 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
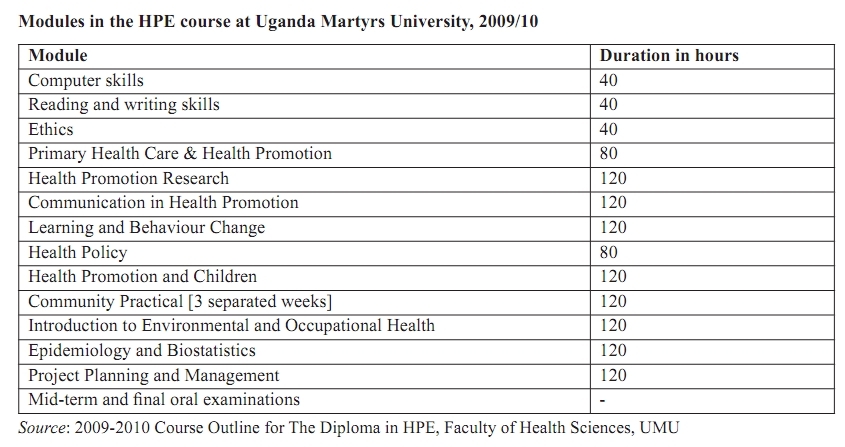
Health Policy and Development, Vol. 7, No. 3, September-December, 2009, pp. 173-179 Miscellaneous Papers Poor understanding of health promotion related to underdeployment of qualified health promoters in Uganda Vivienne Laing Faculty of Health Sciences, Uganda Martyrs University, P.O. Box 5498, Kampala, Uganda Correspondence Address: Vivienne Laing, Faculty of Health Sciences, Uganda Martyrs University, P.O. Box 5498, Kampala, Uganda vlaing@umu.ac.ug Code Number: hp09014 Abstract Health promotion is a relatively new field in the health sector. Having been born as a result of observed weaknesses in the implementation of primary health care (PHC) strategies, it has been slow to pick up in many countries. In Uganda, the Faculty of Health Sciences of Uganda Martyrs University (UMU) picked up the challenge of training health workers in the field of health promotion. Over 100 health workers have qualified in health promotion since 2004. This study meant to follow up the graduates of the programme to see what they are actually doing in the field, to see how their current work is related to health promotion, to see how they perceive their work and to identify the challenges they face in executing health promotion duties. It found that most of them are not in health promotion activities because they have been deployed in clinical services. They attributed this to shortage of clinical staff in health services as well as lack of knowledge of the scope and role of health promotion by the other health workers and, especially, the policy makers and those responsible for staff deployment. The work environment of the graduates is not favourable for the expansion of health promotion activities because of the poor understanding of the field. There are no resources allocated for health promotion, apart from health education campaigns, and many positions are vacant at all levels of the health system. The graduates are isolated from each other and do not receive updated information about the field. The paper recommends sensitisation of all stakeholders of health promotion, formation of a professional association and increased facilitation for health promotion activities, among others. Introduction With over seventy-five percent (75%) of all diseases in Uganda being preventable, the expectation would be that Uganda will have a strong emphasis on health promotion. This is especially true after the Ministry of Health requested that the Faculty of Health Sciences of Uganda Martyrs University commence a diploma course in Health Promotion and Education in 2003. The course started in the academic year 2003-4 with all students actually sponsored by the Ministry of Health via the Global Fund to fight HIV/AIDS, TB and Malaria (GFATM) and, for two subsequent years, via the first African Development Bank (AfDB)-funded Support to the Health Sector Strategic Plan (SHSSP I) project. During academic years 2004/5 and 2005/6, the SHSSP I project sponsored many students as a priority action in capacity building for improvement of service delivery in the project districts of northern Uganda. Background Health promotion first came into prominence in 1986 with the Ottawa Charter which states that "Health promotion is the process of enabling people to increase control over, and to improve, their health" (WHO, 1986). Within health promotion, there are three overlapping spheres namely, health protection, health prevention and health education (Downie et al., 1990). However, the major thrust of health promotion in Uganda has been on the sphere of health education and this has tended to minimise the importance of the other two spheres. Health education is primarily the passing of health information and skills, ensuring a health-literate population. Health promotion has a wider focus and looks at ways to prevent illness and to protect health especially in the use of policies, laws and by-laws. Health promotion has been shown to be a successful approach to holistic health and in reducing the disease burden (Laverack and Labonte 2001). This holistic approach ensures that there is community participation in the development of good health, and thus ensures that there is a receptive response for positive health initiatives that are sustainable. The Ottawa Charter The first major international conference on health promotion took place in Ottawa, Canada, in November 1986, jointly convened by the WHO, Health and Welfare Canada and the Canadian Public Health Association. The conference elaborated a Charter to be followed by member countries. Within the charter, are five strategies namely, to Build Public Policy, Create Supportive Environments, Strengthen Community Action, Develop Personal Skills and Reorient Health Services. It also states that health is not the sole responsibility of the health sector, but that health needs to be addressed from all sectors and at all levels of policy formation. Therefore, health promotion policy should combine legislation, fiscal measures, taxation and organisational change. This aspect thus necessitates a co-ordinated approach to create equity (WHO/CPHA/WC, 1986). To enable this approach to be sustainable, community participation opportunities are needed thus, leading to the empowerment of individuals and communities, which is crucial in improving the health status of individuals, communities and the nation (Labonte and Laverack, 2001). Individuals and communities need to control and own any development strategy for the outcome to be