 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 2, No. 2, April, 2002, pp. 47-51 ORIGINAL ARTICLES Gestational trophoblastic disease following complete hydatidi- form mole in Mulago Hospital, Kampala, Uganda * Dan K. Kaye Department of Obstetrics and Gynaecology, Makerere University Medical School,
P. O. Box 7072, Kampala, Uganda. Code Number: hs02038 ABSTRACT Objectives: To determine epidemiological characteristics and clinical presentation of complete hydatidiform mole (CHM) and complications associated with prophylactic chemotherapy with oral methotrexate. INTRODUCTION Complete hydatidiform mole (CHM), in which there is total degeneration of the trophoblast, is the commonest gestational trophoblastic disease (GTD). Histologically, it presents with diffuse trophoblastic hyperplasia with variable degrees of cellular atypia 1 . Worldwide, there is marked temporal, regional and ethnic variation in the prevalence of CHM 1,2 . High prevalence is reported in China, South East Asia, Northern Europe, the Middle East, and Eastern and Central Africa. In Uganda, Smith 3 found a prevalence of CHM 1.073 per 1000 deliveries (1969-1973). He recommended a policy of routine chemoprophylaxis for all cases of CHM, a policy which began to be implemented in 1980. At that time, many patients who presented with molar pregnancy were apparently lost to follow-up, and presented later with malignant GTD. A prevalence of 3.82 per 1000 deliveries was reported in 1997 4 . Since 1970, no study has analyzed the clinical epidemiology of GTD, yet there has been marked improvement in diagnosis of the disease by use of ultrasound scan and assay of Human chronic gonadotrophin hormone (hCG). For a drug to be used for prophylaxis, it must be safe, effective and convenient. No study has analyzed the complications associated with use of Methotrexate for prophylactic chemotherapy against GTD. If this prospective study was to describe the epidemiological factors and clinical presentation of CHM, and complications associated with prophylactic chemotherapy using oral Methotrexate. METHODS The study was conducted in Mulago hospital, the national referral hospital for Uganda, in the Obstetrics and Gynaecology Department, between 1st September 1995 and 30th January 1998. Permission to carry out the study was granted by Mulago hospital Ethics and Research Committee and the Department of Obstetrics and Gynaecology. The subjects were patients with clinically and histologically -confirmed CHM admitted to the hospital. These were followed for periods ranging from 12-30 months, and were reviewed every 3 months for the first year and every 6 months thereafter. On admission, the patients had history taken and examination and investigation done (notably ultrasound scan, liver function tests, renal function tests and chest X-ray to determine the clinical features and exclude malignant GTD. Evacuation was done by suction curettage or manual vacuum aspiration, and formal dilatation and curettage was done to get specimens for histology for those who were referred after abortion or evacuation. Data was also collected on the patients’ socio-demographic characteristics (age, age of spouse, education level, parity, age at first pregnancy), menstrual history and contraceptive ever-use. For all patients, a risk score for persistent trophoblastic disease was made. They were given oral Methotrexate 0.4 mg/kg/day (25mg/day) for five days in 3 divided doses (10mg, 5mg and 10mg at 6.00 a.m., 2.00 p.m., and 10 p.m. respectively) as directly observed therapy (DOT). At intervals between courses ranging between 9 and 16 days, 78 patients received 1-8 courses of oral Methotrexate as a single agent (total 187 courses). A normal full blood count was a prerequisite for starting therapy. On taking each dose, an inquiry was made of any complaint the patient had, especially related to drug and the staff