 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
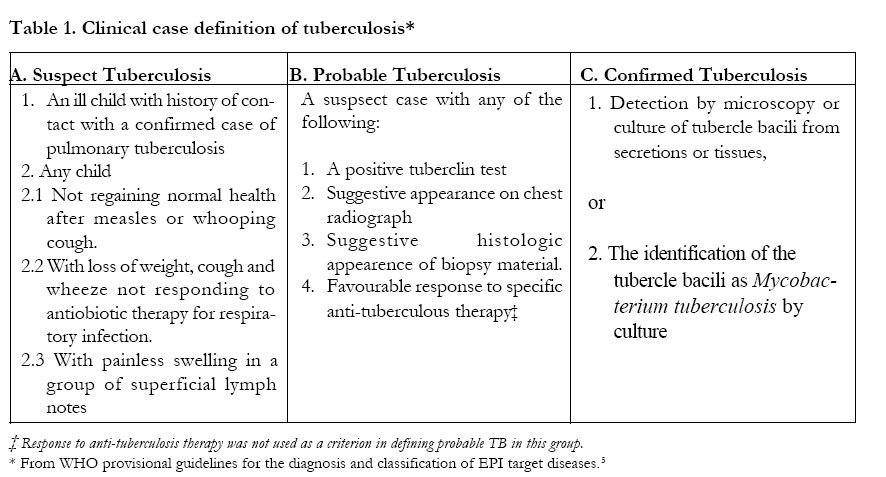
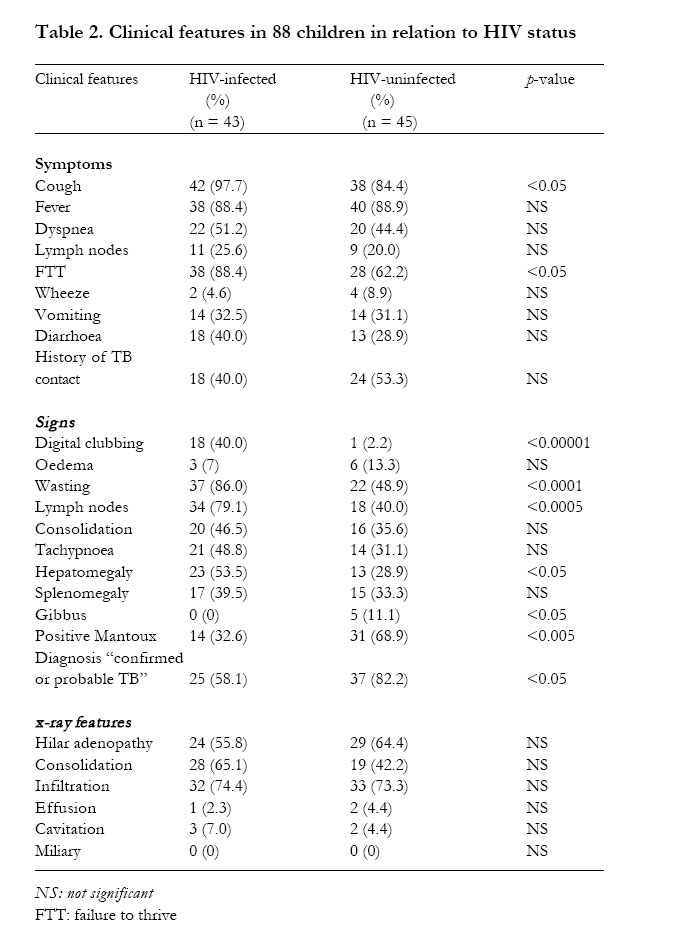
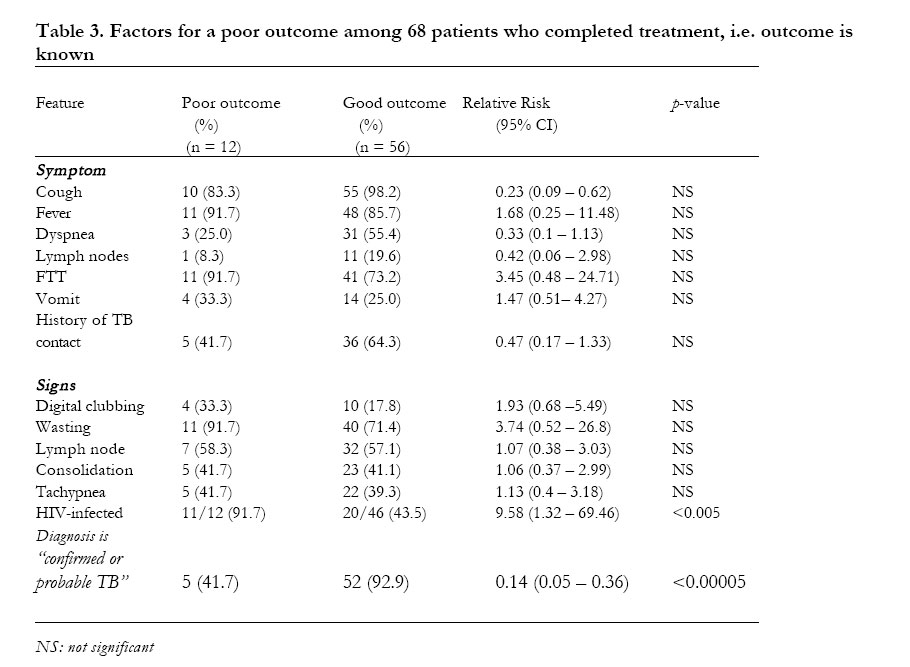
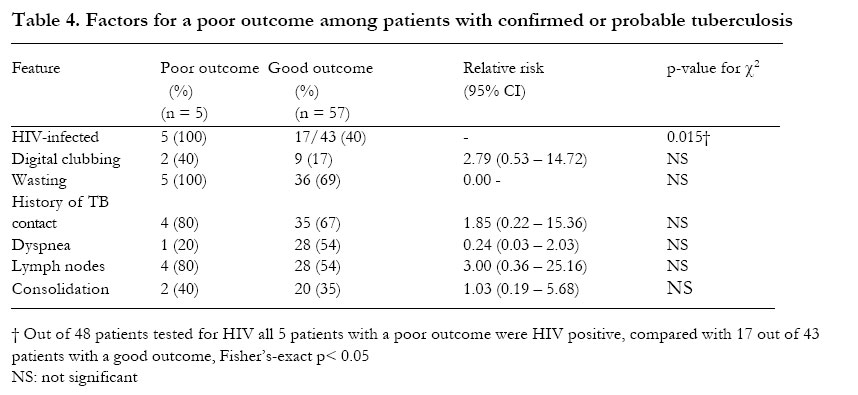
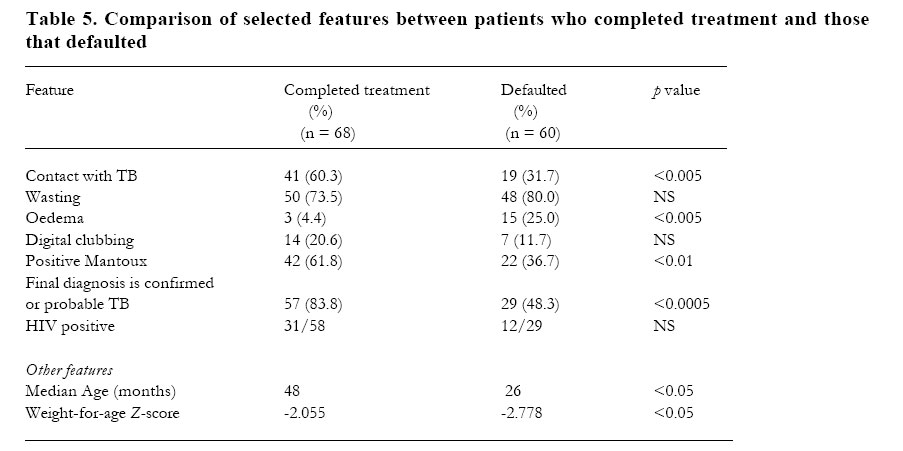
African Health Sciences, Vol. 2, No. 3, December, 2002, pp. 82-88 ORIGINAL ARTICLES Tuberculosis in children at Mbarara University Teaching Hospital, Uganda: diagnosis and outcome of treatment Julius P. Kiwanuka 1 1 Department of Paediatrics, Mbarara University of Science and Technology, Mbarara, Uganda Corresponding Author: Dr. J. P. Kiwanuka Department of Paediatrcis Mbarara University of Science and Technology P. O. Box 1410 Mbarara Uganda Fax: + 256 485 20782 Email: jpkiwanuka@yahoo.co.uk Code Number: hs02045 ABSTRACTBackground: The diagnosis of tuberculosis in children is difficult particularly in HIV infected children. The poor outcome following antituberculosis treatment usually reported in HIV infected children might be due, in part, to other HIV-related chronic diseases wrongly diagnosed as TB. Keywords: Childhood tuberculosis; HIV infection; diagnosis; outcome of treatment. INTRODUCTION There has been an increase in the reported incidence of tuberculosis throughout the world in the last decade .1 In most African countries, this increase has been attributed largely to the HIV epidemic.2 The diagnosis of tuberculosis in children is acknowledged to be imprecise, often relying on various non-specific clinical and radiological criteria.3 In young children, confirmation by smear of sputum and gastric aspirates is difficult, and facilities for culture of Mycobacteria are limited indeveloping countries. The problem of diagnosis is further complicated by the considerable overlap in clinical presentation between tuberculosis and HIV-related chronic respiratory diseases, both conditions common in Uganda. Furthermore, HIV/ TB co-infection has emerged as a major problem in many African countries.4 Consequently, tuberculosis is frequently suspected (but rarely confirmed) and treated in both HIV-infected and non HIV-infected children, and the reported increase in incidence of TB in children may be due, in part, to an increase in non-TB chronic respiratory disease in HIVinfected children. A trial of specific antituberculous treatment is accepted as a rational recourse when the suspicion of TB is strong but the diagnosis cannot be confirmed. A favourable response is often used as part of the definition of “probable TB”.5 This study sought to assess the clinical presentation, diagnosis and outcome of treatment of tuberculosis in children in Mbarara Hospital; and to examine the role of various factors, including HIV infection, on the outcome. METHODS PatientsAll children aged 0-14 years presenting to the paediatric wards of Mbarara University Hospital, with clinical tuberculosis over an 18 month period (December 1998 to May 2000) were assessed and invited to enrol in the study. The definition of clinical tuberculosis was based on the WHO provisional guidelines for the diagnosis and classification of EPI target diseases (WHO 1984) as outlined in table 1.5 Patients were officially enrolled into the study when a decision to treat for tuberculosis was made by the attending paediatrician. Assessment and investigations Clinical and demographic information