 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 2, No. 1, April, 2002, pp. 33-39 Contraception and sexuality among the youth in Kisumu, Kenya Missie L. Oindo Partnership Department, Tropical Institute of Community Health and
Development (TICH) in Africa P. O. Box 2224 Kisumu, Kenya Code Number: hs02034
ABSTRACT
Background: A significant proportion of youth is infected by
HIV and other sexually transmitted infections mainly through sexual
intercourse, while the prevalence of unwanted pregnancies is rising. INTRODUCTION The youth1 aged 25 years and below constitute 64% of Africa’s
population while one in every Kenyan is an adolsecent2. Often the youth
experience gradual movement towards heterosexual relationships which can lead
to sexual activity. Culture fundamentally affects sexuality and fertility by
creating values, norms, and expectations about sexual relationships, roles
and behaviour3. In most traditional cultural set-ups, both pre-marital sex
and pregnancy A significant number of unmarried youth are becoming sexually active at early ages, prompted by the mass media presentation of sex as exciting and risk-free5. Fifty-two percent of the Kenyan youth aged between 15- 19 years are sexually active6 and specifically 39% and 65% of unmarried Kenyan girls and boys respectively, have had sexual intercourse7. Worldwide, studies on adolescent sexual behaviour show that young people’s premarital sexual encounters are generally unplanned, infrequent and sporadic, a pattern that pre-disposes the youth to unwanted pregnancy and sexually transmitted infections. In sub-Saharan Africa, 7.4% of all 15-24 years aged youth were infected with HIV in 1997, mainly thorough unprotected heterosexual intercourse8, while 600,000 Kenyan youths are projected to become HIV positive9 by the year 2005. Kenya’s teenage births to girls aged 15-19 years account for about 12% of Kenya’s total fertility, while Kisumu district’s adolescent fertility10 is reported at 27%. Many of documented schoolgirl pregnancies end in abortions, and adolescent abortions account for 16.5% of all abortions11. Worse still up to 74% of the women with abortions in Kenyan hospitals are adolescents12. The current conflicting messages about youth sexuality, with the promotion of sexual involvement on one extreme and urging of chastity on the other, make the youth feel guilty, uncertain or indecisive about contraception13. Recent Kenya Demographic and Health Surveys (KDHS) show that less than 10 percent of sexually active unmarried adolescent women aged 15-19 years were using any modern method of contraception14. Consequently, there is a 52 percent unmet need for family planning among married women aged 15-19 years15, a figure bound to increase if unmarried, sexually active teenagers were included. A study of model sex education programmes found that while a variety of programmes were quite effective at increasing teenagers’ level of knowledge of conception and contraception, they had little impact on their behaviour16. The relationship between what adolescents know and how they behave is perhaps the most salient issue. The 1989 Kenya Demographic Health Survey showed that 90.1% of all women in the survey knew at least one contraception method, and that never-married women were least likely to know any method as compared to the currently married17. Other factors strongly associated with contraceptive use by sexually active unmarried teenagers include age of initiation, having a stable relationship with a sexual partner, knowledge of reproduction and contraception, acceptance of one’s own sexuality, academic aspirations and parental support and controls18. For example, the older the girl at the time of initiation of sexual activity, the more likely she is to use contraception regularly and use a modern method, primarily the pill19. Younger girls, on the other hand, are more likely to be never-users, sporadic and ineffective contraceptors, and more likely to rely on male methods20. Presently, many parents are uncomfortable discussing sexuality and contraception with their children, a role that has been left to schools already limited by the current debates on sex education21. Until very recently, reproductive health (RH) services in most developing countries have been influenced by political factors rather than by meaningful state or national planning to meet the needs of the masses14. The widespread moral and political disagreements about the adolescent pregnancy problem have created confusion and conflict over what to do about it, resulting in absent or unclear guidelines on adolescent RH issues, including contraception. Even where there are no legal barriers, service providers are not always receptive to young clients and there is a minority who believe contraception is foreign to the culture and that it promotes promiscuity22. Given the youth’s knowledge level on prevention and control of risks of unwanted pregnancies and STIs/ HIV infections, there is concern over their continued unsafe sexual practices and the associated morbidity. Therefore this paper describes the sexual and contraceptive knowledge, attitude and the factors influencing practice among the youths of Kisumu town in western Kenya. It also discusses the social and policy context of youth contraception in urban Kenya.
