 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
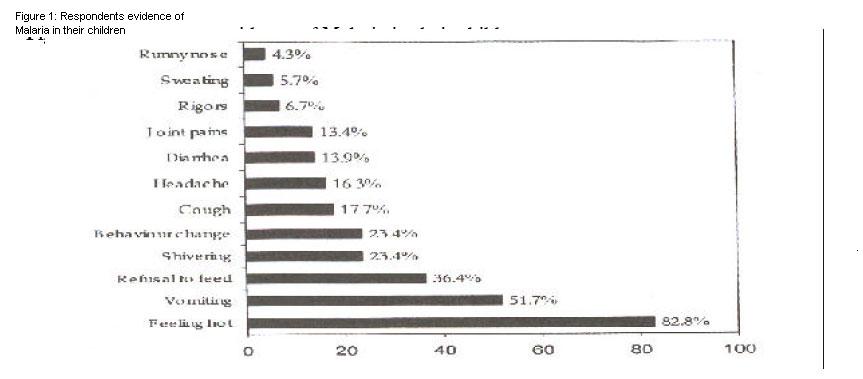
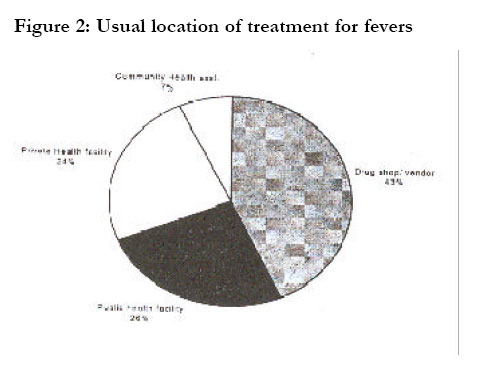
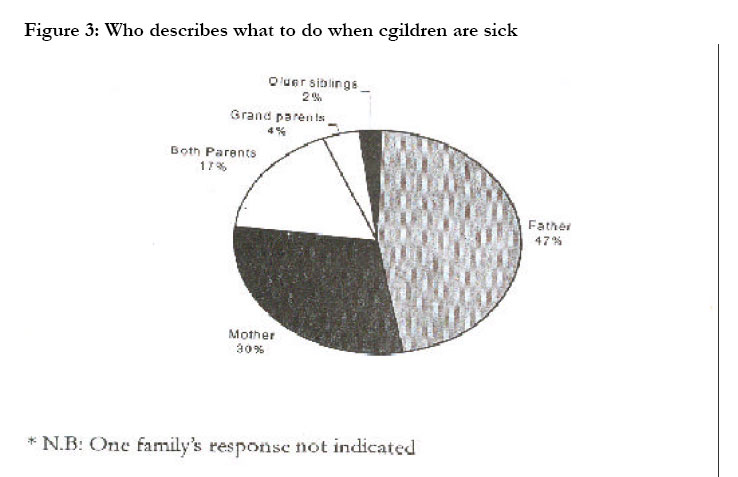
African Health Sciences, Vol. 2, No. 3, December, 2002, pp. 94-98 Health seeking behavior by families of children suspected to have malaria in Kabale: Uganda *Sam Tumwesigire1 and Sharon Watson2 1Kabale Regional Hospital, P.O. Box 7, Kabale, Uganda 2 Development Studies and Social Anthroplogy, University of Notre Daine, USA 51270 Mayflower Road South Bend, I N 46628 United States * Correspondence Author: Dr. Sam Tumwesigire Kabale Regional Hospital, P.O. Box 7, Kabale, Uganda Telephone: 256-486-22006 E-mail: klehosp@infocom.co.ug Code Number: hs02047 ABSTRACTBackground: Malaria is common among communities of Kabale district, and many young children die of the illness. Despite a good distribution of health facilities, able to handle malaria patients, families and individuals tend to depend on self-treatment, or private clinics where drugs used may be of doubtful quality. This study reports on health seeking behaviour by families with children suspected to have malaria. INTRODUCTION Kabale district is a highland area in southwestern Uganda, where malaria transmission is low or unstable. Periods of intense transmission of malaria can however occur like in the years 1998 and 2000, resulting in serious epidemics1. This was attributed to environmental changes caused by destruction of trees, draining of swamps and prolonged heavy rains, which caused frequent, flooding of the valleys, resulting in more mosquito-breeding sites. These two factors combined to increase the spread of malaria in the communities. Malaria has now become the commonest indication for attending public health facilities in Kabale district, and the leading cause of death2. The Uganda National Malaria Control Programme responded to the malaria challenge, by accelerated training of health workers in prompt diagnosis and treatment, intensified vector control methods, surveillance, social mobilization and sensitization. Healthseeking behavior in the communities may be affected by their knowledge regarding likely outcome of malaria illness. Perception and behavior will also depend on available remedies, belief, and access to care for those who are sick, the reputation and affordability of facilities in place, whether government or private. Study justification The size of the malaria problem in many communities in Africa can be influenced by host characteristics such as one’s attitude towards the disease, among others3. In East Africa, studies of health seeking behavior have been done in Kenya and Tanzania4. They mention how cultural explanations of symptoms of malaria and the social structure of the communities may affect financial transactions like those involving health care. No such study is known by the authors to have been conducted among the communities of southwestern Uganda. We took opportunity to carry out such a study in May 2001, a rainy season during which malaria attacks are most prevalent. It is hoped that the results will help to stimulate further research in this area and contribute to improvement of malaria control programmes in the district Objectives The general objective was to establish the healthseeking behavior among families in Kabale district when their children get malaria/fever. The specific objectives were to determine the knowledge of and perceptions about malaria, identify symptoms, diagnosis and treatment methods the respondents use for this disease and to assess affordability of malaria treatment. METHODOLOGY Study setting Five sub counties, which consistently reported high incidences of malaria out of a total of 16, were chosen. These included Kamuganguzi, Kamwezi, Rwamucucu, Bukinda and Kabale Municipality. Lists of villages in each of five places were drawn, out of which a total of 12 villages were randomly selected, each sub county being represented by at least 2 villages. Study populationInterviewees were those directly found looking after sick children, or family members who volunteered to speak on behalf of others. Special key informant groups of women, village elders, and the youth and health workers were separately interviewed and their responses recorded Sample sizeThe sample size was calculated using the formula by Kish and Leslie5. We assumed that the maximum proportion of caretakers with knowledge of malaria was 84% amongst a population of about 400,000. With a margin of error of 5% and 95% confidence intervals, a sample size of 206 respondents was calculated. Sampling methodUsing a village transect approach method, the direction taken by study teams from the center of a village was randomly determined by the pointing of a span pencil. Families were then sampled in alternate homes up to the end of the village in a chosen direction. Where children younger than 5 years old