 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 1, No. 1, December, 2001, pp. 73-82 Contraceptive security, information flow, and local adaptations: Family planning Morocco *Yasmin Chandani and Gerry Breton DELIVER, John Snow Inc. 1616 N. Fort Myer Drive, 11th Floor, Arlington, Virginia, USA 22209 *Correspondence: Yasmin Chandani, 1616 N. Fort Myer Drive, 11th Floor, Arlington, Virginia, USA 22209, Telephone: 703-528-7474; Fax: 703-528-7480. E - m a i l : y a s m i n _ c h a n d a n i @ j s i . c o m , gerry_brenton@jsi.com Code Number: hs01022
ABSTRACT Background
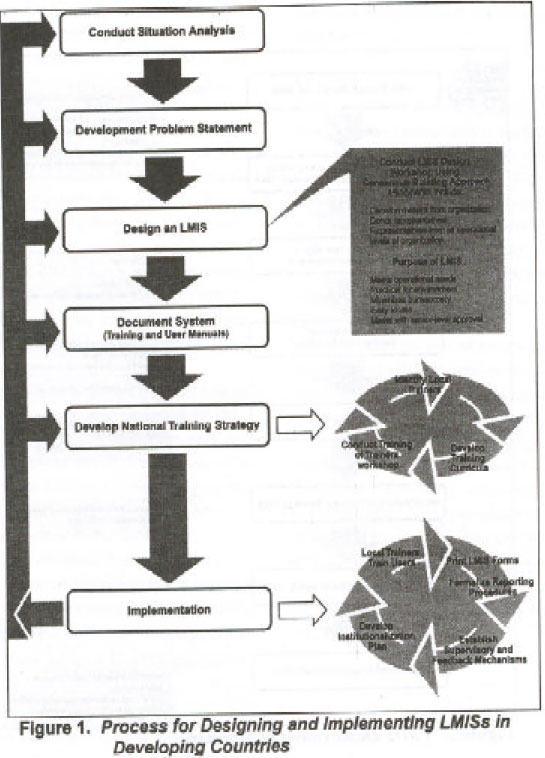
INTRODUCTION Family planning programs, a vital ingredient of socioeconomic development, form a cornerstone of national policy in many developing countries. After the 1994 International Conference on Population and Development in Cairo, governments have increasingly acknowledged the importance of family planning, particularly in opening opportunities for socioeconomic development1. Government spending on health, however, tends to give priority to curative rather than preventive care, and scarce health resources are usually allocated for essential drugs rather than contraceptives2. To ensure the security of family planning programs, therefore, donors have historically provided free contraceptives to governments and organizations that offer family planning services. Family planning programs depend on the uninterrupted flow of contraceptives through multiple levels of the supply chain, ranging from central warehouses to health clinics and community-based distributors. Failure of the supply chain-or logistics system-causes an erratic supply of contraceptives, which may result in loss of credibility and eventual failure of the family planning program. Ensuring the continuous availability of contraceptives at the client level is a key contributor to increasing the use of family planning services3. The driving force behind a logistics system is a well-functioning logistics management information system (LMIS)4. Efficient management of the flow of information on stock levels and consumption from lower levels to the center stimulates the flow of contraceptives back down the supply chain. An LMIS helps determine what quantities of each product need to be sent to a particular location, at the right time, for the right cost. The flow of stock-level and consumption data along the same channels can inform decisions critical to meeting current and future family planning needs. Benefits and Challenges of LMISs Developing country organizations, however, face a number of obstacles in designing and implementing multi-tier LMISs, including a dearth of technical skills for designing and implementing such systems, lack of resources, inadequate infrastructures for technical and communication services, and low literacy rates6. These challenges are exacerbated for organizations working in the public sector, as they must also deal with such barriers as formalistic bureaucracies oriented toward control rather than service7, rapid staff attrition, and an underdeveloped organizational capacity for management8. Another problem that many developing country organizations face is that the processes for design and implementation of information systems often entail a topdown approach but fail to address the needs or support the activities of those using the system. Experience has shown that externally designed and developed systems imposed on a country or program have limited chances of success or adoption9. The most successful examples of adoption and continued use of information systems in developing countries are those systems designed by the user to support their specific needs10. All logistics systems have the same ultimate objective: to obtain and move appropriate quantities of supplies in a timely fashion to places where they are needed, at a reasonable cost11. An LMIS that enhances the flow of information is critical to the successful implementation of a logistics system12. Successful adoption and continued use of an LMIS in a country, however, depends on a combination of customization of the system during its design to the particular country or program environment and, thereafter, continuing adaptations by the system's users. This helps ensure that the LMIS continues to meet users' needs in a changing environment. This paper illustrates why customization and adaptations are crucial to deployment and continued use of LMISs in the public sector context of developing countries. A case study from Morocco, presented later, shows customization of LMIS design and implementation in deploying a functioning system within the specific context or environment. It was found that nstitutionalization of the system was closely linked to the