 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
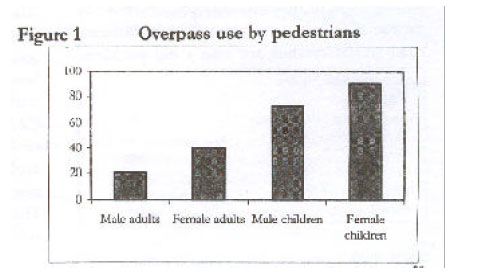
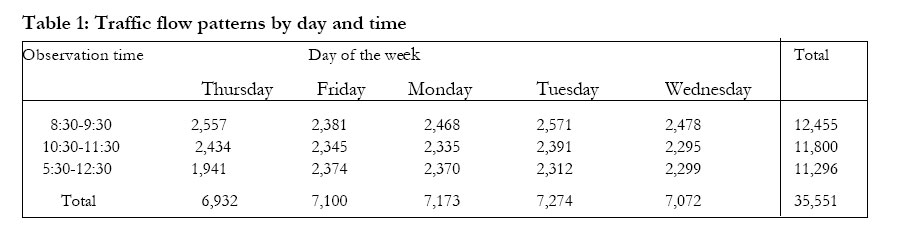
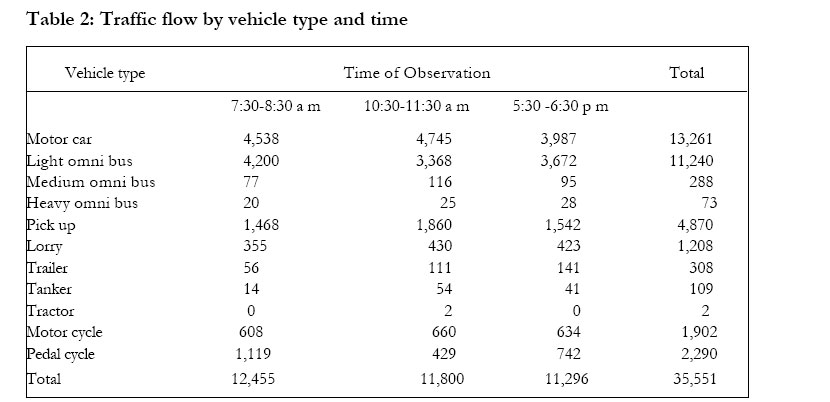
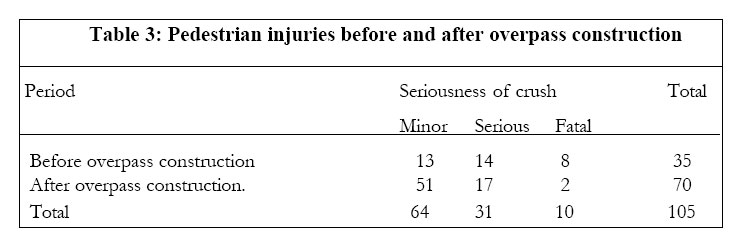
African Health Sciences, Vol. 2, No. 3, December, 2002, pp. 89-93 The effect of an overpass on pedestrian injuries on a major highway in Kampala – Uganda Milton Mutto1, Olive C Kobusingye1, Ronald R Lett2 1Injury Control Centre-Uganda, Makerere Medical School 2The Canadian Network for International Surgery Correspondence Author: Milton Mutto Injury Control Center-Uganda, Makerere Medical School Box 7072, Tel: 256-041-543438, Fax: 256-041-530022, E-mail: icc@med.mak.ac.ug Code Number: hs02046 ABSTRACTObjectives: To describe the pedestrian population, their use of an overpass, and to assess pedestrian perceptions and responses to the risk of traffic crashes, determine pedestrian injuries in relation to traffic flow, and compare traffic crash and pedestrian injury rates before and after the overpass construction. Key words: Overpass, Pedestrian Injuries, Urban Uganda, Accidents. INTRODUCTION Road traffic crashes have been highlighted as a major global public health problem1. In 1998, they were responsible for 1,170,698 million deaths, ranking tenth among the leading causes of death globally2. The Global Burden of Disease Study3 projected road traffic deaths to be 1.39 million in the year 2000, and traffic injury to be the third leading cause of disability adjusted life-years4 by the year 2020. In low and middle income countries, road traffic crashes are also a big problem, estimated to cost between 1-3 % of the gross domestic product (GDP)5. In Uganda, they are the leading cause of injury fatalities and disabilities in urban areas6. Pedestrians are most susceptible, representing 70% of traffic fatalities in most developing countries7, and the larger proportion of traffic injuries on urban roads8. A study in Ethiopia showed them accounting for 85% of casualties in Addis Ababa in 1991 and yet only 40% nation wide9. In Zambia, they accounted for two-thirds of fatalities and over half of road traffic casualties in urban areas compared to only 30% of fatalities and 12% of total casualties in the rural areas10. In Uganda11, hospitalbased studies showed pedestrians as the most frequent traffic casualties (43.5%), followed by vehicle occupants (31.9%). Hospital-based trauma registries in two hospitals also showed pedestrians as the leading category of road users (45.8%) presenting with serious traffic injuries as assessed using the Kampala Trauma Score (KTS<13)12. The pattern of traffic injuries in developing countries reflects their high pedestrian populations, rapid motorization, and poor state of the road infrastructure 13. Their roads usually have a traffic mix, poor illumination and signposting, poor maintenance and roadside hazards14. Road infrastructural improvements are therefore critical in tackling this problem, although a combined strategy of education, law enforcement, and environment modification has been recommended 15. Many developed countries have made substantial progress in improving their road safety by applying multisectoral counter measures with special emphasis on road planning and traffic engineering16. Where pedestrians and non-motorized traffic are deliberately targeted, road casualties can be considerably reduced. This study assessed the effect of an overpass on the rates of pedestrian crashes and injuries. We described the pedestrian population, their use of the overpass and assessed pedestrian perceptions of risk of traffic crashes, and their behavioral response, determined pedestrian injuries in relation to traffic flow and compared traffic crashes and pedestrian injury rates before and after the overpass construction. METHODOLOGYThe study was conducted in Nakawa approximately 6 kilometers on the Kampala-Jinja highway between the 16th and 22nd of December 1999 using cross sectional and retrospective designs. Pedestrian road behaviors and traffic patterns were observed at two peak hours (7:30 am-8:30 am and 5:30 p m-6:30 p m ) and one non peak hour (10:30 a m-11:30 a m), since traffic patterns were envisaged to vary with work and business routines in the city. A convenient