were found to have fever, the caretakers were asked to participate if they consented. If more than one child was sick the younger one was sampled. Data collection and handlingA prepared questionnaire with pre-coded multiple-choice options was used. The interviews were done in Rukiga, the local language. Data was entered, cleaned and processed using SPSS computer programme for statistical analysis. Frequencies of coded options and other tendencies were examined and tabulated. Ethical issuesPermission to carry out this research was obtained from the Kabale District Director of Health Services. Field teams got approval of families and clearance from village heads after explaining the purpose the visits. Respondents were free to answer all or none of the questions, and confidentiality was maintained. RESULTS General There were 209 respondents, 138 (66.0%) of whom were the mothers of sick children; 18.2% were fathers, 12.4% grand parents and 3.3% older siblings. Peasantry was the main economic occupation (66.5% of families). There was little or no formal education as only 7.9% were educated beyond primary school level. In 62.7% of families the main income earner was the father, in 27.8% it was the mother while grand parents or older siblings had this responsibility in 9.6% of homes. Of the available health care expertise in the communities, 47.3% of respondents knew of a trained nurse, 12.9% mentioned other trained health workers, 6.7% used community health staff while 33.1% did not know of someone they could seek help from in case of urgent need. Access to health facilities appeared relatively easy since 97.1% of respondents said they lived within 5 km of a health unit, and could reach it in less than 2 hours. Twelve and a half percent of the sick children were below one year of age, 61.7% ranged between 1 to 5 years while 25% were older. Both sexes were equally represented. Knowledge and perceptions of malariaRespondents unanimously said that malaria was a serious medical problem, which “has caused many deaths and made us poor”. The majority (78.5%) of respondents associated malaria with increased mosquito bites, 1.4% blamed witchcraft, and 2.9% said it was caused by dirty water, while those who did not know ranged between 13.4% and 21.5% depending on the particular community. Almost 3.8% did not respond. Asked to name symptoms they perceived and acted on as due to malaria, the most prominent ones were feeling hot, vomiting, refusal to feed, shivering and behavior change (figure 1). 73.2% said the current attack was serious but 25.8% did not think it was urgent, preferring to withhold treatment. Most respondents (80.9%) thought malaria was best treated at a government health facility, 16.7% preferred clinics and only 1.0% cited home or a traditional healer. The best type of treatment was deemed to be western medicine (92.3%). Some (5.7%) quoted combined herbs and western drugs, only 1.4% stated that herbs were their first choice. However, on further probing, 70.8% knew about at least one herb used to treat malaria. The majority of the interviewees were familiar with the names of common anti-malaria drugs: 87.1% mentioned chloroquine, 52.2% Fansidar ® or sulphadoxine pyrimethamine, and 39.2% knew of quinine. Unfortunately only 38.3% knew how to use chloroquine correctly, for Fansidar ® it was 4.3% and 0.5% for quinine. Fifty three percent of respondents said they were aware of any malaria control activities in the communities. Among community actions they mentioned were building good houses (73.7%), bush clearing (54.5%) and swamp drainage (40.2%). Personal protection methods cited included use of bed nets (62.2%), indoor insecticide spraying (48.3%), and taking drugs (1.9%). Other respondents were not sure how to protect themselves. Diagnosis, treatment, methods and practices Mothers (82.3%) were usually the first to notice their children were sick. Although 73.2% of families wanted urgent action for their sick children only 59% achieved this within 24 hours. While 21% were treated within 2 days, 20% delayed beyond this. Half the patients were treated at government facilities although 80.9% of their caretakers had said that those facilities would be ideal. The other half instead went to private clinics or just bought drugs from drug shops. Only 25.5% used government units to treat previous attacks of fevers in their children; the rest either used private clinics or received treatment at home. The demonstrated knowledge of prevention methods (90% awareness) was not translated into action as only 21.2% of families used any control method. DISCUSSION General study population Over two thirds of the families were poor peasants with little or no education. The respondents’ families are typical of rural communities in Uganda in general and Kabale in particular. Being a strongly patriarchal society, it was not surprising that 2/3 of children’s caretakers were