on duty signed on the treatment sheet. Supportive treatment with intravenous fluids, antibiotics and anti-fungal agents was given to those with toxic symptoms of chemotherapy (severe mucositis, dermatitis, leucopenia or hepatitis). Folinic acid was not used. At each review, evaluation was done by history, examination, serum hCG assay and chest X-ray as a minimum. Remission was diagnosed when the hCG levels fell to normal ranges, without clinical or imaging evidence of disease by end of 60 days post-evacuation. Three patients were lost to follow-up after 6 months, while 16 did not receive any chemoprophylaxis. Data was collected using a coded questionnaire RESULTS
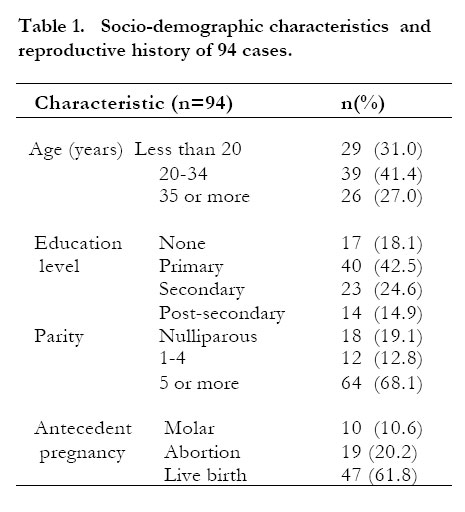
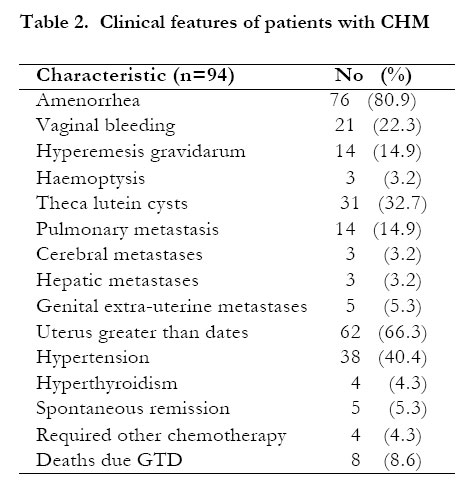
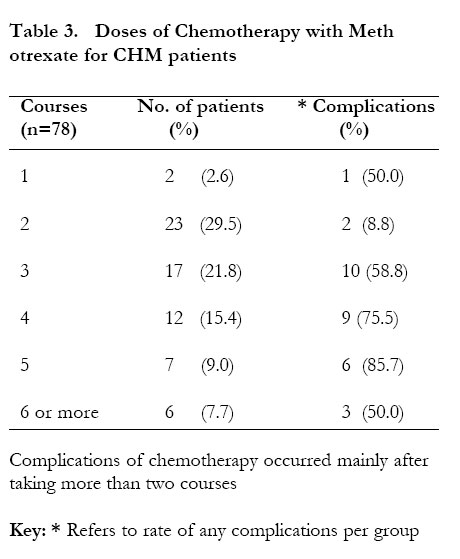
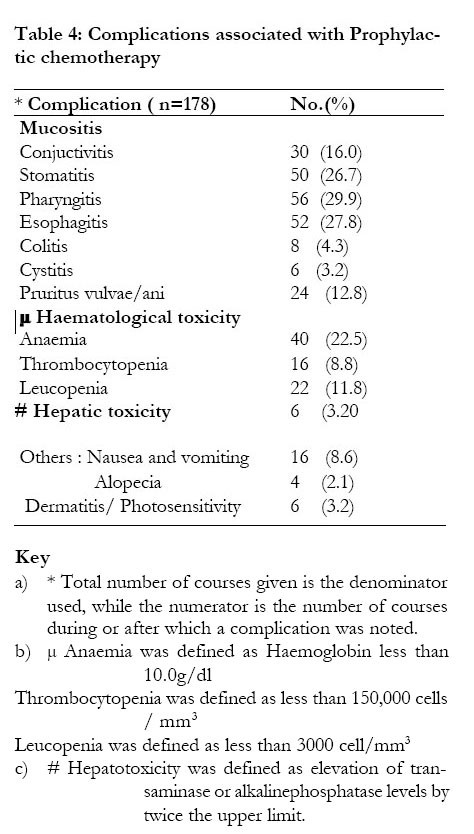
During the study period, there were 94 cases of CHM and 27,485 deliveries were seen in Mulago hospital, giving an incidence rate of 3.42 per 1000 deliveries. The mean age was 29.6 +8.5 years (range 14 -52). The antecedent pregnancy was also molar for 10 women (10.6%), while 16 (17,0%) and 4 (4.3%) had 1 and 2 prior molar pregnancies respectively. Table 1 shows the socio-demographic characteristics and the reproductive history of the 94 cases. CHM was common in adolescents and those aged 35 or more years. Six of these patients aborted spontaneously, 48 (51.0%) had suction curettage, 16 (17.0%) had manual vacuum aspiration while 24 had dilatation and curettage. None had hysterectomy, or induction of labour with oxytocics. Table 2 shows the clinical features of the patients both pre- and post-evacuation. Eighty one percent had amenorrhea and presented in the second trimester (mean gestation age 17 weeks) with threatened abortion or history of molar abortion. Thirty -one (32.7%) had theca lutein cysts, which were bilateral in 25 cases, palpable per abdomen in 20 cases and complicated by torsion in 3 cases. Six women had acute respiratory complications due to trophobast pulmonary embolism, however 14(14.9%) had radiological metastases but only 3 developed haemoptysis. These 3 later developed clinical cerebral metastases. In those with extra-pelvic lesions, 2 had vaginal nodules, 2 had cervical lesions while 1 had a vulval ulcer. One patient had profuse haemorrhage from a vaginal lesion. Twenty-four patients (25.5%) developed persistent trophoblastic disease, of whom 9 (9.6%) died of GTD. The cause of death (all of whom had received prophylactic chemotherapy) was severe anaemia 2, blood transfusion reaction1, malignant GTD with both pulmonary and cerebral metastases4and pulmonary metastases 4. Seventy-eight women received 187 courses of oral methotrexate. One patient died after the first course, of severe anaemia (which arose from therapy). Table 3 shows the courses used and the number who developed complications. The minimum number was 1, but one patient died after the first course and another did not complete the second course. Three women had 7 courses and 1 had 8 courses. Table 4 shows the nature of complications noted in 26 patients (33.3%) on methotrexate. The commonest complications were mucositis and hematological toxicity. Leucopenia, thrombocytopenia and hepatotoxicity were the indication for discontinuation of treatment, and occurred mainly after the second course. The majority of patients presented with vaginal bleeding. Presence of extra-uterine metastases indicates a diagnosis of Malignant metastatic GTD or Choriocarcinoma. None of the patients continued to have vaginal bleeding after evacuation. The commonest complications were mucositis, hepatotoxicity and haematological (Mainly anaemia and leucopenia) DISCUSSION Gestational trophoblastic diseases (GTD) are a continuum from the benign CHM, through to the malignant nonmetastatic GTD (previously called invasive mole, NMGTD) to the metastatic (commonly called