sample of overpass and nonoverpass users was also interviewed during the observation period to assess their perceptions of risk. The respondents were alternately selected by sex in each age category as they arrived at the crossing point. Police traffic crash records covering one year before and one year after the intervention were reviewed for traffic injuries in this trading center. Eight research assistants were recruited, trained and deployed in pairs at 50meter intervals along the road 100 meters either side of the overpass. Four of them observed pedestrians crossing through traffic, two observed pedestrians crossing on the overpass and two observed vehicles. Two other research assistants conducted the interviews. Ethical issuesPermission was obtained from the relevant government agencies including the Ministry of Works, Transport and Communications, the Engineering division of Kampala City Council, the Road and Traffic Safety department of the Uganda Police and the Nakawa local councils. Consent was obtained from the respondents before the interviews were conducted and confidentiality was ensured. RESULTS Pedestrian perceptions of risk One hundred and twenty-three pedestrians were interviewed (male: female ratio of 1.01:1), adults constituted 69.7% of them. Nearly 53% of the respondents cross this road daily, and slightly over half (52.0%) of them use the overpass. The overpass was untidy, poorly lit, and with children frequently loitering on it. It was also used to host advertising billboards, which screened off the pedestrian walkway. Most (77.9%) respondents worried about their safety on the road, but only 6.6% identified the overpass as the appropriate safeguard. Of those who crossed through traffic, 62.8% cited the extra walking distance, the high stairs and extra walking time as reasons for not using the overpass, 21.6% avoided it citing health reasons while 11.9% feared for their security on the overpass. Of those who used the overpass, 67.2% did so to avoid accidents. Most respondents (96.6%) claimed to know the purpose of the overpass; 87.3% thought it was for reducing pedestrian injuries, while 12.7% thought it was specifically constructed for children and old people. Overpass utilizationA total of 13,064 pedestrians were observed, with a male: female ratio of 2.2:1. The overall prevalence of pedestrian overpass use was 35.4 %. More females (49.1%) used the overpass compared to males (29.2%), while 79.2% of the children used the overpass compared to 27.3% of the adult pedestrians (Fig: 1). The gender differences in choice of crossing were significant (Odds ratio = 2.20; CI 2.032.39), while the age differences were not. Traffic patterns and pedestrian injuries at the overpass.The road was not marked. It lacked road signs and carried both motorized and non-motorized traffic. The mean traffic flow was 41.5 vehicles per minute at the 0730 - 0830 peak hour, 39.3 between 1030 and 1130 hours and 37.7 between 1700 and 1800 hours. (Tables 1& 2) The proportion of heavy vehicles (lorries, trailers, tankers, and tractors) in traffic increased from 4.2% of vehicle density in the morning to 5.49 % in the evening; this difference was significant (t =2.847, P < 0.05). Forty percent of traffic conflicts occurred in the mid morning as compared to 44.0% in the evening hours. Cars and light omni buses were the most common crash counterparts and the age group 5-30 years most frequent, accounting for 57.1% of cases. Traffic collisions and pedestrian injuries before and after interventionA total of 105 traffic collisions were reported in this trading center between September 1997 and September 1999, 33.0 % of them before the overpass intervention. Six point seven percent died, 29.5% had serious injuries and 63.8% had minor injuries (Table 3). The differences between fatal and non-fatal outcomes before and after overpass construction were not significant. DISCUSSIONThis study evaluated a pedestrian safety intervention in an urban trading center in Uganda. It examined the relationship between pedestrian perceptions and overpass use, the extent to which the overpass secured pedestrian safety, and the effect of the intervention on pedestrian injuries. There was a low prevalence of pedestrian overpass use, suggesting