successful. Therefore, there needs to be full participation from start to finish (planning to evaluation) of any innovation, plus a flexible approach to improve the health status of individuals and communities. For this to occur, changes in personal and social development opportunities must be enhanced allowing people to make decisions for themselves and their families. Consequently, health delivery must include health promotion as well as curative services to the population; thus providing a holistic approach to health. This sharing of health between different government sectors not only strengthens the population′s ability to be productive citizens, but ensures that the burden of disease is reduced, thus freeing scarce resources to tackle new and emerging health, social and other development needs. Role of a Health Promoter The role of the health promoter is six-fold and only one aspect focuses on education, namely that of educator. The other five roles are also integral in enabling people to have an impact on their health. They are resource broker, community developer, partnership developer, advocate and catalyst and lastly and most importantly empowerer (Labonte, 1998). Health promotion approaches to reducing the disease burden and allowing people to participate fully in their health issues relies on effective and well trained health promoters as opposed to the concept of telling people what they should or should not do in a vacuum. It is easy to tell someone to do something, even when the people already know what they should do, but there are other influences that affect what people do or do not do. People are influenced by many factors, e.g. economic and political factors, but more importantly by social factors. These social factors incorporate the issues of culture and gender for example and from this premise it is clear that the traditional approach to health education may only improve health literacy, but not affect what people actually do in their day to day lives. Health promotion is not a straightforward approach to health and it brings with it a need to refocus what role people and government take in the provision of all government-led services including health, especially at the policy and implementation levels. The Health Promotion and Education Course at Uganda Martyrs University The health promotion and education (HPE) course comprises of 16 consecutive modules, as identified below. For some time, students already holding another professional diploma, who obtained a high aggregate score determined by the University Senate in advance every year would be given extra training in research methodology and required to do individual research, after which they would present a research report and obtain an Advanced Diploma in HPE. Those who got less or failed to produce a satisfactory research report would obtain only a Diploma in HPE after meeting all the other requirements. Although, there have been some changes in the duration of some modules and introduction of new modules the core modules have not changed. However, there have been new developments and changes in the teaching methods and content of the course over the years, as any good course should do. The focus of this study was to examine if the graduates of the diploma in HPE were impacting on health promotion service delivery after completion of the course at the Faculty of Health Science, Uganda Martyrs University. The main objectives of the research were to ascertain if, following training in health promotion and education at the faculty, service delivery of health promotion/education in their district had changed and what were the challenges faced, if any. [Table 1] Methodology This was an evaluative study conducted throughout Uganda during May/June 2009, using qualitative methods focusing on the views of the graduates of the HPE programme, District Health Officers, District Health Educators and Ministry of Health officials responsible for health promotion services. Forty-eight graduates from five academic years (2003/4-2007/8) were purposively sampled until there were no new data being identified. Thirteen district staff were sampled by convenience and three staff from the Ministry of Health were purposively selected. A semi-structured interview guide was used and individual interviews, small group discussions and two (2) focus group discussions were held. Triangulation was possible and thus, the findings of the study are considered valid, if not representative. Results Location of respondents Twenty-nine districts (of about 100) were visited and from these, eight (8) District Health Officers and five (5) District/Senior Health Educators were interviewed. Of the 48 graduates of the programme interviewed, 33 (68.8%) had been sponsored by the SHSSP project. Others had been sponsored by the Belgian Technical Cooperation (1), Uganda Catholic Medical Bureau (1), partial MoH and Self (3), and fully self-sponsored (10). Of these, 22 (45.8%) had obtained the Advanced Diploma, while the rest obtained only the Diploma. Not all those sponsored by the MoH were working in the health promotion field after qualification; nine remained in their previous job or were promoted within their field or side-stepped into other positions e.g. Focal Person for the Health Management Information System (HMIS). Output and perception of the graduates Regrettably, none of the graduates had published any research on health promotion issues after qualification. However, 2% had carried out research at district level, but it has not been disseminated beyond that level. All the graduates