METHODS
A semi-structured questionnaire was applied to a total of 388 respondents (48.2% males and 51.8% females) aged 15-24 years selected through simple random cluster sampling. The instrument examined respondents’ background factors; knowledge of contraceptive services and service sources; contraceptive attitude; contraceptive practice; and aspects of sexuality. Data was analysed using the SPSS computer software package. Twelve Key Informant Interviews with parents, guardians, policy makers and health service were conducted through interview guides and focused on youth sexual and RH problems; adult attitude and communication on youth sexuality and contraception; and national and institutional policies on youth contraception. Six informal conversational interviews with parents, guardians, local administration and the youth focused on societal attitudes towards youth sexuality and contraception. RESULTS
Background characteristics
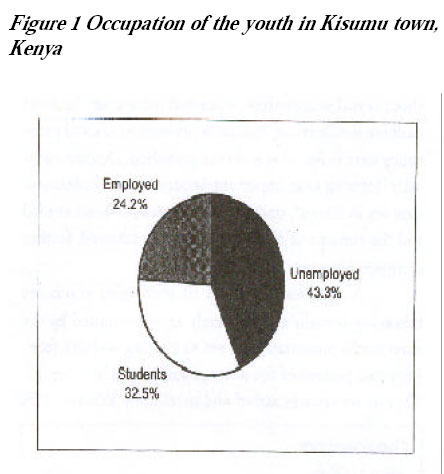
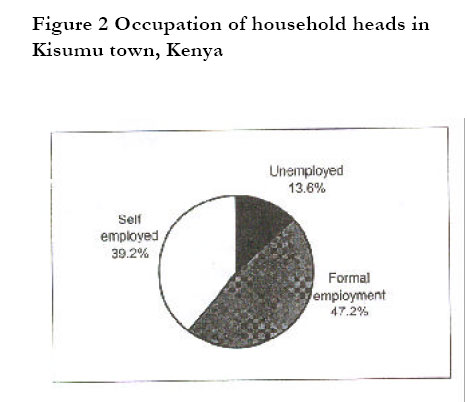
The mean age of the sample population was 19.5 years. Over 83% were single, 10.4% of these reporting a parity of 1-2 children. Mean age at first marriage was 19.9 years, with 65.1% of the ever-married being female and reporting lower ages at first marriage than males. The occupation of the youth and the household heads are shown in Figures 1 and 2.
Knowledge of contraceptive services and service sources
There was a 99.2% level of knowledge of at least one contraceptive among the youth (99.5% for males and 99% for females). Main sources of this knowledge were educational institutions, media and peers. Many parents/ guardians reported reluctance to discuss sexuality with their ‘in-the-family’ youth as opposed to other youth within formal educational and health institutions. The level of knowledge of other contraceptive services, namely information and counselling, was 14.7% and this increased with age. However, there was no significant correlation between age and number of contraceptive service sources known. The most common service source identified was the hospital/dispensary. Others included family planning clinics and pharmacy/shop, with little mention of non-conventional sources such as friends and relatives.