degree of institutional support that affected local funding, adaptations by users, and availability of local technical expertise. This paper clearly explains how these factors shape the support and, ultimately, the sustained use of the LMIS. Design and Implementation of LMISsSince 1986, the Family Planning Logistics Management (FPLM) project, funded by the United States Agency for International Development (USAID), has provided technical support to family planning program managers, trainers, and logistics professionals at the national, regional, and community levels, in more than 30 countries. In general, John Snow, Inc. (JSI)/FPLM uses a standard process to design and implement an LMIS. A participatory approach has been shown to be most successful in designing LMISs, because users who express a high level of satisfaction are most likely to use information systems13. LMISs are built using a consistent framework, and are intended to gather the essential data elements while meeting the local management needs of each country. Data flow mirrors existing procedures and policies. Typically, the request to work in a country originates from a joint agreement between the Ministry of Health (MOH) and the USAID mission in the country. Specific terms of reference are developed according to the mission's strategic objectives and available resources. Figure 1 shows a process for designing a new system, although it may be adapted to suit the specific situation. MethodologyMorocco was selected for the case study for three reasons: JSI/FPLM had a long-term involvement in the country; the involvement had ended and the researchers had relatively easy access to key informants and information regarding the country's LMIS. Two research objectives were identified: assess the process of adoption and continued use of information systems deployed in Morocco; and identify the critical factors necessary for achieving institutionalization of LMIS. The research activities consisted of a review of relevant background literature and secondary data sources (consultant trip reports and publications). In addition we held qualitative interviews with key informants using semi-structured questionnaires (informants were selected based on their availability and knowledge of and experience with the systems assessed). Follow-up calls, faxes, and e-mail correspondence, were used for clarification, when necessary. Limitations
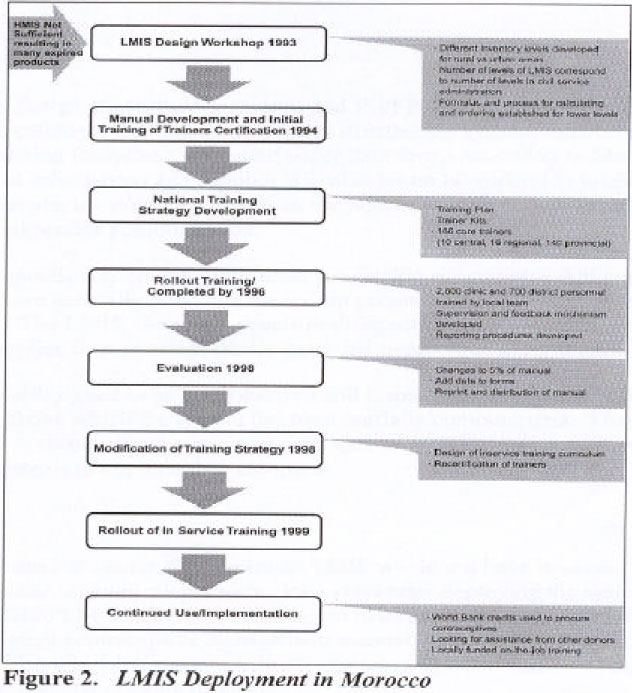
RESULTS: THE MOROCCO CASE STUDY JSI/FPLM began working in Morocco in the late 1980s after the national family planning program requested USAID assistance to improve its logistics system. The existing basic distribution system of the MOH was experiencing problems, evidenced by large amounts of expired contraceptive products in the country. The health management information system (HMIS), primarily a planning tool for the Statistics Department and a separate entity within MOH, did not provide adequate logistics information for inventory management decisions but rather provided summary information for consumption and stock levels. Figure 2 summarizes the process of designing and implementing an LMIS for the contraceptive logistics system in Morocco, for which JSI/FPLM provided technical assistance and USAID contributed significant funding. As shown in figure 2, deployment of the LMIS began with a design workshop in 1993. Representatives of both higher and lower levels of the logistics system attended the workshop, and they helped customize the system to the local context. Rollout training and implementation occurred during the next three years, after development of a curriculum, manuals, a national training strategy, and certification of trainers. Since its inception, the LMIS has ensured a continuous flow of contraceptives to clients and has provided benefits to all levels. The lower levels- the service delivery points-use established formulas and procedures for calculating and placing their orders. The central level evaluates correct use of the formulas, verifies order quantities, and, if inaccuracies are found, provides feedback to the next lower level. The two key factors contributing to the unifying performance of the LMIS are (1) the initial design and implementation of the system, and specifically, the customization of the LMIS to the Moroccan context; vided benefits to all levels. The lower levels-the service delivery points-use established formulas and procedures for calculating and placing their orders. The central level evaluates correct use of the formulas, verifies order quan-tities, and, if inaccuracies are found, provides feedback to and, (2) because of changing environmental factors, logistics managers continuously adapted the LMIS after implementation to maintain its