 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 2, No. 1, April, 2002, pp. 24-28 Isolations of Bwamba virus from south central Uganda and north eastern Tanzania
Julius J. Lutwama, Elly B. Rwaguma, Peter L. Nawanga and Anthony Mukuye
Department of Arbovirology, and Emerging and Re-emerging Viral
Infections, Uganda Virus Research Institute, P.O. Box 49, Entebbe, Uganda.
Code Number: hs02032 ABSTRACT Background: Bwamba virus (Genus Bunyavirus, family
Bunyaviridae) is widely distributed in Africa. It causes many unidentified
fevers because of its benign nature.
INTRODUCTION
Bwamba virus (BWA) is a member of the Bunyamwera serogroup, Bwamba virus antigenic group, in the Genus Bunyavirus, family Bunyaviridae.1-3 Bwamba virus is an arthropod borne virus transmitted by mosquitoes, including Anopheles gambiae Giles, Anopheles funestus Giles, Aedes furcifer Edwards, Aedes (Neomelanoconion) spp., Anopheles coustani Laveran, and Mansonia uniformis Theobald.4-6 The principal anthropophilic vector species are Anopheles funestus and Anopheles gambiae.7 Bwamba fever was first encountered as a clinical entity in 1937 among construction workers on a new road to Bwamba County, Western Uganda (now called Bundibugyo District). Nine patients yielded identical viruses and developed antibodies during a small epidemic outbreak of the disease.8 The etiological relationship of the virus to the disease was conclusively demonstrated by the development of specific neutralizing antibody in the serum of each virus donor with convalescence. Bwamba infection has since been recognised by virus isolations from humans in Nigeria, 9 Cameroon, 10 Central African Republic, 11, 12 Kenya, Tanzania, 8 and South Africa.13 The disease presents as a relatively severe form of generalised infection of brief duration (4-5 days), 8 and benign nature; no fatalities are recorded so far. Exanthem is nearly always present and is frequently associated with meningeal involvement. It is usually accompanied with fever, headache, arthralgia, and pains of generalised or local distribution. Intestinal tract involvement, especially diarrhea, is also seen.7 Some patients may also develop a body rash. Convalescence is characterised by marked asthenia lasting 8 to 10 days. Viremia, in humans, is usually of short duration (24 - 48 hrs) making isolation of the virus difficult. Because Bwamba virus does not generally cause epidemics, it has a limited recognised social and economic impact. Nevertheless, it is widely distributed in tropical Africa.7 Results of samples of serum from 615 residents of various localities in Uganda and Tanzania that were tested for their capacity to neutralize Bwamba fever virus indicated that the disease was very prevalent in both Uganda and Tanzania. The results also indicated that the virus attacks children and adults with approximately equal frequency. Other studies have indicated that antibodies against the virus are distributed as far south as the Republic of South Africa and as far north westwards as Gambia.13 The virus appears to be endemic in Uganda, Tanzania, and Mozambique.13, 14 It also appears to be the tenth most frequent arthropod borne virus infecting humans in the African continent.15Antibodies to Bwamba virus have been found in birds, 4,14 monkeys, 16 and donkeys.14 Routine surveillance of arboviruses in Uganda, in the past, enabled isolation of the virus on several other occasions17 but for more than one and a half decades, no isolation of Bwamba virus have been made until these herein reported.
MATERIALS AND METHODS
Isolate No. I (SG372): In late May 1994, MSF (Medicine Without Frontiers group of volunteer doctors from Holland) reported a suspected outbreak of haemorrhagic fever in Rwandese refugees in Burigi Camp, Ngara, in northeastern Tanzania. Clotted blood samples from 5 out of 14 suspected cases, aged 9 and above, mostly adults were received at Uganda Virus Research Institute, Entebbe, Uganda. Clinical presentation of the patients was low persistent fever, bleeding from nose and gums, jaundice, enlarged liver and spleen, and very dark urine and faeces. Initial treatment was for suspected malaria but none responded to chloroquine, or to penicillin. All 14 cases died within 2 weeks. There was convulsion before death in all the cases. Serum from the 5 blood samples was diluted (10%) in phosphate buffered saline (pH 7.4) with 5% bovine albumin (PBS). Aliquots (2 µl) were inoculated into the brain of (i-c) into suckling baby mice which were then observed daily for 14 days. First signs of sickness were observed on day 7 post-inoculation, and sick mice were collected and frozen at -80°C. Only 1out of the 5 Rwandese serum specimens caused sickness in mice over 3 weeks of observation. Brains of the sick mice were harvested, and a 10% suspension in PBS was filtered through a 0.20-micron cellulose-acetate membrane disposable sterile syringe filter, and used for the first passage. Sickness was again noted on day 7 at the second passage and on day 4 at the sixth passage. Whole mouse carcasses from