recorded for each patient included age, sex, caretaker, symptoms, duration of illness, history of contact with an adult case of tuberculosis, smear status of the contact where possible, BCG immunisation and any previous treatments for the symptoms. A full physical examination, including weight, was performed in all patients. Investigations included Mantoux test and chest Xray on all patients. Where available, sputum and other specimens were examined for acid-alcohol fast bacilli using the Zehl-Nelsen method. Gastric aspiration was not attempted. TB cultures are not available at this hospital. Mantoux testing was performed using 5 TU of tuberculin PPD RT23. Results were read between 48 and 72 hours and recorded as the transverse diameter of induration. Induration of 5 mm or more was regarded as positive. An HIV test was offered to all patients during the period of follow-up and where parental consent was given, it was undertaken using the Abbott DetermineTM HIV-1/2 Test card. Polymerase chain reaction (PCR) was unavailable for confirmation of HIV infection in infants under 15 months. TreatmentAll patients were treated using the standard short course regimen recommended by the National TB and Leprosy programme in Uganda that is 2 months of daily rifampicin, isoniazid and pyrazinamide, followed by 4 months of daily rifampicin and isoniazid (2RHZ/4RH). Additional treatments including haematinics, nutritional supplements and antimalarials were also given where indicated. Patients with HIV infection and suspected Pneumocystis carinii pneumonia received co-trimoxazole in addition to the TB treatment. Follow-upAll patients were treated at home following a brief initial period of admission lasting between one and two weeks. Thereafter they were examined at least once every month until completion of treatment. At each visit their symptoms were reviewed and any changes in clinical and anthropometric signs recorded. Any side effects to the treatment were noted and action taken according to standard guidelines. At the end of treatment, each patient was assigned to one of five outcome categories: ‘improved’, ‘not improved’, ‘deteriorated’, ‘defaulted’ or ‘died’. Improvement was defined as a resolution of symptoms and signs, and satisfactory weight gain. Conversely, patients classified as “not improved” had either persistent symptoms or signs or their weight gain was inadequate. Worsening symptoms, appearance of new symptoms and signs or continue loss of weight defined the “deteriorated” category. Patients who did not complete the prescribed six months of treatment were recorded as defaulters. AnalysisFor the purpose of analysis patients were divided into two outcome groups as follows: “good” outcome including those that had improved, and a “poor” outcome including those recorded as not improved, deteriorated or died. Defaulters were excluded from this comparison, as their outcome could not be ascertained. Data were analysed using the Epi Info version 6.04 statistical analysis package. The Yates’ corrected χ2 test was used for comparison of proportions between HIV-infected and uninfected subgroups. The relative risk was used to assess the impact of various risk factors on the outcome of treatment. Ethical considerationsEthical approval for the study was obtained from the Mbarara University Research Committee. Verbal