mothers while men were the main income providers and had to approve of when to start or stop a child’s treatment. Since mothers were the first to detect illnesses but had relatively little empowerment to initiate action, this could also result in treatment delay. This delay (found in 22.5% of the sick children) is dangerous, as it increases the risk of severe disease6. Knowledge and perceptions of malariaMost (80.9%) of respondents knew that malaria was transmitted through mosquito bites, and disease incidence increased when more mosquitoes were breeding during long rains. General prevention methods: living in good houses (73.7%), bush clearing (54.5%), using mosquito nets (62.2%) and insecticide spraying (48.3%) were mentioned which was impressive. This may have been due to health education messages from ongoing malaria control activities as testified by 53.1% of those interviewed. The Tanzanian study also revealed high levels of awareness4. Chloroquine was the best known anti-malarial followed by Fansidar ® and quinine in that order, but their correct use was not well grasped. Only 38.3% knew how to use chloroquine correctly, for Fansidar ® it was 4.3% and 0.5% for quinine.This suggests a high incidence of inappropriate treatment, which worsens risk of severe disease and encourages development of drug resistance. Diagnosis, treatment methods, practices and affordabilityThe five commonest symptoms of malaria cited by the caretakers of the children were feeling hot, vomiting, refusal to eat, shivering and behavior change in that order. At the moment there are no universally agreed clinical criteria for malaria, but common experience in endemic areas correlates high temperature (>37.5°C) with malaria7, 8. It is concluded therefore that the families could confidently recognize malaria on clinical grounds. It was surprising that almost all (97.1%) lived within 5 kilometers of a health unit which access was much better than the Ugandan average of about 49%. The respondents said they chose where to obtain treatment because of: belief in treatment offered (31.1%), free or cheap drugs (25.8%) and convenience (14.8%). The condition of the child came last at 5.7%. We sensed this had to do with economic hardships as only 23.6% of the families could afford costs of treatment. The rest had to borrow money, sell something or just do nothing. This general poverty reduced the capacity of many surveyed households to access good malaria treatment. The practice of home or self-medication may also be a manifestation of reduced trust and confidence in the public health system, perhaps because of poor services available (such as lack of drugs, few trained personnel and inadequate diagnostic facilities). In this respect, a betterorganized private health sector could be utilized more to promote the objectives of the malaria control programme in the region for example by training drug vendors, herbalists, families, volunteers and all those who handle malaria patients. Many other communities in Africa also rely on the private health sector for medial care9-11 as do other communities in Uganda where 47.6% of fever cases are self- treated according to a recent survey12. The high level (80.9%)of awareness about malaria control methods may have been due to health education messages from ongoing malaria campaign activities as testified by 53.1% of those interviewed. However, the poor knowledge of how to correctly use these control methods should be addressed so as to reduce prevalence and chances of inappropriate treatment. Use of herbs to treat malaria needs mention as it was practiced but was found to be less common here than reports from elsewhere in Africa where up to 80% of people may use them to treat fevers13. The use of herbs in our surveyed families was most likely due to lack of access to modern drugs. This calls for further studies to investigate, identify and confirm effectiveness of local remedies and their anti-malarial properties and to establish their safety. CONCLUSIONIn the studied communities of Kabale district, health-seeking behavior for children with malaria was influenced by capacity to afford treatment. There appeared to be reduced trust in the public heath care system and more reliance on the informal sector including use of herbal medicine. Many obtained treatment late. Awareness about personal and community malaria control issues was fairly good but use of these methods was low. AcknowledgementWe are grateful to Dr. J. Katungu, the DDHS of Kabale for approving this study, Dr. Kato of the National Malaria control program for his encouragement, the staff and students at Kabale hospital for doing the field survey, Ms Regina Nyangoma and Judith Orishaba for typing the manuscript. REFERENCES
Copyright © 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02047f4.jpg] [hs02047f1.jpg] [hs02047f3.jpg] [hs02047f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}