the fifth passage were frozen in liquid nitrogen and sent to the National Center for Infectious Diseases, Centers for Disease Control and Prevention (CDC), Fort Collins, Colorado, USA., together with aliquots of the original 5 Rwandese sera for further identification. Isolate No. 2 (SG 383): On October 5, 1994 one adult, male, a member of the Uganda Virus Research Institute staff, working with the Rakai Project, in Rakai district in south western Uganda, reported to the Institute clinic in Entebbe, complaining of fever, headache, backache and muscle pain, particularly in the neck region. He had used chloroquine and some antibiotics without any improvement in his condition. The initial treatment was of suspected malaria. He reported to have contracted the disease most likely in Rakai district about a week before reporting to the clinic. A blood sample was collected from him for examination. No malaria parasites were identified by microscope examination of blood slides. Aliquots of the serum were diluted as for isolate No. I, and inoculated ic into suckling baby mice which were observed daily for 3 weeks. The first signs of sickness were observed on day 4, and death of some of the inoculated mice on day 5 post-inoculation. Sick mice were collected and frozen at 80°C. Brains were harvested from the sick mice and a 10% suspension in PBS was filtered and used for the first passage. Sickness was again noted on day 4 post-inoculation. At the fourth passage, sickness in mice was first observed on day 2, and the virus killed mice on day 3. Like for the first isolate, whole mouse carcasses from the third passage were sent to the National Center for Infectious Diseases, Centers for Disease Control and Prevention (CDC), Fort Collins, Colorado, USA, together with an aliquot of the original serum for further identification. The infective agent was identified by immunofluorescence assay (IFA) tests. Examination by fluorescence microscopy indicated positive reactivity of the viral isolates with the Polyvalent Bwamba fluid (this grouping fluid includes BWA, Eret. 147, KAM, MOS, NDO and PGA monoclonal antibodies). Additional tests using specific monoclonal hyperimmune antibody fluids (viral type specific MHIAF) were performed. The antigen was found to react when using the BWA virus monoclonal antibody fluid. Further definitive identification of the isolates was made by carrying out plaque reduction neutralization tests (PRNT). A plaque is a localized focus of virus-infected cells. Enumeration of these foci is a quantitative method for assay of viral infectivity. If antibodies against a particular virus are present, virus cannot attach to cells and infectivity is blocked (this is called neutralization). The neutralization of viral infectivity is the most sensitive and specific method for determining the identity of an isolate. To identify viral isolates, antisera of known reactivity are employed. In this study antisera of Bwamba and Pongola viruses were used. Bwamba and Pongola viruses are antigenically related and thus, are cross-reactive in IFA tests. Antisera was diluted 1:5 in BA-1 diluent and then successively in two fold dilutions to 1: 5120. The virus was diluted in BA-1 with 8% fresh human serun added to provide exogenous complement. The viral dilution was made to provide 200 plaque-forming units (PFU) per100 µl of the solution. The fresh serum was pretested and found free of antibodies against Bwamba and Pongola viruses. Equal volumes of the dilutions of the antisera and the test virus (100 µl of virus to 100 µl of each antisera dilution) were mixed and incubated at 37oC for 1 hr to permit virus antibody interaction. As a control, the test virus was mixed with an equal volume of maintenance medium (1 x M199 with 5% feotal calf serum). This control indicated the infectious dose of the virus actually present in the test dilution. 100 µl of virus-antisera mixtures were inoculated per well on six-well plates containing a monolayer of Vero culture cells, each well taking a different dilution of the antisera. One of the wells received the control mixture. The mixture was adsorbed onto the cell monolayer at 37oC for 1 hr in a CO2 incubator, rocking after 30 minutes. Using a pipette, an overlay of nutrient agar (3 ml) at 42oC was added to each well and left on the bench to set. After setting the plates were inverted and incubated at 37oC in a CO2 incubator for 7 days. On day 7, a second overlay of nutrient agar (2.5 ml) containing neutral red stain (500 µl 1% neutral red added to 100 ml of overlay) was added to the plates. The counting of plaques started the following day and continued for a week. Reciprocal tests comparing each isolate with the prototype strain of BWA virus (strain M459) and of Pongola virus (strain SAAr1), and their antibodies were carried out. The neutralizing activity was determined by its ability to reduce the number of virus plaques as compared with the number seen in control cultures. The highest antisera dilutions inhibiting 90% of the infectious virus dose compared to the control wells determined the end point. Stock viruses were prepared as 10% suckling mice suspensions in PBS (pH 7.4 with 4% bovine albumin). Isolate No. 3: Between mid-1996 and mid-1997 there was an outbreak of O’nyong-nyong virus fever epidemic in Rakai district in south-central Uganda. The entomological studies that were carried out yielded 10,050 mosquitoes of different species. On processing these mosquitoes for virus isolation, Bwamba virus was isolated from a pool of 50 Anopheles funestus mosquitoes. (Details of the isolation and confirmatory tests are given in Lutwama et al,.18