consent for participation in the study was obtained from the parent or guardian of each child enrolled. Separate consent for HIV testing was obtained in each case after appropriate counselling. RESULTS Presenting features and diagnosisOver the 18-month period 128 patients were enrolled in the study. Patients who did not complete a minimum follow-up period of six months were excluded from the analysis of outcome. However, all 128 patients initially enrolled were included in the analysis of clinical and laboratory features at presentation. The median age was 36 months (range 2 months to 13 years), with a male to female ratio of 1.06:1. Four patients (3.1%) had a diagnosis of TB confirmed on smear of sputum and/ or ear swabs. Eightytwo patients (64.1%) had “probable TB” and 42 (32.8%) remained as “suspected TB” even after investigations. A history of contact with an adult case of TB was reported in 60 (46.9%) patients. This included 36 (60%) patients whose contacts were smear-positive, 4 (6.7%) smear-negative and 20 (33.3%) whose smear-status was unknown. Mantoux testing was performed on 117 patients. The mean diameter of palpable induration was 10.6 mm (range 0 – 60 mm). Sixty-four patients (50%) had a positive Mantoux test. These included 2 patients with confirmed, 60 with probable and 2 with suspected TB. A history of contact with an adult TB case was significantly associated with a positive Mantoux (relative risk = 1.68, [95% CI 1.17 – 2.41], p = 0.006). A negative Mantoux test was associated with wasting (relative risk = 0.48, [95% CI 0.35 – 0.64]), and a positive HIV status (p = 0.001). HIV testing was performed on 88 (68.8%) patients and consent for testing was withheld in 40 (31.2%). Of the 88 tested 43 (48.9%) were HIV-positive. Comparison between HIV positive and negative patientsThe clinical features, contact history and Mantoux results of the patients in relation to HIV status are shown in table 2. Symptoms of cough and failure to thrive, and the physical findings of digital clubbing, visible severe wasting, enlarged lymph nodes and hepatomegaly were all significantly more common in HIV positive patients. Conversely, HIV positive children were significantly less likely to have a positive Mantoux test. There was no significant difference in the frequency of reported TB contact. HIV positive patients were less likely to be classified as “confirmed or probable TB” (p = 0.025). Follow-up and outcome analysisAfter a minimum six-month period of followup, 68 patients had completed treatment and therefore had a known outcome. Of these, 56 (82.4%) had improved and were classified as “good outcome”, while 12 (17.6%) failed to show improvement or deteriorated, and 3 of them died. These were classified as “poor outcome”. Table 3 shows the analysis of the various risk factors for a poor outcome of treatment. HIV positive patients were significantly more likely to have a poor outcome (relative risk = 9.58, [95% CI 1.32 – 69.46]). Failure to thrive (RR = 3.45) and wasting (RR = 3.74) appeared to be risk factors for a poor outcome, but did not reach statistical significance. A diagnosis of confirmed or probable TB was associated with a good outcome (relative risk for poor outcome = 0.14, [95% CI 0.05 – 0.36]). Of the 68 patients with a known outcome 57 (83.8%) had a diagnosis of confirmed or