 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 1, No. 1, December, 2001, pp. 90-96 Biovailability and stability of erythromycin delayed release tablets 1Sydney Ogwal* and 2Xide T.U 1Department of pharmacy, Faculty of Medicine, Makerere University P. O. Box 7072 Kampala Uganda *Author Correspondence: Sydney Ogwal, Department of Pharmacy, Faculty of Medicine, Makerere University, P. O. Box 7072 Kampala, Uganda. Fax: 256(41)532389; Tel: 256-770601127. E-mail: sidneyogwal@hotmail.com Code Number: hs01024 ABSTRACT Background
INTRODUCTION Erythromycin is a typical representative of the macrolide group of antibiotics and is produced by Streptomyces erythreas. Clinically it is widely used in the treatment and prevention of diseases. Like penicillin G it is a broad spectrum antibiotic and it is effective against most gram negative and positive bacteria compared to other antibiotics. The side-effects are relatively low1. Current indications for the drug include: respiratory infections, whooping cough, Legionnaires disease and Campylobacter enteritis. Erythromycin is also known to be active against penicillin resistant staphlococcus,chlamydia and mycoplasma. Erythromycin base is a white, bitter, crystalline substance that is poorly soluble in water. It is a weak basetion by stomach acid and this culminates in decreased absorption following exposure to gastric secretions. Modifications of the drug and its product formulations have attempted to improve absorption and subsequent serum levels by two methods. One involves providing a protective enteric coating to shield erythromycin base from acid degradation in the upper-gastro-intestinal tract. The other involves altering the chemical structure of erythromycin molecule itself to decrease acid inactivation. In the twentieth century in 1960’s came enteric-coated dosage forms and in the 1970’s it became widely used clinically3. Biovailability study measures the extent and rate of drug absorption in the body. Blood or urine samples of subjects are normally used as an index to determine biovailability. The area under the concentration time curve is calculated using Latin square method or trapezoidal rule. AUC o-∞=AUCo-t + Ct/K. The following factors should be considered when evaluating drug product for biovailability studies.4 The drug substance in each product must be the same and for relative biovailability two brands or two dosage forms of the same drug must be compared. For absolute biovailability the AUC value of the product under study must be compared with AUC value of intravenous administration of the same product. The subjects should be healthy with normal liver and kidney functions. Biochemical and medical examination should be used to confirm their medical state. Informed consent should be obtained from each volunteer. Elderly patients and young children should be excluded from the study because age has significant effect on pharmacokinetics. In fact subjects should be of the age of 18 to 35 years. They should be of normal weights because in overweight subjects the apparent volume of distribution maybe somewhat different. Smokers should be excluded because cigarettes can alter the kinetics of the drug under study and the number of subjects should be 10-20 sufficient for the investigator to see any real differences in biovailability (probably 20% variation). The assay method should be the same for all phases of study and complete cross over design should be used. Each subject should receive all the products with a wash out period between each dose administration. In most countries, including Uganda erythromycin appears in the following dosage forms: enteric coated tablets, capsules, suspensions, powders, suppositories, ointments and injections. Currently there are no erythromycin delayed