validity. Customization Inventory levels specifically address provincial geographic constraints. Although communications in Morocco are generally good and the terrain presents few problems, some mountainous areas are remote. The LMIS, therefore, specifies different inventory levels for rural and urban clinics to ensure that supplies flow to urban clinics more frequently than to rural ones. JSI/FPLM did not designed the LMIS to be computerized but, instead, relies on paper reports at regional and local levels, above which the system has been partially computerized. The HMIS and LMIS have been linked in theory, if not yet in practice. One of MOH's latest initia tives is to analyze data from both systems to see how they compare. Adaptations
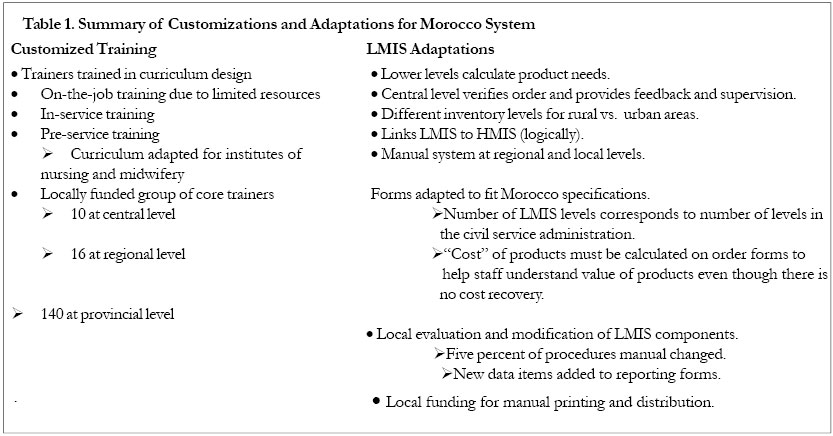
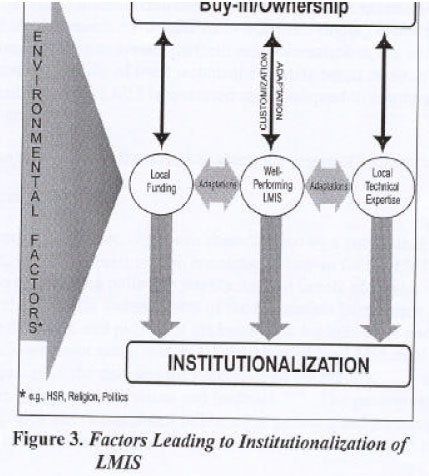
Project managers are aware of the continuous need to improve and adapt to ensure ongoing functioning of the system. “The LMIS has to be constantly maintained, customized, and evaluated to ensure its survival,” the Family Planning Division (FPD) program administrator noted14. Users have suggested additional form modifications for ease of use. A move is under way to compare data from the HMIS and LMIS to implement further improvements. A key indication of Moroccans' belief in the LMIS's utility is the current proposal to expand the system to include noncontraceptive products. Table 1 provides a summary of customizations and adaptations made to the Moroccan LMIS. Discussion Establishing a well-functioning system customized to meet users' needs, however, does not guarantee that the system will be nurtured and maintained-and ultimately institutionalized-after the technical expertise and funding provided by donors is withdrawn. Adaptation by users is key to ensuring that the system continues to meet the program's needs. Equally important for ensuring institutionalization, however, is whether such adaptation is supported by local technical expertise and funding and is enabled by the political, economic, and social context in which the system operates. The continued use of the LMIS and, ultimately these factors, have strongly influenced the degree of institutionalization. Based on the study findings, a framework to assess institutionalization of an LMIS, using these factors, was developed and is presented (see figure 3). Figure 3 illustrates the key factors in determining whether or not an LMIS can be said to be institutionalized in a country. Institutionalization of the LMIS exists when all three factors at the center of the graphic-local funding, a well-performing LMIS, and local technical expertise- are present. The existence of these three key factors, in turn, depends on the degree of institutional ownership of the LMIS at both operational and policy levels. The case study demonstrates the critical nature of institutional commitment for ensuring adequate political will to support and protect the LMIS in a changing political, economic, social, and cultural climate. Without user buy-in at all levels of the system, there does not appear to be significant impetus to achieve the following key conditions for institutionalization of LMIS: the push to garner local funding to maintain system operations, the ability to attract and retain local technical expertise, and the creation of incentives for program managers to continue to adapt the system towards improvement. Without all three conditions, institutionalization would be difficult to achieve. Rapidly fluctuating political and economic environments in many developing countries can lead to significant disruptions in logistics system performance. Nonetheless, the combination of sufficient funding and availability of local technical expertise based on strong institutional commitment can ensure that the LMIS is protected and is adapted to continue functioning within the changing environment. The following discussion uses the framework to assess the degree of institutionalization in Morocco (see figure 3). Ownership of the SystemJSI/FPLM's intervention in Morocco has been characterized by a continuous, high level of institutional support, which has been vital in encouraging buy-in for the LMIS at all levels. Nationally, Morocco has a strong policy on population and family planning. Within MOH, the Family Planning Division (FPD) and members of the Population Directorate instigated the design and development of the LMIS and pushed to get better data for indicators and decision making. The FPD program administrator noted that, “ . . . managers of the LMIS must make a constant effort to verify the quality of the data and the timeliness of the reports. . . These managers must also ensure that there is regular supervision and feedback.”14 The government has had