 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 2, No. 1, April, 2002, pp. 29-32 Diverticular disease of the colon in Kampala, Uganda
Elsie Kiguli-Malwadde, Henry Kasozi
Department of Radiotherapy, Faculty of Medicine, P. O. Box 7072
Kampala, Uganda Code Number: hs02033
ABSTRACT
Background: Diverticular disease of the colon has been
reported to be a disease of the western world, however of recent it has been
described in the Africans. INTRODUCTION Diverticular disease of the colon is an acquired disease of adults thought to be rare among the black population. It is often described as a disease of the western world. 1,2,3,4,5 The cause is not known though it has been reported that it occurs due to persistently raised intra-colonic pressure and are associated with constipation. It is also known to be associated with a low residue diet. It has been reported that it was unknown before 1900 and has been associated with food processing and food refinement in industrialized countries 5 . The diverticulae are a pulsion type of mucosal out-pouches not covered by
the muscular layer. They occur mainly in the sigmoid colon and are found
along the sidewalls of the colon at the site of blood vessels’ entry,
which is a site of relative weakness. Other parts of the colon may be also
affected especially on the left side. However diverticula may be found any
where along the colon. Complications of diverticular disease include
diverticulitis, haemorrhage, muscular hypertrophy and obstruction, pericolic
abscesses, perforation and vesico-colic fistula. There is no evidence that
diverticular disease predisposes The main objective was to study the clinical, demographic and radiological features of patients with diverticular disease of the colon in Kampala, Uganda. MATERIALS AND METHODS A retrospective and prospective descriptive study between January1995 to
December 1996, January 1998 – December 2000 was carried out. The
period January1995 to December 1996 was retrospective, while January 1998
– December 2000 was prospective. Thirty-one consecutive patients seen
in two x-ray units and two major hospitals in Kampala with radiological
evidence of diverticular disease were recruited. These units do 540 barium
enemas All the patients had a standard double contrast barium enema. All patients were prepared for at least 3 days before the barium enema. A low residue diet was recommended for 3 days and a cleansing enema was given on the morning of the barium enema. Barium sulphate suspension was introduced into the colon via the rectum from a suspended disposable enema bag up to the mid transverse colon. Air was then introduced and the patient rotated until the entire colon was coated with barium and air. Spot films of the rectum, sigmoid colon, splenic and hepatic flexure were taken. Full-length abdominal films and spot films of the pathological parts were also taken. The films were then examined for features of diverticular disease like flask shaped or rounded pouchings, rounded pools of barium or ring shadows. Muscle changes and other complications were also looked for. All patients seen during the study period were included. Radiological findings and salient clinical data were analysed.
RESULTS
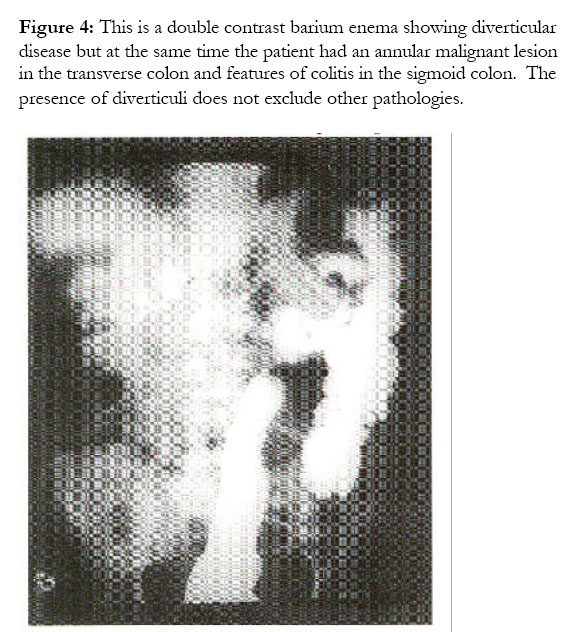
Thirty one cases of diverticular disease were seen during the period January 1995- December 1996, January 1998- December 2000. Sixteen males and 17 females were recruited giving a male to female ratio of 1:1. The age range was 42-80 years, mean age 52 and a median of 60 years. One patient was European, one was a ‘half-caste’ with Caucasian and African heritage, and 10 were Baganda while 8 were from other tribes. The income of the patients was difficult to establish as they all had more than one job. Two patients had had up to primary education, others had had higher education in tertiary level institutions. Only 2 patients came from a rural area, the rest came from urban areas. The main presenting complaints varied from rectal bleeding (13), abdominal pain (12), constipation (7) and abdominal mass (3). Some of the patients presented with more than one complaint. In the prospective study, inquiry into the dietary habits of the patients revealed that all the patients except one had a mixed type of diet with the local foodstuffs as well as low residue foods. The appearances on the barium enemas showed flask shaped outpouchings or ring structures when viewed end on, (Figures 1,2,3). The sigmoid colon was the main part affected followed by the descending, transverse, ascending colon and caecum, 3 patients had diverticular disease throught the whole length of the colon. One patient had a malignant lesion in the transverse colon in addition to diverticular disease. (Figure 4).
DISCUSSION
By 1968 it had been reported that diverticular disease was unknown in the African4 . Recently, however it has been reported that diverticular disease of the colon is on the rise in the African population1. Madiba reported 20 cases in a period of five years in South African blacks1. Ssali reported eight cases in five years in Uganda3 .We now report 31cases in five years. This supports the fact that more cases of diverticular disease are being seen in the African population in Kampala, Uganda. The commonest presentation among these patients was rectal-bleeding. Madiba reported similar findings in South Africa4. In another study in the USA, colonic diverticulum was found to be the commonest cause of lower GIT bleeding7. In the western world, diverticular disease has been noted to be a disease of adults and is found in two thirds of the autopsy population in those aged over 80 years8. However such data is not available for Africans. In the current study all patients were over 40 years and this may suggest that it is predominantly a disease of adults. Madiba reported that women were more affected than men4. However in the current study the males and females were equally affected. The clinical and radiological presentation is similar to what has been reported in the western world2,5,9.. Could it be that diverticular disease is a new entity in our environment or has it been there in silent existence? Is it possible that the Ugandans have adopted a western diet especially those that live in the urban areas. As noted, many supermarkets have sprung up in Kampala recently and these sell processed foods and the middle class frequents them. Ssali3 argued that the diet of the Ugandan middle class only differs from the traditional diet in its protein content in the form of meat, eggs, fish, and milk. In the current study this argument seems to be supported by the fact that most patients still eat a traditional diet. Others could argue that most Ugandans still eat the local diet and so this problem may not be associated with diet. A few of the patients presented have lived in western countries but this was only during their adulthood. It could also be that diverticular disease of the colon has been with us undetected but with improved health care, more patients are being investigated and thus being discovered. After all, barium enemas were not commonly done 20 years ago. The findings at colonoscopy have not been reported but these could also reflect a similar picture. Is diverticular disease in Africa the same as the western type? Based on the clinical and radiological findings of this study, the two diseases seem to be similar.
CONCLUSION
In conclusion, diverticular disease of the colon exists in the African. There is need to increase our index of suspicion for diverticular disease and its complications. If the disease is associated with a low residue diet, then the health system should advise our population to maintain the highresidue African diet. However we cannot exclude a possibility that factors other than diet may be contributing to the rise in prevalence of diverticular disease of the colon in Uganda. Further studies to confirm or support some of these findings are recommended.
REFERENCES
Copyright 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02033f2.jpg] [hs02033f4.jpg] [hs02033f1.jpg] [hs02033f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}