Contraceptive attitude
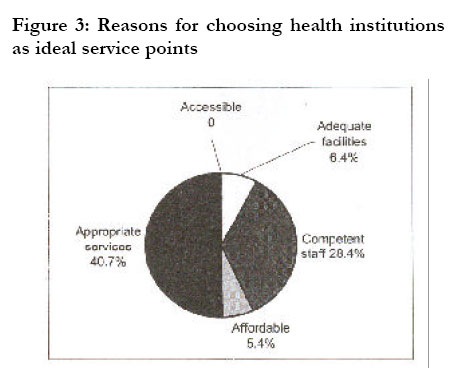
Eighty-five of the youth affirmed present and future need for youth contraceptive services. The negative attitude towards youth contraception was attributed to the perceived health risks and the notion that the practice promotes promiscuity. Data revealed the basis of this perception as, not definite facts or real life experiences, but rather mere hearsay. Ironically, some opponents were current modern contraceptive users. Adult opinions on youth contraception also vary from full support of effective youth contraception for service-seekers to total opposition of the issue as inappropriate. There are, also, moderates who advise youth contraception only under very special circumstances, such as pregnancy and STI counselling. Eighty three percent of the youth favoured health institutions (hospital/dispensary and the family planning clinic) as ideal service points, basing on different reasons as shown in Figure 3. In terms of adequacy of currently available services, 47.7% believed these were mostly adequate, 26.5% felt they were only sometimes adequate and 25.8% felt they were hardly ever adequate. These varied attitudes were based on issues of current levels of availability (39.7%), accessibility (24.2%), appropriateness (22.4%), affordability (3.1%), and acceptability (2.6%) of the services.
Contraceptive practice
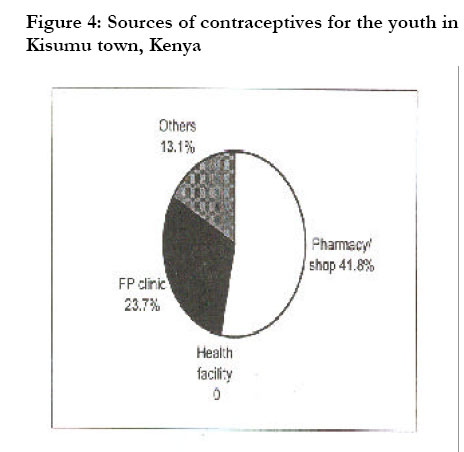
Fifty two percent of the youth had ever-used a contraceptive method, and the trend in the common methods ever-used shows popularity of the male condom, with the pharmacy/shop as the most common service source. In general 34.6% of the youth had used a contraceptive method during their first sexual experience, a probability that decreased with age. Only 31.4% of the youth are current users of a contraceptive method. The most common method in use was the male condom, especially among the younger youth. The choice of the currently used method was based on its effectiveness in pregnancy prevention (43.4%), disease prevention (37.7%), affordability (9.8%), ease of use (8.2%) and availability (0.8%). Common sources for currently used methods are shown in Figure 4. The disparity between knowledge and practice of contraception can be analysed at three levels. Across the youth population, there was a 99.2 percent level of knowledge of at least one contraceptive method against a 31.4 percent current contraceptive practice level. Seventy one percent of the sexually experienced youth had ever-used a contraceptive method against 42.8% current use. Most significantly, only 57.5% of the sexually active youth were currently using a contraceptive method.
Aspects of sexuality
Seventy three percent of the youth were sexually experienced, with most of the first sexual experiences occurring within the 15-19 years age group: 74.4% these were sexually active, with 84% engaging in regular sexual encounters and 79.7% maintaining single partner sexual encounters. The major motivational factors for engagement in sex were pleasure (78.4%), obligation (15.6%) and material gain (5%). About 89.5% of the youth acknowledged the risks in sexual relationships. Of these, 65.3% viewed STI/HIV as the greatest risk and 34.1% considered unwanted pregnancy as the greatest risk. Only 0.6% recognised abortion and psychological problems as main risks. Consequently, about 51.3% of the youth believe that contraceptive use is the main precaution one can take against the identified risks, followed by abstinence (42%) and 6.7% for other practices such as faithfulness between sexual partners.
Significant background factors influencing contraceptive
use
Basing on a 95% significance level, the computation of the chi-square test of association for current contraceptive practice against independent background variables identified significant influencing factors of occupation (p = 0.01), age (p =0.02) and religion (p = 0.05) of the youth. Logistic regression analysis of these factors identified levels of strength of association highest with religion (β = 0.42), occupation (β = -0.46) and age (β = -0.66).