choriocarcinoma, MGTD). Both malignant types can arise as a CHM, a normal pregnancy or a non-molar abortion 1. All have similar epidemiological risk factors, which include conception at extremes of reproductive age, high parity and prior molar pregnancy 1,2. The variation in the incidence of CHM in the literature arises from 3 factors: the definition used for CHM, the denominator used (total pregnancies, total deliveries, total live birth or total population of women of childbearing age), and the population at risk 2. The incidence obtained in the study, though higher than in 1969-1973, may be an under-estimate, as not all women with spontaneous abortion had specimens taken for histology. Likewise, there is now improved diagnosis of CHM by use of ultrasound and serum hCG assay. On epidemiological risk factors, prior molar pregnancy, ages < 20 years and > 35 years, and high parity were associated factors. These are recognised risk factors 1,2,3,4. Prior history of CHM is a recognised risk factor 6, the risk being higher for those who had more molar pregnancies. In this study, 10(10.7%) women had the antecedent pregnancy as molar, while 16(17.0%) and 4(4.3%) had at least 1 and 2 molar pregnancies respectively, and 19 (20.2%) had unspecified spontaneous abortions prior, some of which could have been molar. On clinical features, 80.9% presented in the second trimester with threatened abortion. This is the commonest presentation 1,2. Theca lutein cysts, which are due to stimulation of the theca by high hCG were present in 31(32.7%) of cases, of which 25 were bilateral, 20 were palpable per abdomen and 3 required emergency surgery or torsion. In prior studies, Montz et al 7 found them in 50% of 273 cases, 3 of which needed emergency surgery, while Mungan et al 8 found them in 50% of 310 cases, 1.8% of which required emergency surgery. Rare features include acute pulmonary complications due to massive trophoblast embolisation, pre-eclampsia and hyperthyroidism. Features associated with high risk molar pregnancy are very high hCG levels, uterus larger than dates of gestation or exceeding 20 weeks, large theca lutein cysts, maternal age greater than 40 years, prior molar pregnancy, hyperthyroidism and pre-eclampsia 9. Histological findings include marked trophoblast hyperplasia, presence of extensive necrosis and haemorrhage, marked trophoblast immaturity and cytotrophoblastic proliferation 9. These are related to high hCG levels. Histology alone is not reliable in diagnosis of malignant GTD 9. The diagnosis of persistent gestational trophoblastic disease was based on persistently elevated serum hCG levels, with or without chemotherapy, at least 2 months after abortion or uterine evacuation. In the study, 24(25.5%) had persistent GTD. This is consistent with the literature that about 20% of CHM result in persistent GTD 10. Other evidence of persistent GTD include persistent amenorrhoea, persistent vaginal bleeding or theca lutein cysts, development of massive trophoblast immobilization several weeks after abortion or evacuation, and evidence of extra-pelvic disease, at least 2 months after abortion or uterine evacuation 1,2,8,9,10. Therefore, patients on follow-up should have serial chest X-rays, clinical evaluation and assay of serum hCG levels 1,2,10. Progressivelyrising levels at any time post-evacuation, levels exceeding 20,000I.U/ml four weeks or more post-evacuation, persistent levels even in absence of extra-uterine disease, are indication for chemotherapy 1. In this study, oral methotrexate was used for prophylactic chemotherapy in 78 women (187 courses, range 1-8 courses, without folinic acid or citrovorum rescue factor). Overall, the drug was well tolerated for the first 2 courses, and toxicity occurred mainly after completion of the second course. Mucositis (mainly stomatitis, pharyngitis, esophagitis, colitis, conjunctivitis