interviewed felt and believed that their skills and knowledge acquired from the Health Promotion course were not being utilised fully. They felt that the primary explanations for this were a lack of knowledge by other health workers and District Health staff of what health promotion is and what health promoters can do. They felt that lack of knowledge was pervasive, including among some District Health Officers (DHO) and administrators. This belief was entrenched by several observations, key of which are the contradictions in nomenclature of posts in the Public Service, which influences recruitment. For example, although the Ministry of Health has a Division for Health Promotion, the Health Service Commission only provides jobs for appointment of Health Educators and this is duly reflected in the job titles and job descriptions. In addition, the Health Promotion Division of the Ministry of Health only produces material and guidelines for Health Education, with no guidance and support for the other spheres of health promotion. The respondents felt that, in the field, being Health Educators, they are mainly used to mobilise the community, especially during the major immunisation campaigns. They felt that, otherwise, their colleagues do not view them as being people with skills to aid in the fight to prevent disease or to improve health conditions. They reported that the only other time they are used is when donor projects which require specific health promotion input operate in their areas or when donor-funded local NGO′s request an input. However, these projects were not common in all the districts surveyed. Hospital-based graduates only focus on curative services and have little or no input into disease prevention via health promotion approaches at hospital level. All the respondents stated that most health workers believe that they can be good health educators even if they do not understand what good health education is or have the necessary skills to carry out good health education. The graduates also felt that their colleagues who were not trained in health promotion did not know or understand the differences between health promotion and health education. Moreover, the graduates reported that their colleagues untrained in health promotion also believed that health education was ′telling people what to do′ and this was reflected in their practices. The graduates felt that this was totally wrong it had led to people having the information, but not using or implementing it. In their opinion, health promotion and health education is a highly specialised profession which should not be viewed as someone standing up and lecturing people about their behaviour whether positive for good health or not. They felt that this approach had actually put people off from attending sessions, because people were tired of being told what to do, especially where they could not see the way forward. An example they often cited was the education about the construction of latrines and the subsequent higher coverage despite lower utilisation. Lack of logistical equipment and resources dedicated for health promotion activities was cited often. Means of transport, fuel, public address systems, and locally appropriate IEC materials were lacking in 27 of the districts visited. Two districts had means of transport in the form of motorcycles obtained them from a donor programme which had now ceased. Staffing of health promotion positions There were health promotion vacancies in every district visited and yet, graduates of the Health Promotion course had not been appointed to those positions. Instead, many of them remained in their previous, often clinical, positions. This was especially true for the graduates who had been sponsored by the SHSSP project, because many of them had been taken from a clinical positions. The graduates felt that they had been denied those positions and various reasons were cited e.g. tribalism or decentralisation. Some (6%) of the graduates interviewed felt that the appointment of health workers should be re-centralised to enable people to be appointed as health promoters on the basis of qualification. Community involvement and challenges in follow up of health promotion activities Most respondents noted that currently, the planning of health education activities in the districts had no community involvement. Since health promotion is based on the premise of enabling communities and on empowering people to address their own health needs, the graduates felt that this approach led to people being passive recipients of a top-down programme. This, they felt, undermines the willingness to implement even the good plans and policies because the community does not own the health promotion programmes and does not see them as theirs. In all the districts visited, there were no health promotion activities based on a local needs assessment. The only activities carried out were based on specific programmes, usually donor led or national programmes enshrined in the HSSP II but which may not be relevant to every district. To implement the said activities, the health promoters have to beg and borrow transport means from other departments to reach the community or hitchhike on transport means going for outreach activities. This prevented continued contact with people and communities, a basic concept of good preventative interventions and even good health education. It was reported that it is common for the follow-up of a health education session to take place one year later. The graduates reported that health care is still viewed as