DISCUSSIONS
Knowledge and attitudes towards contraceptive methods The high 99.2% level of knowledge of at least one contraceptive method among the target population compares relatively well with, and even shows an increase from the national 1989 KDHS figure of 90 percent17. Most youth get their contraceptive knowledge from educational institutions and peers with parents and other relatives featuring very little as sources of this knowledge. It emerged that the youth are reluctant to consult informally with adults on contraception issues. Reasons for this include not knowing how to approach the issue and not wanting to alert the disapproving adults of the youth’s sexual activities. The ‘informed’ peer is then viewed as a better source of knowledge and counsel because of assumed confidentiality and non-judgement. Furthermore, few parents/guardians are comfortable discussing matters of sexuality with their youth. They deem issues of contraception and sexuality to be more appropriately discussed in a reactive rather than proactive fashion, especially when the youth is already involved in a sex-related problem such as an unwanted pregnancy or STI. These findings support earlier observations that parents often prefer sex-related issues to be addressed by schools21. Yet the formal education system to which the responsibility of sex education has been left is also still limited by the current debate on what aspect of family life education should be taught, to whom, and by whom. In the meantime alternative sources of information are sought in the form of inadequately informed or misinformed peers. Despite the relatively high level of contraceptive knowledge by the youth, there is still a marked lack of factual information that promotes suspicion and unfounded myths. The mystery around and undue restrictions on youth contraception contribute to negative attitudes towards effective use of the methods. Religion, though often explicitly not mentioned, greatly influences contraceptive practice among the youth and is indeed the basis of the recurrent morality concerns by the opponents of youth contraception4. It does regulate sexual behaviour, including attitude to and practice of contraception. However, the chastity stand has been pointed out as also posing several dilemmas for the sexually active faithful who, being only human, do not know which is the lesser evil. This issue is best captured in the following statement from one key informant:
The disparity between knowledge of a contraceptive method (99.2%) and other contraceptive services (14.7%) clearly shows lack of comprehensive knowledge of contraceptive services by the youth.
Knowledge and attitudes towards contraceptive service sources and
providers
Many youth (87.7%) have a fair idea of conventional sources of contraceptive services. The most favoured choice of ideal setting is the health institution-based settings, a choice based on the appropriateness of the services offered. Here, “appropriate” is synonymous to “requested for” services. Data reveals that the youth often go to service points with their minds already made up on desired service. Competent personnel address this need in an efficient and courteous manner that encourages the client to seek such services even in the future. “Adequacy” of service is equated with the available range of service supply and the accessibility of the same. Many youth believe that there is a wide range of contraceptive services available, especially the methods. However, some service facilities are viewed as hostile and inaccessible. Some health personnel contribute to this as evidenced by the stand held by one 47-year old nurse at a government hospital:
This attitude limits the desired range of services the youth are finally able to access from more accessible sources like shops, which unfortunately are often not well placed to offer a comprehensive service package. Suffice it to say that the major determinant of whether service personnel significantly influence clients depends on their level of training, competence, and ability to inspire and motivate the client. Satisfied clients are also effective proponents of contraception and hence the nature of services offered and who offers these services at any point plays a big role in influencing the youth’s attitude towards the setting’s ability to address expressed needs and consequent health seeking behaviour.
Contraceptive practice
Few youth use a modern contraceptive method during their first sexual experience, a probability that decreases with age. Where a method is used it is more likely to be a male condom whose popularity is attributed to constant media and public campaigns and advertisements, as well as its high accessibility and comparatively low cost15. Despite a higher level of knowledge of the pill, fewer females have ever-used it, considering it too cumbersome and too rigorous for irregular sexual contacts. Abstinence features very little as a method of contraception, mainly because most of the youth view it as the complete withdrawal from sex for reasons not strictly contraception-related. Instead, natural contraception practised in accordance with the ovulation cycle or “safe days period” of the female sexual partner features more. There is a definite gap between ever-use and current use of contraceptives, attributed to subsequent abstinence, discontinuations and irregularity of use between the first and subsequent sexual relationships. Discontinuations and irregularity of use have been blamed on perceived health risks such as infertility and foetus abnormality in the females, tedious method procedures such as daily pill dosage, influence from partners and societal factors like religion and peers, intimidation by the “assumed” costs, and poor attitude towards service centres and service providers.
