 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
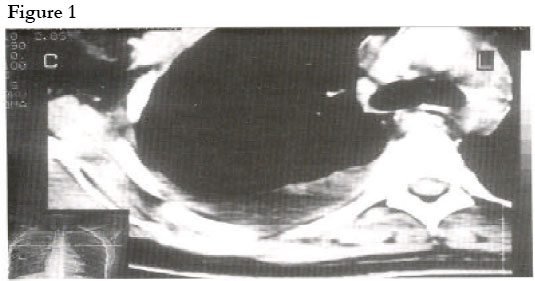
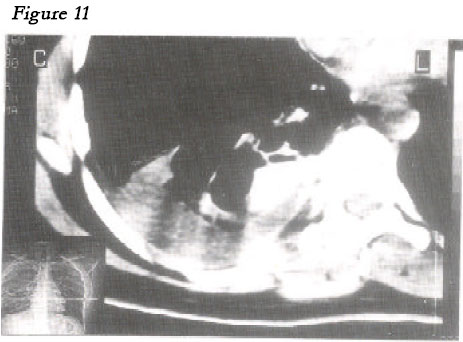
African Health Sciences, Vol. 1, No. 1, December, 2001, pp. 97-98 CASE REPORTS Menstruation in an unsual place: A case of thoracic endometriosis in Kampala, Uganda 1Rosemary Kusaba Byanyima Correspondence: Rosemary Kusaba Byanyima, Department of Radiology, Faculty of Medicine, Makerere University, P. O. Box 7072 Kampola, Uganda, Tel: 256(41)530137, E-mail: r_byanyima@hotmail.com Code Number: hs01025 ABSTRACT: While pelvic endometriosis is relatively common, thoracic menstruation is rare. A report of what is believed to be the first case of thoracic endometriosis in Uganda is given. A 34 year old female was complaining of on and off chest pain mainly on the right side. Clinically she had signs of pleural effusion and 500 mls of altered blood were tapped from her right pleural space. Worried about a possibility of a malignant process, an urgent chest CT scan was performed. A right posterior pleural mass and pleural effusion were found. A pleural biospy was taken and confirmed at histology as endometrial tissue. She did well on surgical excision and hormonal therapy. This was a rare case of endometriosis which shows the usefulness of imaging in the patient work up. CASE REPORT A 34 year old female presented in a Kampala private clinic complaining of recurrent right sided chest pain for an unspecified period. She gave no history of fever or haemoptysis. She was nulliparous but her menses were regular. General examination was normal. On systemic examination significant findings were signs of right sided pleural effusion. An anterio-posterior chest X-ray confirmed the clinical suspicion of the right pleural effusion. Five hundred millilitres of altered blood were aspirated from the right pleural space. Her haemoglobin level was 13.3 mg/dl, ESR 15 mm (Westergren in first hour) and the prothrombin time was normal. A chest CT scan was performed a week later (Figure I, II). A right pleural soft tissue mass with irregular outline located at the level of the angle of the 10th rib was seen. It measured 40 x 15 x 20 mm in size, enhanced moderately and homogeneously with contrast, and there was no evidence of rib destruction. There was a moderate right pleural effusion. The lung parenchyma, hila and mediastinal structures were normal. A radiological diagnosis of malignant mesothelioma was made although there was no history of asbestos exposure as far as the patient could remember Biospsy of this lesion and histology confirmed the diagnosis of endometriosis but from the CT findings an impression of malignant mesothelioma had been made although no history of asbestos exposure was present. A combination of surgical excision of the endometrical plug and hormonal therapy were used and the patient is doing well. DISCUSSIONThere are so far three accepted postulates of the mechanism of endometriosis. (1,2,3,4,5,6) The first is retrograde menstruation, which explains only pelvic endometriosis. The second is of serosal cells metaplasia. Here the remnants of the Muellerian ducts with its coelomic cells retain their potential to differentiate into endometrial tissue. This postulate explains pelvic, peritoneal and limb bud endometriosis. The third postulate is vascular and lymphatic embolisation, which explains endometriosis in distant sites like in this patient. Ectopic endomentrium is oestrogen dependent too and cyclic symptoms are common although in this patient the symptoms were not cyclic. This explains why she first visited a physician and not a gynaecologist. Thoracic endometriosis is very rare. (6,7,8) The radiologists in Uganda with sophisticated equipment like CT can carry out guided biopsy for histological diagnosis but because of the high index of suspicion of mesothelioma a scope of the pleural space was preferred for this patient. Pelvic endometriosis is the commonest site of endometriosis and like pelvic inflammatory disease causes adhesions that carry grave complications such as like infertility and ectopic pregnancies Medical therapy and surgical excision are equally effective modes of treatment for this condition. ACKNOWLEDGEMENTTo the patient who kept me informed of her progress and Dr. Jolly Beyeza for the literature. REFERENCES
Copyright 2001 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs01025f1.jpg] [hs01025f2.jpg] |
| |||||||||

{kind=link}
{kind=link}