and diarrhea) were the commonest complications. Others were hematological and hepatic toxicity. The rate of complications of 33.7% , was comparable to that of Kashimura et al 12, who used parenteral methotrexate. Therefore, care must be taken if 3 or more courses are given for chemoprophylaxis, with close monitoring for mucositis, hepatic and hematological toxicity. The primary remission that occurred in 54 of 78 patients treated (69.2%) is acceptable and comparable to that of oral methotrexate. This is one of the few studies where oral methotrexate was evaluated as a single agent for chemotherapy for CHM and persistent GTD. It is also the first study to evaluate the Mulago policy of prophylactic chemotherapy with oral Methotrexate for CHM. In a prospective study to evaluate the role of single-agent prophylactic chemotherapy with Parenteral methotrexate for CHM, Kashimura et al 12 followed 420 patients for 5-15 years. Twenty-two (7.5%) of 293 patients on chemotherapy developed secondary trophoblastic disease compared to 23(18.1%) of 127 who did not receive it. In the above study, 30.7% of the patients on chemotherapy developed toxic symptoms, mainly mucositis, thrombocytopenia and leucopenia, with no deaths or discontinuation of therapy due to the drug, and all received folinic acid. Three times as many patients who got chemotherapy developed secondary trophoblastic disease, but were cured by combined treatment with a single agent. They concluded that chemotherapy of CHM did not entirely eliminate occurrence of metastatic disease as a single agent for treatment of non -metastatic GTD, Lurain & Elfstrand13 found parenteral Methotrexate (0.4mg/kg/day intravenously for five days per treatment course, repeated every 14 days) extremely well tolerated and effective in 89.3% of cases, with significant toxicity in 12 (4,7%). These studies show that Methotrexate is effective and safe for chemotherapy. The variability in the rate of complications and remission may be due to individual variability in the rate of drug absorption. Low doses are well absorbed, but high doses are incompletely absorbed especially when used over a long time, and meals may affect absorption rate 14. Barter et al, who used a single oral dose (given 1 hour before or 2 hours after meals to enhance absorption), found oral methotrexate to be equally safe, tolerable and cost-effective. Oral methotrexate is cheaper, more convenient in dosage and more acceptable to patients than parenteral regimens, as it may be given on out-patient basis. Mucositis, however, may interfere with drug absorption (increasing or increasing rates), thus affecting drug bioavailability and toxicity, and meals may interfere with absorption. Sulphonamide and non-steroidal anti-inflammatory agents, by displacing methotrexate from binding sites on albumin, may increase free serum drug levels, thereby increasing toxicity. CONCLUSION Complete hydatidiform mole occurs in Ugandan women at prevalence 3.4 per 1,000 deliveries. Many women present with high-risk disease, associated with high parity and conception at extremes of ages. Although oral methotrexate is cheap and tolerable, complications are common when several courses of the drug are used for prophylactic chemotherapy, mainly mucositis and hematological toxicity. Methotrexate does not eliminate the occurrence of, or prevent death from, metastatic gestational trophoblastic disease. Recommendations Patients with CHM should be monitored closely for the development of post-evacuation gestational trophoblastic disease. Those on prophylactic chemotherapy require close monitoring for the toxic effects of the drugs, mainly for mucositis, haematological and hepatic complications. REFERENCES
Copyright 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02038t4.jpg] [hs02038t3.jpg] [hs02038t2.jpg] [hs02038t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}