hospital-based curative services with little concept of any long-term view of preventing diseases from actually occurring. This is a short-term approach, which is unsustainable for any country. Prevention of diseases and enabling individuals and communities to stop the "merry-go-round" of continually visiting the health facility for preventable diseases needs to be addressed as a priority. Lack of funding was cited as a major problem with health promotion departments having to work within other departments′ budgets, predominantly within the Health Inspectorate. Where there was a small budget set aside for health education as part of health inspection, it ranged from 1-10% of the district′s budget, the majority being below 5%. Most IEC materials available for use in health education were prepared at the central MoH and were inappropriate and not specific to problems in each district. Some were prepared in a language that the majority of the people from the districts could not understand, thus causing confusion rather than conveying solid and appropriate health messages. The quality of the local language used in other cases distorted the messages. Where IEC materials are used, there is a definite need for them to be appropriate to that specific area and to be in the language that the majority of the people understand. People need to be respected as being in charge of their own health and to be able to read and understand health messages without the need of an interpreter. This is a fundamental aspect of "Health as a Human Right". Health promotion and Health Education At present, the government′s focus is only on health education, as easily seen from job descriptions and job titles, however from the interviews it was observed that some of the graduates were trying to include the other two spheres, namely protection and prevention. Their involvement in other spheres depended on the level of the respondents in the district, there being more involvement in these other areas the higher the level of appointment of the graduate. Overall, it can be said that the time allocation among the three spheres for the most highly placed graduates was Health Protection (12.2%): Health Prevention (31%): and Health Education 56.8%. Whereas the main focus health promotion activities in the district was on health education, the main preventive activities were in school health and mother and child health. This narrows down health promotion considerably and reduces it to only passing on information and a few skills. The external social factors that influence health and the demand for health care are ignored completely. The majority of the challenges experienced by the graduates in implementing health education were very similar in all the districts. The leading challenges were low levels of literacy, the negative influence of traditional/cultural practices, and the demand for allowances for attending health sessions especially after the communities were conditioned by some donor-supported programmes. Many respondents felt that, especially the latter practice had caused a lot of conflict between health staff and communities and has not led to any sustainable positive health change. They felt that the approach of those donors should be changed and that communities should not "be bought" to attend sessions. This would enable community members to actually become part of the programmes and not passive recipients. With only 2% of health promoters carrying out specific monitoring and evaluation of health programmes, the remainder using the HMIS system, which is based totally on curative services, this clearly illustrates that we do not know the exact situation at individual and community level of how effective health education is, far less how health promotion is promoting positive health behaviour. The results of health promotion efforts take long to be seen although they are longer lasting and more sustainable. It is aspects such as these, which make curative practitioners question the whole concept, rationale and contribution of health promotion, compared to curative services whose results are visible immediately or in the short-term. Improving the situation of health promotion in the country MoH and District Health Officers/District Health Educators, all agreed with the reasons given above as to why health promotion was not being implemented appropriately. The graduates and their district level seniors would like the MoH to strengthen the staffing, financing, facilitation and ultimately the performance of the Health Promotion Division. They would also like the Division to advocate and lobby further so that health promotion is widely known and accepted in the country, especially as health promotion is stated to be a priority in both the ending HSSP II and the proposed HSSP III. They also strongly expressed their anxiety in waiting for the MoH to finalise and publish the national policy on Health Promotion and for this to be circulated to all Government Ministries and Sectors including NGOs and community-based organizations (CBOs). In their view, this would help the other staff, especially other health workers, to begin to understand health promotion and the role of the health promoter in the district. This would also allow them to be viewed as a separate profession and for all districts to know and understand the position of health promotion in the health sector and beyond. Such a document would enable the MoH to clarify the distinct skills and knowledge that health promoters have and the approaches they can use to assist people to make appropriate