidence of tuberculosis (TB) in the world which comprise 80 % of its burden. In 2001 the treatment success rate was reported to be only 56 % in spite of the alleged full population coverage with directly observed treatment-short course (DOTS) (WHO 2004). St Francis Hospital Buluba (SFHB) is a rural health institution which diagnoses and treats a large number of patients with TB and is the Sub-District referral hospital of Bunya West in the district of Mayuge, in the South-Eastern zone of the National Tuberculosis and Leprosy Programme (NTLP) of Uganda. After conducting a clinical study of the TB patients diagnosed in SFHB during 2002-2004 (Ollé-Goig, forthcoming), we noted that there were several deficiencies in the recording of the data related to these patients (clinical forms, categories of patients, smears obtained and outcomes of treatment) in the Unit Tuberculosis Register (UTR). The present study was conducted to identify and characterize these deficiencies and compare SFHB to other large treatment centers in the zone. Materials and methods In March 2004, all the patients' records entered in the UTR of SFHB during 2002 were studied. To be able to compare our results with other institutions, we also studied UTR records for the same year in Jinja Regional Referral (JRH) and Iganga (IH) Hospitals, which are located in neighboring districts in the same NTLP zone. At each center, we interviewed the person in charge of entering the patient's data in the UTR to clarify any doubts about the records. We used the standard definitions of the NTLP to classify the patients according to the clinical forms, categories and outcomes. To be able to compare the outcomes of treatment among the hospitals (which had significant differences in the number of patients transferred) we excluded from the calculations those patients who had been transferred to other centers. The standard NTLP regimen for a new patient was 2HRZE/6HE. A patient still having an acid-alcohol-fast bacilli (AAFB) positive sputum smear at the end of the second month of the intensive treatment phase had had this phase prolonged for another month. The regimen for all non-new patients (patients returning after default, patients with treatment failure and patients having relapsed) was 2HRZES/1HRZE/2HRE. Results The 3 hospitals covered a population of about 1.4 million people (327 000 in Mayuge District, 423 000 in Jinja District, and 673 000 in Iganga District). Overall, there were 1995 patients and more than half were detected in JRH. Forms of the disease: Table 1 shows the different TB forms recorded. In JRH no sputum was obtained for AAFB examination in 15 % of the patients treated for pulmonary TB. Most cases with an abnormal chest radiograph in were treated as TB. The proportion of extra-pulmonary forms detected in the three hospitals seems very low, especially in an area with a high prevalence of the human immunodeficiency virus (HIV) infection. Categories: Table 2 shows the patients' categories. Most of the patients (>90 %) were categorized as "New patients" in all the UTRs. The proportion of Defaulters, Relapses and Treatment failures was very small. However, several patients were diagnosed as a Relapse or a Treatment failure even when they had a negative smear or when no smear was done. Treatment outcomes: Table 3 shows the results of treatment in 1532 patients. The proportion of confirmed cured cases was small as a large proportion of patients completing treatment had no AAFB smear obtained during the last month of treatment. However, even after adding the patients completing treatment to those cured, the overall success rate was less than 50 %, below the reported national average. The proportion of patients defaulting was very high in all hospitals (from 1/5 in IH to 1/3 in JRH). The overall case fatality rate was about 10 % (higher in IH) and not very different from the national figures. The number of cases whose treatment outcomes were not recorded is strikingly high: from about 1/10 in IH to more than 1/4 in JRH. Discussion The results show that Buluba and Iganga Hospitals had higher proportions of smear-positive TB cases than Jinja Hospital. This could be explained, in part, by noting that in JRH, 15% of the patients diagnosed with pulmonary TB had no sputum smear for AAFB. The ratio of smear-negative pulmonary TB/ smear-positive pulmonary TB was also more than double in JRH. A contributing factor for this high proportion of smear-negative pulmonary TB could also be deficient laboratory performance in that center. Most of the patients detected in the three hospitals were "New" patients. The high defaulter rates also suggest that many patients end up not being covered by the NTLP. The proportion of Relapses and Treatment failures was small in all hospitals. A positive smear is required for the definition of Relapse or Treatment failure and it is noteworthy that most of the Relapses and Treatment failures were diagnosed in JRH where a significant percentage had no proof of a positive AAFB smear. The proportion of patients with a successful outcome was low in all hospitals but especially in JRH. This could be due to several factors such as a high defaulter rate due to e.g. poor health education, wrong diagnosis or poor history taking which ignores previous anti-TB treatment. To improve the results of treatment, studies should be conducted to identify the reasons why patients discontinue treatment. The high case fatality rate may be related to possible co-infection with HIV. It has been shown that many patients present with advanced TB, HIV disease, or both, when medications have little impact on their course (Harries, 2004). There is a high rate of attrition leading to the treatment outcomes for a large number of patients not being recorded. This is very likely due to the patients being dissatisfied with the diagnosis of TB, especially without evidence, given the long duration and stigma attached to the diagnosis. Defaulting particularly makes it likely for the diagnosed patients to spread the disease in the community and increase the likelihood of resistance to treatment. Conclusion and Recommendations This study revealed important deficiencies in the recording of data in the UTRs of three Ugandan hospitals. Given that the adequate recording of data is an essential component of DOTS (Smith 2004), it is highly doubtable that the Ugandan NTLP is as successful as reported at national level. Without accurate records the precise evaluation of the fate of patients, the performance of the NTLP, and the trends of the TB epidemic cannot be monitored. This is of the outmost importance as TB constitutes not only a health problem to the patient but also a major public health threat. Its control is feasible and is the responsibility of all health workers and systems. According to the World Health Organization, in 2001 only 47 % of the estimated cases were detected (WHO, 2004). As the success rate of those started on treatment was 56 % this means that overall in Uganda only 30 % of the patients with TB completed treatment successfully. Further training of health workers in diagnosing, recording, reporting and treating of TB and of NTLP staff in regular and systematic supervision is an essential first step before these figures can improve. References
© Copyright 2009 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp09008t2.jpg] [hp09008t1.jpg] [hp09008t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}