own-ership of the logistics and management information systems and a strong degree of commitment to and control of the systems from the start, as well as focused ideas on system design and goals. Although the central level was responsible for getting the system started, operational results helped draw in support from all levels. Smooth functioning of the LMIS requires that users from all levels take responsibility for the system's success or failure and that they be committed to its maintenance. A consultant with more than 10 years work experience in Morocco noted that initial high-level support for the LMIS gave it credibility. Then, as the system began to work well, people paid more attention to it. Lower-level personnel quickly observed and experienced the benefits of using the new system. They determined their own orders and began receiving the quantities they had ordered at the time they needed them, greatly reducing expiries and stockouts. This reinforced users' ownership of the system. The LMIS in Morocco has been housed consistently within FPD at the central level, and has not suffered from problems relating to institutional transitions. As illustrated in the framework (see figure 3), the degree of institutional commitment for the LMIS plays a strong role in determining whether or not local funding is available to support LMIS operations after donor funding is phased out, and whether adequate and appropriate technical expertise is retained for the system after external technical assistance is withdrawn. Transfer of Responsibility: Local Funding and Local Technical Expertise for Maintaining the LMISUSAID funded the initial design and implementation of the LMIS and JSI/FPLM provided the technical expertise. USAID also procured contraceptives for the country's needs. The idea was to deploy a functioning LMIS that would allow the country to effectively and efficiently manage their contraceptive supplies and gradually transfer capacity for managing the system to local users. Thus, although all initial startup costs came from external sources, the goal was that eventually the country government would bear the maintenance costs for the LMIS and the costs for the commodities. The transfer of responsibility for funding has occurred in two phases: the end of logistics technical assistance provided by JSI/FPLM bilateral project (in 2000) and gradual phaseout of USAID's funding for contraceptive commodities (ending in 2000). Funds from the bilateral project supported much of the initial training for the LMIS. As the project ended, declining availability of training funds and the institutionalization plan caused Moroccans to switch from effective but expensive mass LMIS training events to integrating LMIS training with less expensive pre-service and in-service, on-the-job training. USAID funded a workshop in curriculum design for the national training team so they could develop logistics curricula both for in-service training and for insertion into the general health pre-service training curricula. Currently, all operational functions necessary for the continued performance of the LMIS in Morocco are funded by the government, including salaries for LMIS support staff, training, printing and distribution of forms and manuals, reporting, analysis of data, and supervision visits from central to lower levels. The number of central level staff dedicated to maintaining the LMIS was unaffected by the end of the project because project funds were never used to pay for their salaries. For commodity funding, Moroccans have responded to the planned USAID phaseout in several ways. First, Morocco has begun to seek funding for contraceptives from other donors and, currently, they use World Bank credits to purchase a portion of its supplies. Second, LMIS effectiveness and efficiency have become even more valued. According to a consultant, “Morocco is buying more and more of its own contraceptives, so for them (the LMIS) is a way to make sure that they can minimize their costs without running the risk of either expiry or stockout.” Nonetheless, it is important to note that the transition has not been without problems; technical expertise is still required, albeit on an infrequent basis, particularly for helping Moroccans procure their own contraceptives. Furthermore, commodity funding is only guaranteed for the short-term future. Morocco received its final shipments from USAID in the fourth quarter of 2000 and the World Bank loans expire in 2001. Political and Economic FactorsFamily planning in Morocco has a high profile. The royal family sponsors family planning campaigns, and the government is willing to dedicate resources to and place priority on family planning activities. As a result of MOH's strong family planning policy, the