Disparity between contraceptive knowledge and practice
There exists a disparity between contraceptive knowledge and practice, indicating that knowledge does not always constitute practice. The concern is the relationship between what the youth know on contraception and what they actually practise16,21.
Aspects of sexuality
Most youth are sexually experienced, with most of the first sexual experiences occurring within the 15-19 years age group. Many are currently sexually active and engage in regular sexual encounters with regular partners over a given period, showing a relatively stable pattern of relationships. More importantly, the youth are aware of consequences of sexual relationships such as unwanted pregnancies and STI/HIV infection. They also have knowledge of precautions for these risks as revealed by the analysis of choice of contraceptive method against reason for choice. For example, Norplant, injection and the pill are primarily chosen for their role in pregnancy prevention, while the male condom is primarily chosen for both disease and pregnancy prevention, dual roles that it can serve well if used appropriately. But the recurrent concern, as depicted by the disparity between contraceptive knowledge and practice, especially among the sexually active youth, is what the youth do given what they know21.
Factors influencing contraceptive practice
Demographic factors Age influences contraceptive use at different stages of a youth’s life. First, the young youth is less likely to have ever-used or to be currently using a contraceptive method. Secondly, the younger the respondent during the first sexual experience, the less the probability of using a contraceptive method during this first sexual act. Thirdly, the older the youth at first marriage, the greater the probability of contraceptive use. Qualitative data points out that the youth getting married at older ages are more mature and responsible and are thus able to make rational decisions related to their sexuality, including use of contraceptives12,18. Sex. Males are more likely to use contraceptive methods, especially so in the current scenario of HIV/AIDS. The role of the male condom in STIs prevention has popularised it as one of the most frequently used contraceptive methods and seen a shift in responsibility for contraception in sexual relationships20.
Socio-economic factors
Occupation. The out-of-school youth are more likely to use contraceptives than the in-school youth, basing on their age maturity and economic capacity. Marital status. The single, socio-economically dependent and sexually active youth is more likely to adopt contraceptive practice as a wise precaution against STI and pregnancy and their associated implications than her married counterpart. Level of education. The higher the level of education one attains the greater the probability of using a contraceptive method. The education system exposes one to more interactions and other sources of information that enables one to make wise decisions such as using a contraceptive when sexually active. Social activity. The youth interacting in social activities are more likely to acquire varied info+rmation and behaviour regarding contraception from peers and others such as media idols. The right or wrong information they get often consciously or unconsciously influences their attitudes and desire to adopt contraceptive practice. Cultural factors Service factors Adequacy of service facility. The youth favour friendly settings that provide their desired service readily and at affordable costs. Availability and accessibility of services impacts on the general level of contraceptive practice among the youth. Thus personnel at the service facility can motivate or demoralise the youth from seeking and using services.
Policy factors
The Kenyan policy on youth contraception is not explicit, resulting in different institutional and individual policies ranging from open-door policy for married couples to prohibition of service provision to the more vulnerable unmarried youth7,9. This has contributed to the practice of unsafe sex and seen the rise in popularity of the more easily accessible natural contraception and condoms. It can also be sighted for the popularity of the less restrictive commercial service sources over health institution-based facilities that otherwise offer more comprehensive services.
CONCLUSION:
This paper has explored contraceptive knowledge, attitude and factors influencing contraceptive practice among the youth in Kenya’s western town of Kisumu. There was a wide disparity between contraceptive knowledge and practice. There is need to review and revise policies and practices regarding reproductive health, sexuality and family life education.
REFERENCES
Copyright 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02034f3.jpg] [hs02034f4.jpg] [hs02034f2.jpg] [hs02034f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}