 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 1, No. 1, December, 2001, pp. 60-65 Ebola haemorrhagic fever among hospitalised children and adolescents in nothern Uganda : Epidemiologic and clinical observations 1Mupere E, 2Kaducu O.F and 2Yoti Z 1 Gulu Regional Referral Hospital Northern Uganda P. O. Box 160 Gulu; 2 St Mary's Hospital Lacor, Northern Uganda Correspondence: E. Mupere, Gulu Regional Referrar Hospital Northern Uganda, P. O. Box 160 Gulu, Uganda, Fax 256-41-250828; E-mail: mupez@yahoo.com; Code Number: hs01020 ABSTRACT Background
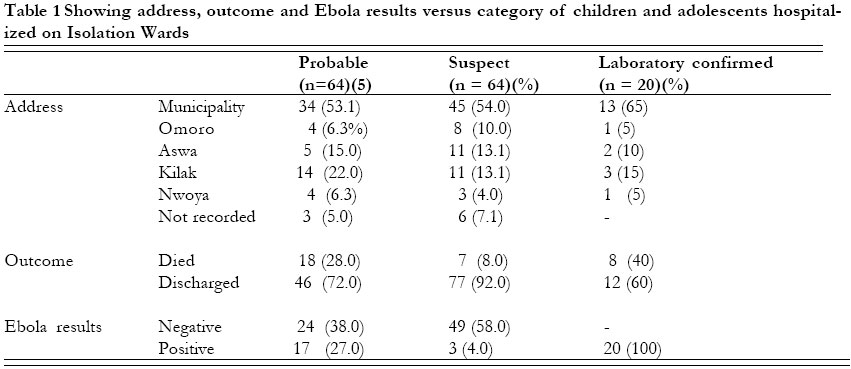
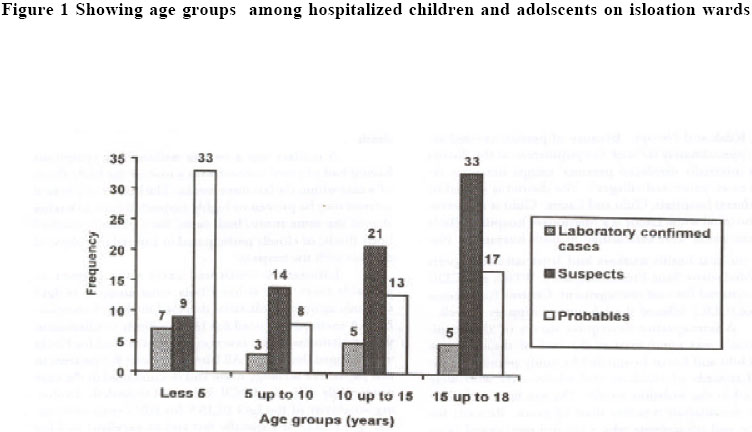
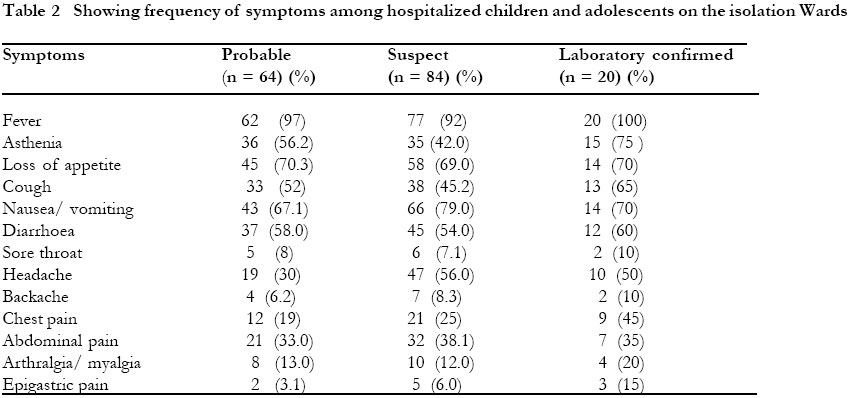
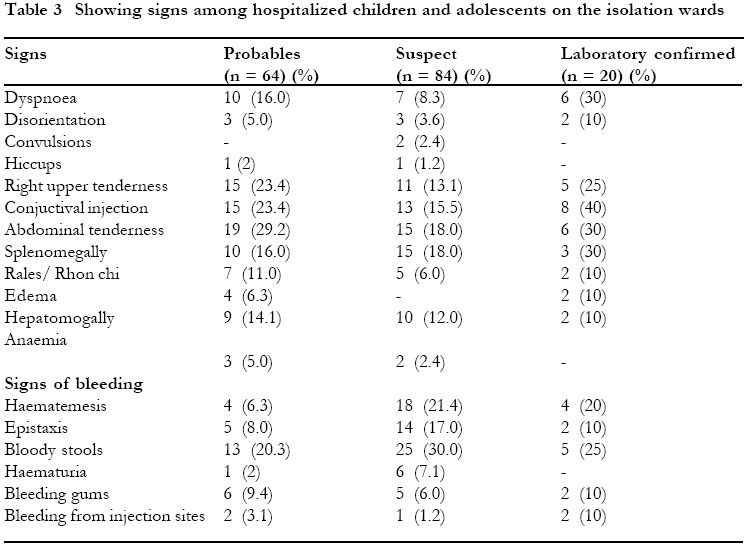
INTRODUCTION Ebola is a lipid enveloped RNA virus belonging to the Filoviridae family of thread-like viruses1,2. Ebola viruses are among the most pathogenic viruses known to humans3. Four genetically different subtypes of Ebola virus are known to cause human illness (Zaire, Sudan, Ivory Coast and Gabon after the place where they were first isolated) 1,2. Ebola haemorrhagic fever (EHF) is often characterized by the sudden onset of fever, weakness, muscle pain, headache, and sore throat, which are followed by vomiting, diarrhoea, rash, kidney and liver dysfunction, and often internal and external bleeding1, 2,3. Ebola viruses are transmitted by direct contact with blood, secretions, organs, or semen of infected persons or through contaminated needle reuse following a 4 to 16 day incubation period (the period between infection and onset of symptoms)2,3. Transmission through semen has been reported to occur up to 7 weeks after clinical recovery4. Health care workers have frequently been infected while attending to patients. No existing treatment or vaccine exists for Ebola, and the reservoir of the virus is unknown2, 3. On 8th October 2000, an out break of an unusual illness in Gulu district (Northern Uganda) was reported to the Ministry of Health in Kampala by both the Medical Superintendent of Lacor Hospital and the Acting District Director of Health Services , Gulu District. The focus of the outbreak was reported to be predominantly in Rwot Obilo, a remote village north of Gulu Municipality. Other cases, some linked to burials in Rwot Obilo, were reported in areas in and around Gulu Municipality. The illness was characterised by acute onset of fever, severe muscle pains, bleeding from multiple orifices (nose, mouth, anus, and vagina) and death. Viral haemorhagic fever was suspected by the Medical Superitendent of Lacor Hospital. At the time of that re-porting; more than ten people, including two student nurses at Lacor Hospital, had died with Viral haemorrhagic fever- related symptoms and signs . On 14th October, the National Institute for Virology laboratory South Africa confirmed the presence of Ebola virus, most closely related to subtype Sudan, in several samples5,6. The overall case fatality was about 50%. The national Ebola epidemic toll was 425 cases out of which 29 were health workers and 214 died of the disease including the Medical Superintendent of Lacor Hospital 7. Two hundred eighteen were laboratory confirmed cases. The last case in Gulu was a 40 year old woman who got infected from nursing her grand child following the mother's death. Uganda was then declared Ebola free on the 27th February 2001, 2 maximum incubation periods later. One of the unique epidemiologic feature of Ebola out outbreaks has been the relative sparing of the paediatric population8,9,10. Herein, therefore, we describe the epidemiologic characteristics and the clinical manifestations of children and adolescents who were admitted to the Ebola isolation ward during the epidemic in Gulu district. METHODS AND SETTINGSGulu district is situated in Northern part of Uganda, bordered in the North by the Republic of Sudan, and has a population of 469,700 persons11. The district is divided into five