release tablets on the market. The aim of the study was to design erythromycin delayed release tablets and increase their stability in the stomach, so that they have an effective therapeutic action. We also sought to carry out biovailability studies to establish whether delayed release tablets meet the Bioequivalent requirement for the market. MATERIALS AND METHODS2HENJIANG Pharmaceutical Factory, Peoples Republic of China, provided erythromycin base powder. The bromocresol purple used was from Nanjing Chemical Reagents and Company and was of analytical grade. The various reagents and chemicals used conformed to the standard, of the Chinese Pharmacopoeia4. InstrumentationThe dissolution tester employed was a ZRS-4 model supplied by Tianjin University Electronic factory. Shanghai Analytical instruments Factory supplied the 751-G model spectrophotometer used. Formula and preparation of erythromycin delayed release tablet is shown below
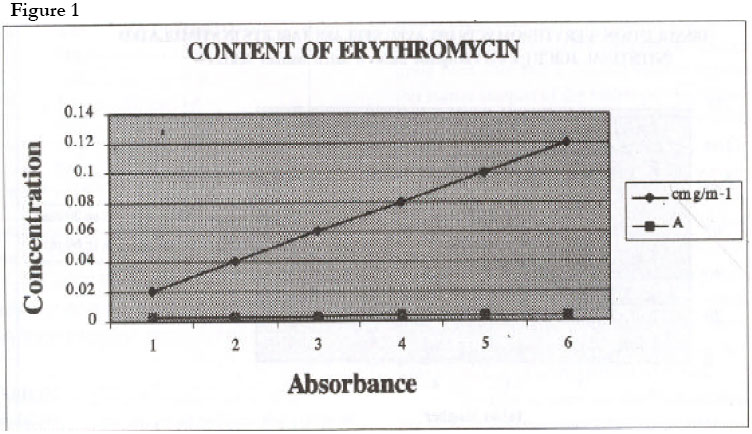
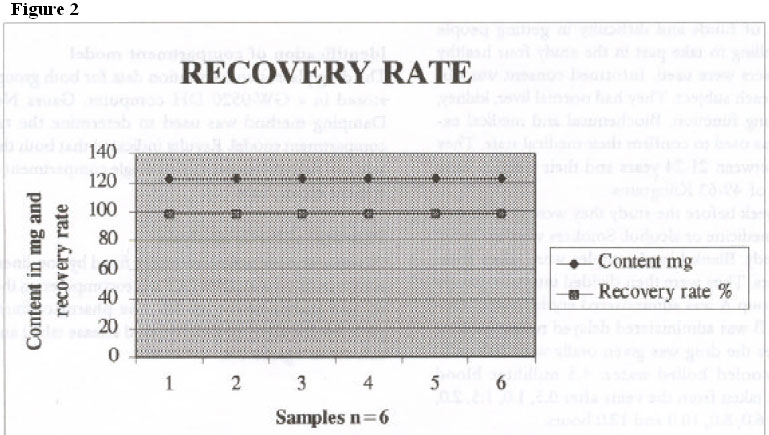
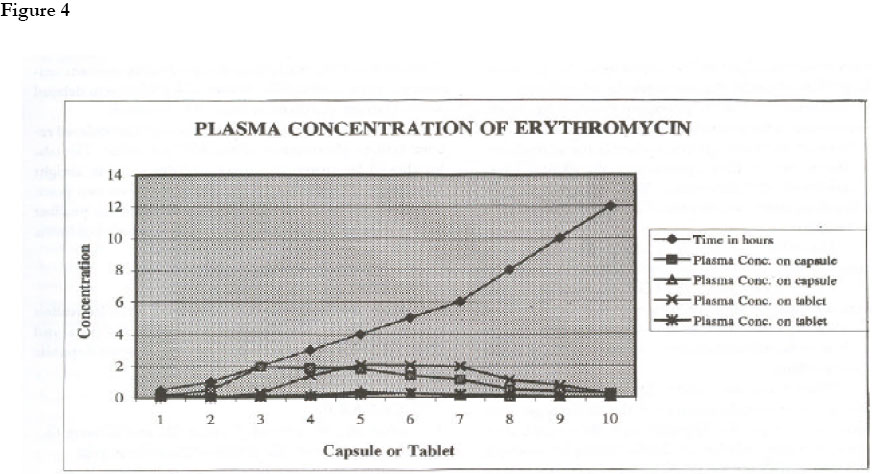
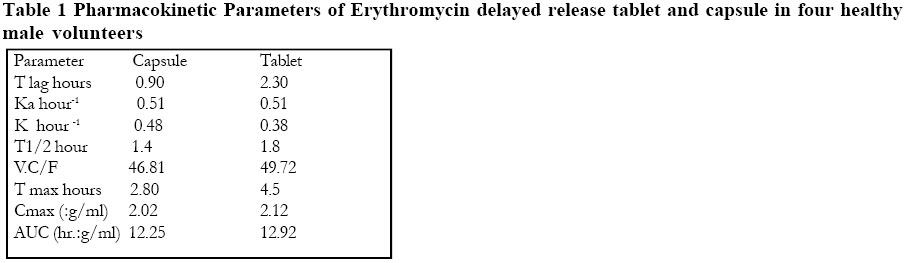
The active ingredient and excipient II and I was weighed accurately and mixed uniformly. The binder was added to form wet granules and screened through a 20-mesh screen. It was dried at 50oC for one hour. The dry granules were screened through an 18-mesh screen. Magnesium stearate was added and compressed into tablet. The tablet hardness was over 8.0 kg and weight 0.17 grams. Coating procedureEudragit No. 2 2.0 g The coating pen was heated to about 40oC and the tablets were put in the coating pan and sprayed. The tablets were allowed to absorb hot air for 1-2 minutes, and then dried using hot air for 5-10 minutes at 60oC. This procedure was repeated 8-10 times. The dried tablets were then placed in a dissector. As a precaution, we made sure that the tablets were relatively hard before coating and that they had a smooth appearance. We also made sure that the temperature was neither too high nor too low, since high temperatures lead to the coatings drying too fast and the coatings would not be uniform. When the temperatures are too low the coatings dry too slow and may form a sticky chain. Determination of dissolution ratePreparation of standard solution 1. Determination of absorbency value of standard solution. 2. Determination of absorbency value of sample. Selection of wavelength Standard Curve The following volumes (0.5, 1.0, 1.5 2.0, 2.5 3.0 mls) were pipetted into a 10 ml volumetric flask. one ml of bromocresol purple and 3.0 mls of hydrochloric acid were added. Glacial acetic acid was used to top each to volume. It was shaken and allowed to stand still for 10 minutes. The absorbency was determined at 480nm. Determination of recoveryOn the basis of the formula and the amount of excipients, contained in one tablet, erythromycin powder and the other excipients were weighed accurately into a 100ml volumetric flask. It was dissolved using anhydrous ethanol and diluted to volume. The solution was shaken vigorously and filtered. Ten mls of the filtrate were measured accurately into a 50 millilitre volumetric flask, and glacial acetic acid added to volume. One ml was pipetted into a 10mls volumetric flask 1.0mls of bromocresol purple indicator, and 3.0mls of hydrochloric acid was also added. It was shaken and allowed to standstill for 10 minutes. At wavelength 480nm the absorbency was determined. The recovery rate was calculated from the correlation equation Dosage stability The tablets were placed in high temperatures (40oC, 60oC and 80o C) high humidity relative humidity 75% and 92.98% strong light (2650 lux) for 10 days. The stability indices examined included appearance, content of the active ingredient, dissolution percentage, pH, and presence