LMIS has received senior management support, which is “critical to the development, implementation, and use of Logistics Information Systems.”15 Decision makers within the program are willing to dedicate resources to maintain the system because it has demonstrated its cost-effectiveness, a critical consideration for the program in the face of USAID funding withdrawal. The Moroccan government is considering decentralization of the logistics system, which could lead to the creation of regional manager positions and an increase in responsibilities for provincial managers. Logistics functions and the LMIS would both be decentralized to regions, where data entry would also be conducted. To maintain a well-functioning LMIS in the face of decentralization, the central level would have to set standards for provinciallevel LMIS activities, such as training and supervision, that provinces would be encouraged to follow. Physical infrastructure has also played a determining role in ensuring the success of the Moroccan system. Communications are relatively advanced; for example, many facilities have access to telephones and faxes, which enhances the ability of supervisors to provide feedback. Physical access and transportation is only problematic in some remote areas-an obstacle that personnel have managed to overcome. Social and Cultural Factors
Institutionalization of the LMIS The combination of political, economic, and sociocultural factors described earlier, as well as the extent of institutional (technical and financial) support for the system, are the prime determinants of whether the transition from donor to host-country government succeeds. In Morocco, broader support for family planning has impacted government; managers within the family planning division are confident of their ability to implement the system and make changes, because they know they will receive the fiscal, administrative, and political support they need. Management personnel and users within the system were able to accept the LMIS as their own project, because they knew they were supported at all levels of the system and that improvements resulting from the LMIS would be valued. This was a motivating factor in their accepting ownership of the LMIS and customizing it on a continual basis so that it met their needs and continued to deliver the results for which it was originally designed. Overall, institutional support in Morocco has allowed the LMIS to flourish and adapt to meet the changing needs of the program and users. Although local funding for LMIS operations appears to be sufficient, one challenge includes planning for procurement of products beyond 2001. Without a continuous supply of products, the system will fail. Another challenge to institutionalization is ensuring that there is sufficient technical expertise to maintain and improve the system ConclusionsThe case study from Morocco demonstrates that even in the most challenging environment an LMIS can be deployed with the full involvement of users and can be made to work. Customizing the system to country-specific situation was a critical factor for ensuring buy-in for the implementation process, and it resulted in visible improvements that were important in promoting adoption by users at all levels. However, significant external support-funding and technical expertise-were also critical components that ensured the initial success of the system. Nonetheless, evidence from the case study demonstrates that, after a system has been implemented, the benefits it provides are not sufficient to ensure its institutionalization. Without institutional support and an enabling environment-manifested by local funding and technical expertise sufficient for maintaining the system-further adaptations of the system by users to meet the program's changing needs may not guarantee the system's continued use and institutionalization. These conclusions suggest several lessons for donor agencies and organizations that provide technical assistance. When donors and implementing agencies decide to invest in deploying a LMIS, the following approach might increase the likelihood of institutionalization, as it is defined in this paper. Before beginning, all key stakeholders should conduct a situational analysis of enabling factors for institutionalization, based on the elements identified in the framework in figure 3. The presence or absence of political will must be assessed and defined for each of the three critical elements in the framework: local funding, system performance, and local expertise. If there is little evidence of political support for the introduction and use of a LMIS to improve decision making, donors and implementing agencies are unlikely to make progress with any enduring effect. However, if