changes for them to take more control over their health. The respondents also recommended that all district health sector staff (DHO, Administrative staff, health workers of all grades, and support staff) should be sensitised assertively on what health promotion is and the skills of health promoters since this was still a new profession in Uganda. The general public and all other government sectors could also be sensitised on health promotion, especially those responsible for policy formation. Specifically, district level health promotion staff very much wanted the number of health promotion posts increased and ensuring that all posts are filled with appropriately trained staff. They are aware that this has major financial consequences for the district level which has an already diminishing health budget. However, they believed that the long-term outcomes of establishing and operationalising extra posts in health promotion would have positive results on the health of the population, especially as a major break-through in the reduction of communicable diseases. Both the graduates and district level staff stated the need for academic institutions in the country to start degree courses in health promotion at bachelors and masters levels. Specifically, they emphasized that this could start at Uganda Martyrs University as the pioneer institution in that discipline. They also proposed that the university should play a bigger role in changing people′s views about health promotion e.g. through organising annual workshop/seminars for all trained health promoters. They also proposed that a new and agreed job description needs to be drawn up in consultation with people trained in health promotion. In addition, a career path for qualified health promoters needs to be drawn by the Health Service Commission so that they also have a recognizable salary scale, career path and a cadre separate from Scientific and Administrative staff is currently the case. They also proposed that health promotion should have a dedicated budget within district health services and that the health promoters should be facilitated to meet with communities to enable them to jointly identify the priority health problems with the communities. This would allow for the communities to be totally involved and for the bottom-up approach to be used thus allowing for ownership and true control over their lives by individuals and communities, in line with the Ottawa and Bangkok Charters. This would enable the health promotion departments at district level to make work plans and to work with communities to achieve the goals and objectives set together and to liaise and work with local NGO′s/CBO′s on health promotion activities, so that bad practices can be eliminated. The respondents also expressed concern about the frequent demand for allowances by the communities and especially the local leaders before they come for meetings or to help in mobilising and sensitising the communities. Nearly all placed the blame firmly on donor-led initiatives where attendance allowance is always given for attending community meetings. This is a major problem in ensuring community participation and sustainability, but also clearly highlights the top-down approach used within the development field. For empowerment and a holistic approach to development and good health, this dependency cycle needs to be broken and this requires committed government intervention. The respondents also felt that the current job description for Senior Health Educator leaves much to the interpretation of the individual districts and is not consistently applied. In addition, the respondents felt that entry requirements into the Health Promotion training programme at UMU which are dependent on national standards but are not widely publicized cause confusion for the districts and the graduates. This has negative impact on efforts to attract more students into the programme. For example, they complained that the government directive that candidates with only a first certificate should not be allowed to obtain an advanced diploma, no matter how well they performed, was unfair. In addition, they also felt that the current directive on the equivalence of an Advanced Diploma to a Bachelors degree was not a permanent position and could be reversed in future to the disadvantage of the graduates. These views were also held by some staff of the Faculty of Health Sciences. District and MoH staff agreed that there is need to make health promotion efforts more inter-sectoral. So far, there is significant Health Legislation in place, but its enforcement is very poor. Health promotion efforts need to come from all corners e.g. qualified graduates, District levels and MoH. Other issues raised were the need for making regular updates in the field of health promotion available to the graduates through workshops and seminars on different aspects of health promotion. Many respondents also emphasized the need for the formation of a national professional association of qualified health promoters, which would have regular meetings and produce newsletters about their work. Over 75% of the graduates felt that this was the responsibility of either the MoH or of the Faculty of Health Sciences, UMU. Discussion Health promotion in Uganda is still very much in its infancy and requires a concerted effort to advance the discipline into not only the health sector, but the entire fabric of society. To achieve the desired effects, health promotion needs a collaborative approach to support the communities and individuals to make the desired