of any impurity. A part from at 65o C, 80o C the tablet surface became very dry, and high humidity, the tablet surface became wet and there was no obvious change in the content of the active ingredient and dissolution rate. No impurity was discovered after examination using Thin Layer Chromatographic method. In strong light the tablet pH increased from 8.10 to 8.30. However in all other cases there was no obvious change. Product accelerated test showed no change in the tablet appearance, content of the active ingredient; dissolution rate, pH value and no impurities were detected after Thin Layer Chromatography examination. Determination of relative biovailability of erythromycin delayed release tablets: Drug plasma concentration was used as an index to determine relative biovailability. Erythromycin capsule (250 milligrams batch number 9501204) used as the reference standard. Erythromycin delayed release tablets (125 milligrams batch number 96030116) were used as the sample. The chromatographic column used was Spherisorb C18 10mm 4.6 *250 mm. The mobile phase was water: 0.2 % methanol. Acetronitrile 55:10:25. Sodium hydroxide was used to adjust the pH to 5.8. The flow rate was 1.0 milliliter/minute. Determination of erythromycin plasma concentration Due to lack of funds and difficulty in getting people who were willing to take part in the study four healthy male volunteers were used. Informed consent was obtained from each subject. They had normal liver, kidney, heart, and lung function. Biochemical and medical examination was used to confirm their medical state. They were aged between 21-24 years and their weights were in the range of 49-63 Kilograms. A week before the study they were not allowed to take any medicine or alcohol. Smokers were excluded from the study. Blank blood samples were taken from the volunteers. They were then divided into two groups A and B. Group A was administered erythromycin capsule. Group B was administered delayed release tablets. In both cases the drug was given orally with 200 millimeters of cooled boiled water. 4.5 milliliter blood samples was taken from the veins after 0.5, 1.0, 1.5, 2.0, 3.0, 4.0, 5.0, 6.0, 8.0, 10.0 and 12.0 hours. RESULTS Figure 1The samples were centrifuged at 3000 revolutions per minute to extract plasma. Identification of compartment modelThe drug plasma concentration data for both groups was stored in a GW-0520 DH computer. Gauss Newton Damping method was used to determine the type of compartment model. Results indicated that both the capsule and delayed release tablets single compartment model is most appropriate. Pharmacokinetic analysisPharmacokinetic parameters were fitted by non-linear least square method with IBM/XT microcomputer on the basis of one compartment model. The pharmacokinetic parameters for erythromycin delayed release tablet and capsule are in figure 1, figure 2, figure 3, figure 4. Table 1 Pharmacokinetic Parameters of Erythromycin delayed release tablet and capsule in four healthy male volunteers The equation used for calculation was percentage
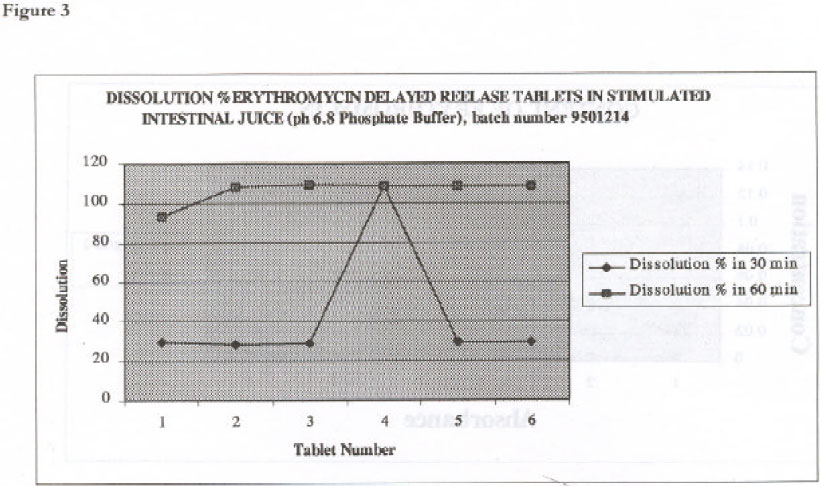
dissolution = A/0.2778 * Results indicated that both the capsule and delayed release tablets single compartment model is most appropriate. DISCUSSIONThe biovailability results are good because the scope of biovailability is between 80-150%. However the study was only carried out in four subjects. More studies should be done using ten to twenty volunteers in order to check for possible variations in pharmacokinetic and biopharmaceutic parameters. Unfortunately the effect of the factors that normally affect Biovailability such food, dairy product and fats were not studied and could have affected the results. However, all other requirements of biovailability studies were met. In