counties which include: Municipality, Omoro, Aswa, Kilak and Nwoya. Because of persistent rebel activity, approximately 60% of the population in the district live in internally displaced persons' camps hereafter referred to as 'protected villages'. The district is served by two referral hospitals; Gulu and Lacor. Gulu is a government hospital while Lacor is a Missionary hospital. Ebola isolation wards were established in both hospitals. Na-tional medical health workers and International experts from Medeciens Sans Frontiers (MSF), WHO, and CDC were recruited for case management. Centres for Disease Control (CDC) offered the laboratory support as well. A retrospective descriptive survey of the hospital records was conducted at the end of the epidemic from Gulu and Lacor hospitals.The study population included records of children and adolescents who were admitted to the isolation wards. The age limit for inclusion in the analysis was less than 18 years. Records for children and adolescents who were not considered cases were also not included in the analysis. No patient was excluded because of deficient case notes. All records for children and adolescents under 18 years from Gulu and Lacor hospitals were consecutively retrieved. A structured standardized questionnaire was used to collect the data from the patients' case notes. The case notes had been written by doctors (national and international experts) and clinical officers. The nurses had documented the vital signs. Data collection was conducted by two doctors who were involved in the Ebola case management. Social demographic data, clinical manifestations and category (suspect, probable and laboratory confirmed) of the patient were documented according to the records on the case notes. The data was entered in EPI-INFO 6 Software package to facilitate statistical manipulation. Case definitions This paper includes children and adolescents who were admitted to isolation wards and categorized as suspects, probable and laboratory - confirmed cases. A suspect (clinical) case was any person ill or deceased who has or had fever with acute clinical symptoms and signs of haemorrhage such as bleeding of the gums, nose-bleeds, conjuctival injection, red spots on the body, bloody stools and/or melaena (black liquid stools), or vomiting blood (haematemesis). A probable case (with or without bleeding) was contact with a clinical case of Ebola haemorrhagic fever and with a history of acute fever, or any person (living or dead) with a history of acute fever and three or more of the following symptoms: headache/vomiting/ nausea/ loss of appetite/diarrhoea/intense fatigue/abdominal pain/general muscular or articular pain difficult swallowing/ difficulty in breathing/ hiccoughs or any unexplained death. A contact was a person without any symptoms having had physical contact with a case or the body fluids of a case within the last three weeks. The notion of physical contact may be proven or highly suspected such as having shared the same room/bed, cared for a patient, touched body fluids, or closely participated in a burial (e.g physical contact with the corpse). Laboratory-confirmed cases were suspect or probable cases with either Ebola virus antigen, or IgG antibody against Ebola virus detected in clinical samples. ELISA method was used for IgG antibody confirmation while polymerase chain reaction (PCR) was used for Ebola virus antigen detection. All laboratory tests for patients in this paper had serology done and documented in the case notes while a few had PCR done and recorded. Enduring sensitivity of the IgG ELISA for EBO virus antibodies, IgG ELISA is a specific test and an excellent tool for investigation of the ecology of these viruses12. RESULTS The sex ratio (M: F) among children adolescents admitted to the isolation ward was 3:4 while the sex ratios among categories of patients were: probable 1:1, suspect 5:7, and laboratory confirmed 