there is political support for deploying the system, but not necessarily for funding or staffing, implementing an LMIS can be a starting point, which can be followed by efforts to build support for funding and technical resources. Based on the analysis, the subsequent process of designing and implementing the system should be accom panied by advocacy efforts aimed at ensuring institutional support at higher levels and strategies to ensure security of sufficient funding and appropriate technical resources. In other words, donors and implementing agencies should work together to ensure the presence of all factors necessary for ensuring institutionalization. Donors should focus their efforts on the area in which they have a relative advantage, namely, ensuring institutional support at higher levels by securing a long-term commitment of funds. Implementing agencies' relative strength lies in deploying a well-functioning system that meets local needs, developing the local capacity to manage the system, and building support for the system at all levels. In considering the inability of many countries to fully fund health service costs for preventive products, however, donor agencies and host country governments might begin to think of new ways to define institutionalization. Given a willingness to reconsider definitions of institutionalization, donors and host country governments can go a step further and look at institutionalization as a process by distinguishing short- and medium-term goals from long-term goals. In the short- and medium-term, institutionalizing an LMIS might be defined as deploying a well-functioning system that is routinely maintained and adapted by local technical expertise, but may not necessarily involve financial independence from donors. As an example, Nepal is considered to have a well-institutionalized LMIS, but is dependent on donor funding to continue.16 The donor pays to operate the computerized LMIS, print some forms, and part of the training, while the Ministry of Health pays staff costs for attending the training, completing and submitting the LMIS forms, and using the data for decision making. In the long-term, however, an LMIS may need to be financially sustainable to be considered institutionalized. Donors and implementing agencies might have a better chance of achieving long-term goals of reducing dependency by public sector programs if they define institutionalization as an incremental process, in which system adoption and local ownership must precede financial sustainability. This would allow donors to better target initial resources and planning efforts on achieving the two short-term goals while building advocacy and developing new collaborative mechanisms to enable host country governments to achieve long-term financial sustainability. REFERENCES
ACKNOWLEDGEMENTS We wish to thank Marcelino Barcena of the Department of Health/Philippines; El Khedri Ali and Oucherif Brahim of the Ministry of Health/Morocco; David Alt and Tita Nepomuceno of John Snow, Inc./Philippines; and Shyam Lama, Kieran McGregor, Gary Steele, and Edward Wilson, of John Snow, Inc./Arlington for their valuable information, without which this paper would not be possible. We would also like to thank Bill Felling, Tony Hudgins, Richard Owens, and Leslie Rock of John Snow, Inc./ Arlington whose input and review of the paper was extremely helpful. Last, but not least, we would like to thank our technical writer, Pamela Cubberly of Cubberly & Associates; and our editor, Pat Shawkey; and our graphics designer, Gus Osorio, of John Snow, Inc./Arlington, for putting the paper in its final form. DELIVER, a five-year worldwide technical assistance support contract, is funded by the Contraceptives and Logistics Management Division (CLM) in the Center for Population, Health and Nutrition of the Bureau for Global Programs, Field Support and Research of the U.S. Agency for International Development (USAID). Implemented by John Snow, Inc. (JSI), (contract no. HRN-C-00-00-00010-00), and subcontractors (Manoff Group, Program for Appropriate Technology in Health [PATH], Social Sectors Development Strategies, Inc., and Synaxis, Inc.), DELIVER strengthens the supply chains of health and family planning programs in developing countries to ensure the availability of critical health products for customers. DELIVER also provides technical management and analysis of USAID's central commodity management information system (NEWVERN). This document does not necessarily represent the views or opinions of USAID. It may be reproduced if credit is given to DELIVER/John Snow, Inc. and permission obtained from Africa Health Sciences.
Copyright 2001 - Makerere Medical School, Uganda |

{kind=link}
{kind=link}
{kind=link}
{kind=link}