probable TB. Within this subgroup again HIV positive children were significantly more likely to have a poor outcome (Fisher’s exact p = 0.015), (table 4). Sixty patients (46.9%) were lost to follow-up before completing the minimum six-month period on treatment and were classified as defaulters, of whom 42 defaulted within the first month of treatment. Table 5 shows a comparison of selected features between the defaulters and those who completed treatment. Defaulters were significantly younger (median age = 26 months vs. 48 months, Krukas-Wallis H = 4.9; p 0.03), had a lower mean weight-for-age Z score (WAZ = -2.778, t = 2.0, p = 0.047) and had a higher frequency of oedema (χ2 = 9.54; p = 0.002). On the other hand, patients who completed treatment had a higher frequency of TB contact (χ2 = 9.37; p = 0.002), more positive Mantoux tests (χ2 = 7.06; p = 0.008) and were more likely to have a diagnosis of“ probable or confirmed TB” (χ2 = 15.0; p = 0.0001). DISCUSSION The impact of HIV infection on the clinical expression and treatment of tuberculosis in adults has been widely described 6,7. However, it has been more difficult to do the same in children owing to the difficulties in making a firm diagnosis of tuberculosis. Nevertheless, tuberculosis is frequently suspected, and treated, in a child with chronic respiratory symptoms, especially if these are associated with growth faltering or weight loss. This study emphasises the difficulty of moving beyond this suspicion to making a confident diagnosis of TB. The study also highlights the important link between a firm diagnosis of tuberculosis and a good outcome on treatment. A diagnosis of TB was considered highly probable in 67% of the patients, including only 3% with confirmed TB. The rest were treated despite lack of additional evidence for tuberculosis infection. This proportion is similar to that reported from other centres where the majority of children treated are recorded as ‘smearnegative’ PTB.8 Increasing proportions of children treated for TB in Africa are HIV-infected. Such children often receive repeated courses of antituberculosis therapy even when the diagnosis of TB remains uncertain. The HIV seropositivity rate of 49% found in this study is similar to that in earlier reports from Malawi9 and Zambia10, and emphasises the impact of the HIV epidemic on the childhood TB notification rates in this area. As in previous studies the outcome of treatment in this patient-group was poorer in HIV-positive patients (relative risk for a poor outcome = 9.58), even when the diagnosis of TB was considered highly probable.9 Various reasons for this have been suggested including advanced immunosuppression, poor absorption of drugs, poor compliance and possibly infection by multidrug resistant strains of MTB. 11,12,13 However, owing to similarities in clinical presentation, a significant proportion of such children will have other HIV-related chronic respiratory diseases rather than tuberculosis. Clearly, their response to antituberculosis therapy would be expected to be poorer. In this study we defined ‘probable TB’ before initiation of treatment and thus excluded the clinical response as a diagnostic criterion (see table1). A diagnosis of ‘confirmed or probable TB’ was significantly associated with a good outcome. HIV-positive patients were less likely