2:3. There was a significant association between the category (probable and suspect) of the patients and the outcome (χ2 = 10.4, p = 00145, OR 4.38). Similarly there was a statistical association between the Ebola results and the category of the patients. (χ2 = 17.30, OR 11.11, p < 0.00003). The duration of hospital stay was 4.9 days. The mean age of children admitted to the isolation ward was 8.2 year ± SD 5.6 while the range was 16.99 years (17 - 0.01 years). The youngest child admitted on isolation ward was 3 days while the oldest included in the analysis was 17 years of age All laboratory confirmed cases were febrile. Frequent symptoms were asthenia, loss of appetite, cough, nausea/ vomiting and diarrhoea. Sixteen percent of the confirmed cases had haemorrhagic signs. Gastrointestinal and respiratory symptoms were prominent while central nervous signs were infrequent. DISCUSSION The sex ratios in nearly all categories of children and adolescents admitted on the isolation wards showed that Ebola affected the females more than males. The females appear to be at increased risk than males. This could be explained by the fact thatfemales play the role of care giving/ or provide nursing care in households hence increased exposure to the causative agent through contact with the sick and their body fluids such as stool vomits and blood. Similar observations of increased secondary infection in females household members were found in the Kikwit Ebola viral haemorrhagic fever outbreak13. Overall, the case fatality among the laboratory confirmed children and adolescents admitted to the isolation wards was (40%) quite close to that of the Sudan epidemis in 1976. This is in agreement with results of the blood samples from the National Institute of Virology, South Africa which revealed that the epidemic was due to Ebola Sudan subtype3. The case fatality was higher among the under fives than the older children probably because the under fives had prolonged period of close contact while on the ward with their parents and therefore, acquired higher viral load. Most of the patients, including laboratory confirmed children on the isolation ward, came from the Municipality in Gulu district. This could be explained by the fact that the epidemic started from a remote village near the Municipality. There was a significant association between the category of the patient and the Ebola test results (p < 0.01). Those who had contact were 11 times more likely to turn positive on Ebola screening. The proportion of those who were Ebola positive is higher in the probables because of direct contact with a clinical case of Ebola than in the suspects and the reverse is true. Close contact and exposure to body fluids of an infected person have been a major risk factors for transmission of Ebola virus in hospital settings and intrafamilial spread in several Ebola outbreaks 5,9,10. Similarly, there was significant association between the category of the patients and the outcome (p = 0.0145). Those who had contact were 4 times more likely to have a poor outcome, therefore, the proportion of confirmed patients who died in probables is more than the suspect. This could be because direct contact to the clinical case probably exposes an individual to a heavy viral load and yet the population appears to lack specific immunity to Ebola virus. The under fives had more admissions among the laboratory confirmed and probables than the suspects who had a higher number in the older age group (15 up to 18 years). This could have been because a number of young children were admitted to isolation wards following admission of their parents. Close relatives declined care for them because of fear of contracting the deadly disease. These children later became Ebola positive on serology while on the ward and symptomatic. The older children and adolescents might have contracted the disease from nursing of their parents or close