the development of the new delayed release formulation, there were two critical points. First, it was necessary to ensure that the compressed tablets had a relatively hard core and a smooth elegant appearance. For this reason samples of the tablets produced were assessed for their hardness and only batches with a hardness value of ≥ 8kg were used for the next stage which involved application of an enteric coating to the compressed tablets. Secondly, the coating parameter especially the temperatures needed to be controlled to a very narrow range of around 40oC ± 0.5. This is because when the temperatures are too high, the coatings would dry very fast leading to the formation of a non-uniform coating. However, if the temperatures fell to relatively lower values, the drying process would be slowed significantly with possible formation of a sticky mess of tablets. In order to carry out studies involving quantitative assays, it was necessary to select an appropriate wavelength at which absorbencies from different samples would be assessed The scanning of a methanolic erythromycin standard solution (0.1mg ml-1) indicated that the maximum absorbency for the drug is 480nm. When the scan was carried out on a sample of powdered tablets, it was observed that the excipients did not interference with the spectrum of maximum absorbency identified earlier. The drug showed a linear response over the concentration range 2-12 x 10-2mg ml-1 (that is 20 -120μg ml-1). In the dissolution studies, measurement of erythromycin in simulated gastric juice indicated that there was no drug released under these conditions after 60min. This confirms to the USP requirement that Erythromycin delayed release tablet preparations must be resistant to the breakdown by the acidic gastric contents for at least one hour. This allows the drug to move into the alkaline intestinal medium when taken orally. This arrangement protects the drug from inactivation through degradation in acidic medium2 The release of the drug in simulated intestinal medium (Tablet 1) after 60 min was 105%. This was far above the 70% specified by the USP. This indicates that the new formulation meet pharmacopoeial requirements and in addition, the new excipients II and I permitted the entire drug to be released once it has reached the alkaline intestinal medium. When the tablet surface became wet, there was no obvious change in the content of the active ingredient and dissolution rate. No impurity was discovered after examination using Thin Layer Chromatographic method. In strong light the tablet pH increased from 8.10 to 8.30. However in all other cases there was no obvious change. Product accelerated test showed no change in the tablet appearance, content of the active ingredient; dissolution rate, pH value and no impurities were detected after Thin Layer Chromatography examination. The results indicate that the absorbency of the standard solution was 0.302 (n=6). This is a clear indication that the tablets were of uniform size and had good quality. CONCLUSIONSThe results of the study have shown that the content uniformity, appearance, dissolution of erythromycin delayed release tablets conform to the U.S.P standards. The stability experiment showed that delayed release tablets when stored below 40oC are stable. The tablet should be stored in a cool and dry place in airtight containers. The shelf life is temporarily given two years. When administered to four healthy subjects, the product gave a relative biovailability of 105.31% which conforms to USP standards. ACKNOWLEDGEMENTThis study was supported by funds from State Education Commission of the Peoples Republic of China and 2HENJIANG Pharmaceutical Factory, Peoples Republic of China. REFERENCES
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}