RESULTS
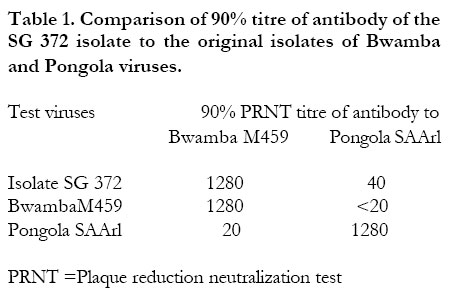
The identification studies using serological methods showed that the two virus isolates (SG 372 and SG 383) were of Bwamba virus (BWA). The results of one-way neutralization assays using the plaque-reduction neutralization test (PRNT) comparing isolate No. I (SG 372) and the original isolates of Bwamba virus (M459) and Pongola virus (SAAr1) are presented in Table 1 . Isolate SG 372 gave a high titre similar to the homologous Bwamba virus (M459) titre. The titre was the reciprocal of the highest dilution giving more than 90% neutralization. This indicated that the isolate was of Bwamba virus. The titre for Pongola-virus when compared to isolate SG 372 was five folds lower than the homologous titre for Pongola virus (SAAr1). Isolate SG 372 was retested with isolate SG 383 comparing them to the original Bwamba virus isolates (M459) and Pongola virus isolate SAArl again using the PRNT after 5 days of infection of Vero cells growing on 6 well plates. The results of one-way neutralization assays using the plaque-reduction neutralization test (PRNT) comparing isolates SG 372 and SG 383 with the original isolates of Bwamba virus (M459) and Pongola virus (SAAr1) are presented in Table 2 . The titres for isolates SG 372 and SG 383 when compared to the original Bwamba virus were three folds higher than when compared to the original Pongola virus.
DISCUSSION
Since the 1937 outbreak of Bwamba fever in a moderate epidemic in Bwamba, Uganda, no further large outbreaks of the disease have been recognized. The last confirmed isolate of BWA in Uganda was made some time in the 1980s. Bwamba virus fever is usually mistaken for malaria and is usually treated as such. In a number of cases it occurs concurrently with malaria. All blood samples obtained from the Rwandese refugees were highly positive for malaria parasites. All the cases were first treated as malaria but on failure of malaria treatment it was realized that it could be a different infection. Since some of the vectors that transmit BWA also transmit malaria, there are many chances of concomitant transmission and infection. Anopheles gambiae s.l. and Anopheles funestus are known also to transmit O’nyong-nyong virus (ONN).19, 20 In a recent ONN epidemic in Rakai, Masaka, Mbarara and Sembabule districts of south-western Uganda (1996-1997) where Anopheles funestus was suspected to be the major vector species 18 there were a number of cases who reported febrile illness. They also at times had a rash but IgM body tests were not positive. 21 Some of these infections could have been cases of BWA viral infections or some other viral diseases. Lutwama et al 18 reported the isolation of BWA and NDO viruses from Anopheles funestus collected during the 1996-1997 ONN epidemic in southwestern Uganda. The donor of the serum from which the second isolate was obtained believes that he was infected while on duty in Rakai district, two years before the beginning of the recent epidemic in that area. Thus there is the likelihood that he was infected in Rakai district where the virus may be circulating and Bwamba fevers may be occurring unnoticed. The natural history of BWA is not very clear. While antibodies against BWA were demonstrated in monkeys and donkeys, the natural reservoir hosts are not known. There may be vertebrate hosts or the vectors themselves may constitute the main reservoirs. In the absence of recent sero-survey data on prevalence of BWA virus, conclusions regarding the significance of these infections are presently impossible for Uganda. Studies need to be carried out to understand the natural history of BWA virus, especially, in light of re-emerging infections. There is a need to know as much as possible about the infections we have presently, such that they do not surprise us in future when they may re-emerge in more dangerous forms.
ACKNOWLEDGEMENTS
We acknowledge the MSF Holland Volunteer doctors who sent the samples from Tanzania. The assistance of Dr. R.G. Downing for receiving the specimens from Tanzania, and sending the virus isolates to Fort Collins USA, is highly appreciated. We express our gratitude to D.J. Gubler, T. Roehrig, N. Karabatsos, B. Cropp, and D. Martin (CDC, Fort Collins, CO) for assistance in laboratory confirmation of the virus diagnosis.
REFERENCES
Copyright 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02032t1.jpg] [hs02032t2.jpg] |
| |||||||||

{kind=link}
{kind=link}