to be classified as ‘probable or confirmed TB’. This finding is similar to that reported from an earlier study in Malawi.9 This may have been partly due to lower sensitivity of the Mantoux test and the difficulty in interpreting chest X-ray changes. However, one has to accept that some of them did not have TB at all. As in previous studies HIV-positive patients had a significantly higher frequency of clinical signs such as digital clubbing and generalised lymphadenopathy, which suggest the presence of other diseases like LIP and bronchiectasis. 9,14 Thus the poorer response to treatment may have been due, in part, to a wrong diagnosis. In contrast to adult tuberculosis, which frequently results from reactivation of latent infection, tuberculosis in children is most often the result of a new and recent infection.15 The suspicion of tuberculosis in a child should therefore stimulate the search for a smear-positive contact in the child’s environment, and finding such a contact makes the diagnosis more probable. A history of TB contact was reported in 60 patients, and was associated with a positive Mantoux test in both HIV positive and negative patients. The Mantoux test remains useful in the diagnosis of TB in children and is frequently positive even in HIV-infected children. In a recent study of Malawian children with suspected PTB, 11 out of 31 Mantoux-positive children were HIVinfected.9 In this study, although less sensitive, the Mantoux was positive in 14 HIV-positive patients, comprising almost one third of the total number of positives. Loss to follow-up constitutes a significantly frequent and frustrating outcome of treatment of children with tuberculosis. The reasons for this are usually uncertain. In our study, almost half of the patients did not complete a six-month course of treatment, most of them defaulting within a month of commencement. Patients who defaulted were more likely to have an uncertain diagnosis of TB. This has been the experience in another study, where the authors reported higher lost-to-follow-up rates among children with an unknown diagnosis.9 In addition, defaulters were younger and more severely malnourished, and probably had a higher mortality rate at home. In conclusion, HIV infection is common among children presenting with suspected tuberculosis in this hospital, and has a significant impact on the clinical features, as well as the outcome of TB treatment. HIV positive children with suspected TB frequently have signs that suggest the presence of other diseases such as LIP and chronic bronchiectasis; and are less likely to have a diagnosis of “probable or confirmed TB” after investigations. Patients with an uncertain diagnosis of TB are less likely to improve on anti-TB therapy. AcknowledgementsThe author would like to acknowledge the contributions of Dr J Mwanga, Dr A Ndamira and all the staff of the paediatric wards of Mbarara Hospital in the continued clinical care of the patients in this study. We also acknowledge, with thanks, the donation of tuberculin PPD for the study by Dr D Newsom. Special thanks go to Professor J Axton and Professor H Bode for their help. REFERENCES
Copyright © 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02045t4.jpg] [hs02045t5.jpg] [hs02045t1.jpg] [hs02045t2.jpg] [hs02045t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}