a flaw in its conception and design. Despite its advantages in resolving pedestrian- vehicular conflicts at specified crossing points, and the high perception of risk among pedestrians, most of them crossed through traffic; more than 90% did not recognize the overpass as the means of addressing their road safety concerns. The study also found a dramatic increase in pedestrian injuries around the overpass with total pedestrian casualties more than doubling within a year after intervention, although fatalities declined significantly. A number of reasons could account for this pattern. The overpass intervention was not popular among pedestrians, most of whom found it inconvenient, difficult to access and use. It represented an additional walking distance, high stairs and longer crossing time compared to the alternative through traffic. Pedestrians are known to avoid facilities that add to their walking distances16. Since pedestrian options were not restricted to the overpass, most of them crossed at “convenient” points through traffic. This was a major weakness in the overpass intervention, it assumed that pedestrians would exercise “sensible judgments” based on their knowledge and perceptions of risk and use it, which did not happen. No deliberate attempts were made to limit pedestrian options and channel pedestrian traffic to the overpass. Secondly, many pedestrians, especially females and children, complained that the overpass presented a new health and security risk. Billboards placed on it impaired visibility, casting further doubt about its safety especially in the evenings and at night. Some pedestrians feared thieves could conveniently use the overpass. An earlier study found pedestrians avoiding foot- bridges because they perceived them to be common sites for petty crime17. The absence of road markings and signs may have significantly affected traffic flow on this section of the road, implying, traffic was poorly managed at the overpass. Consequently, traffic was mixed, disorderly, congested and inefficient especially during evening hours when the proportion of heavy vehicles increased. Moreover motorists flouted traffic regulations and pedestrians avoided the overpass most in the evenings. The overpass could have resolved pedestrian-vehicular conflicts at the crossing point, if its location and design facilitated its use by pedesrtrians16. While the problem of contact was addressed, factors that promote use by pedestrians were not. A similar strategy was tried in Nigeria, but compliance by the target group was very low18. The Kampala overpass was an expensive intervention estimated to have cost 100,000 US dollars, and yet cheaper options such as Zebra crossings, humps, and signalized crossings were not evaluated. The overpass intervention did not address the need for speed regulation in the trading center, which function was earlier played by the speed humps. This meant that a motorist was given the responsibility of his or her own speed control, which was difficult to assure. The overpass intervention was therefore expensive not only in money terms, but also pedestrian losses. Its effectiveness was assessed in an ideal situation within 100 meters either side, but pedestrians beyond this distance were less likely to benefit from it. ConclusionsThe study has shown how ineffective and probably detrimental at 100 meters the overpass was and underscores the need for a comprehensive approach to problems of pedestrian safety encompassing engineering, public education and enforcement. It also demonstrates how engineering can fail if the knowledge and behaviors of intended beneficiaries are not considered. A careful study of overpass interventions is recommended before they can be replicated elsewhere. Cheaper alternatives at more frequent intervals may be more effective. AcknowledgmentsWe thank Victor Avasi, Faith Kabagenyi, Jane Karungi, Nelson Katabula, Charles Malokuwoza, Doreen Tumushabe, Miriam Nakalembe, Tina Akisu, Traffic Police officers Katuramu and Tushabomwe, who diligently collected and field edited the raw data. REFERENCES
Copyright © 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02046t1.jpg] [hs02046f1.jpg] [hs02046t3.jpg] [hs02046t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}