changes in an increasingly difficult and changing environment. This cannot be achieved with vacant posts and staff discouraged due to confusion over the acceptance of their qualifications and lack of knowledge by other cadres of what health promotion is. Health education, which is widely practiced in Uganda and widely believed to be synonymous with health promotion, is a narrow component of health promotion. Therefore, the full roles and responsibilities of health promotion need to be disseminated widely and clearly to ensure that everyone knows them. Continuing with the narrow focus will have some successes, but nothing compared in the long-term to initiating all health promotion approaches and working with participating and empowered communities. Health promotion has been shown to be an effective and efficient way to reduce the burden of disease and with over 75% of diseases being preventable, then there is need to question why it is not being implemented and supported. It would reduce the ever increasing demand for good and reliable health services. This lack of knowledge of health promotion is causing poor preventative health care. Good health education is a skill which not all health workers have. Standing and preaching to a group of pregnant women about prevention of mother-to-child transmission of HIV without their husbands present maybe seen as health education, but it is not good health education. As previously stated, social factors play a very powerful role in how and what people do in their own homes. This means that health promotion approaches need to be adapted to every local circumstance e.g. the choice of venue, the timing and the approach used. Much has been written about the dependency syndrome and how difficult it is to involve people without giving them allowances. This approach is still being implemented, even when it is known to be dangerous for community health. By allowing donors to dictate how NGOs and CBOs work, which is not how the Government of Uganda implements its own programmes, causes problems within the communities and makes them dependent on handouts. This situation does not, in anyway, bring empowerment of the people, but disempowerment and minimises the important asset of people. The wrong signal is sent out, stopping people from taking control of their own lives, and placing all the burden on government. Health promoters can play an important role in changing this approach. The process to change this will not be smooth, because there are many who do not want the status quo to change, possibly due to fear of a reduction in their own status or influence. Conclusion Health promotion in its broad sense is not being implemented in Uganda currently despite the presence of qualified staff trained in the discipline. The forthcoming third Health Sector Strategic Plan (HSSPIII) makes health promotion a priority approach. However, there are still many challenges to be overcome, not least of which are understanding the definition and scope of the discipline by the majority of the health workers and policy makers, institutionalizing health promotion into the public service and securing funding for health promotion activities. The few graduates of the Health Promotion programme at Uganda Martyrs University are too few to make an impact yet, in an environment which does not appreciate their work yet. Moreover, they are not yet placed in positions where they can have visible impact on the health of the population. All stakeholders need to be sensitized about the scope and capabilities of the graduates of the programme in the wider context of the discipline. Next steps In view of the above, this paper exhorts the Ugandan Ministry of Health to expedite the approval and implementation of the national policy on Health Promotion. It also supports and encourages the government proposal to implement the HSSP III provisions which make health promotion a priority approach to health care delivery in Uganda. It also supports call for the strengthening of the Health Promotion Division of the Ministry of Health. Such strengthening can only come when all the stakeholders fully understand the scope of health promotion and the roles of health promoters. Therefore, sensitization of all the stakeholders needs to be done first. Part of the strengthening process will include a revision of the job description and job title of health promoters, to widen it from the current narrow view of Health Education and the filling of vacant health promotion posts at different levels of the health system. Health promoters need to be recognized as professionals through the establishment of a professional association which will define training and practice standards and ensure adherence to them. Such an association could benefit from technical support and guidance by the International Union of Health Promotion and Education (IUHPE). Other efforts to strengthen the practice and profession of health promotion in Uganda will include the starting of degree programmes in the field and the holding of regular meetings focused on health promotion issues. Academic institutions such as the Faculty of Health Sciences of Uganda Martyrs University could play a big role in incubating the growth of the profession in the country, by hosting the association and organizing such identification and team-building processes like workshops, seminars and scientific conferences.[4] References
Copyright 2009 - Health Policy and Development The following images related to this document are available:Photo images[hp09014t1.jpg] |
| |||||||||

{kind=link}