relatives and attending burial ceremonies. Further more there was a steady increase of suspects with increase in age overall and a relative decrease of the probables. This observation implies that the risk of exposure to the causative agent probably increases with age. Three older children and adolescents among the suspects turned positive on screening for Ebola. This finding is in agreement with the common clinical and epidemiologic features of viral haemorrhagic fevers prim arly affecting the adults8,15. The adults have increased likelihood of exposure to the causative agent8. In the current survey of hospital records, out of 93 children and adolescents who were screened for Ebola, 20 (22%) turned positive. The national laboratory confirmed cases16 were 218. Therefore children and adolescent contributed only 9% (20/218) of the confirmed cases. Most of the patients in the national out break were adults16. Similar findings were found in the previous Ebola outbreaks5,13, reflecting the relative sparing of the paediatric population. In general the frequency of case manifestations were higher among laboratory confirmed than the probables and suspects. However, laboratory confirmed cases were suspect or probable cases with either Ebola virus antigen or IgG antibody against Ebola virus detected in clinical samples. All Ebola confirmed children and adolescents on the isolation ward were febrile though only 16% had bleeding manifestations. Neurological symptoms were infrequent. Clinical manifestations observed among the laboratory confirmed children and adolescents in the epidemic were comparable to those observed in several previous Ebola epidemics 17,18. The gastrointestinal and respiratory symptoms were prominent while central nervous symptoms were infrequent. A number of children and adolescents in this epidemic were admitted on the isolation wards with haemorrhagic manifestations but later turned out negative on Ebola antigen and antibody tests. Similarly several laboratory confirmed cases in the early phase of the disease had non-specific symptoms of Ebola haemorrhagic fever which were often indistinguishable from those of disease that are much more common in the tropics, notably malaria, shigellosis and typhoid fever. Therefore, initial management should include empiric therapy and laboratory tests against their agents. CONCLUSION The observations in this Ebola epidemic regarding the children and adolescents is in agreement with the previous findings8,9,10 that the paediatric population is relatively spared. Only 20 (9%) of the 218 laboratory confirmed cases nationwide on the isolation wards were laboratory confirmed children and adolescents under 18 years of age. The clinical manifestations were similar to the previous Ebola epidemics 17,18. The under fives were at an increased risk of contact with the sick and dying Ebola parents. In the event of a future Ebola epidemic, strategies to shield children from exposure to the sick and dying Ebola relatives in hospitals and families are recommended. Health education to older children and adolescents to avoid risk of contact with sick relatives and their body fluids should be emphasized. AcknowledgementsWe acknowledge quality service to the Ebola patients in the isolation wards by all national and international experts and support staff. The medical superintendent of Gulu and Lacor hospitals for allowing access to hospital records, Michael Odie for the statistical help and Evelyn Kabanyonza for secretarial work. DedicationThis article is dedicated to the late Dr. Matthew Lukwiya, Medical Superintendent Lacor Hospital, who risked his life to provide quality care to the Ebola patients and in the event died as 'hero'. May his soul rest in eternal peace. REFERENCES
Copyright 2001 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs01020t1.jpg] [hs01020t3.jpg] [hs01020t2.jpg] [hs01020f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}