 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 2, No. 3, December, 2002, pp. 121-123 Congenital lobar emphysema: a diagnostic challenge and cause of progressive respiratory distress in a 2 month-old infant. Richard I. Idroa, Harriet Kisembo b and Didas Mugisac Department of Paediatrics and Child Health, Mulago Hospitala Correspondence Dr Richard Iwa Idro, Department of Paediatrics and Child Health, Mulago Hospital P.O Box 7051, Kampala – Uganda. Fax: + 256 – 41 - 530022 Code Number: hs02052 Abstract
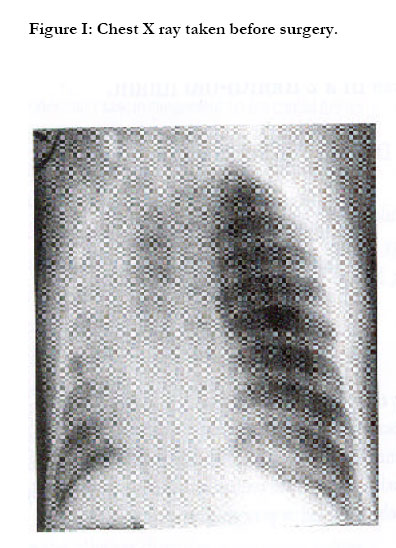
Congenital lobar emphysema (CLE) is a rare congenital abnormality characterized by over inflation of a pulmonary lobe. It often presents a diagnostic and therapeutic dilemma. No case has been described in Uganda in the previous 10 years. We describe a case of a 2 months old infant who presented with severe respiratory distress. A diagnosis of congenital left upper lobar emphysema was established on diagnostic imaging. Both his vascular anatomy and the bronchial wall were normal. He improved dramatically after surgery. The SaO2 normalized within 12 hours of Surgery (lobectomy) and the postoperative period was uneventful. Case Report History and clinical features A 2 months old boy presented to Mulago hospital (National Referral Hospital of Uganda) with a 6 weeks history of cough, wheezing, and progressive difficult/noisy breathing but no fever. At the age of two weeks, he was admitted to a district hospital with features suggestive of bronchopneumonia. He spent one week in the ward and failed to improve on antibiotic therapy. While at home, his condition worsened and the child was brought to Mulago hospital. He however continued to breastfeed normally. He is the sixth child in his family. His parents are not consanguineous neither was there any history of neonatal deaths in the first and/or second-degree relatives. The prenatal and peri-natal history was uneventful. The birth weight was 3.9kg. At admission, the infant was cyanosed with a SaO2 of 80%. He had no gross dysmorphic features, no finger clubbing, diaphoresis or dependent oedema. He was tachypnoeic with severe chest in drawing and a respiratory rate of 80/min. The chest had minimal expansion with respiration, the trachea was shifted to the right, and he had a hyperesonant percussion note over the left anterior thoracic region. There were bilateral scattered rhonchi and crepitations. The radial pulse was regular, small volume with a rate of 150/ min though the intensity of the heart sounds was not altered. Both the liver and spleen were displaced 3 cm below the costal margin. Investigations The chest radiograph showed a gross over inflation of the left upper lobe. The inflated lobe herniated into the right side of the chest and the grossly enlarged left upper lobe displaced the mediastinum with it (figure I). No structural defects were seen on echocardiography but the great vessels were poorly visualized at the left parasternal region. A computerized Tomography Scan of the chest confirmed an emphysematous left upper lobe but with no anatomical abnormality of the bronchial wall. Other investigations included a total WBC count of 8300/mm3 with a differential count of lymphocytes 61%, granulocytes 30.2% and monocytes 8.8%. The Hb was 12.7g/dl and the platelet count was 280,000 mm3. Surgery
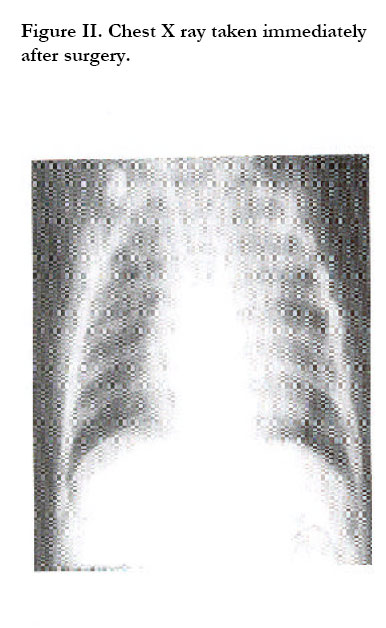
Surgery was done using a left postero-lateral thoracic incision. The pleura and vascular anatomy were found to be normal. The left lung was bipolar but its upper lobe was emphysematous and grossly enlarged. It filled the left hemi thorax and extended to the right displacing the mediastinum. There were no tension cysts and both the lower lobe and lingula were normal. A left upper lobectomy was done and the lingula fixed to the lower lobe to prevent volvulus. The SaO2 increased to 95% the same evening and no complications developed. He was discharged after a week. Discussion We describe a case of congenital lobar emphysema. Over the previous 10 years, no single case had been seen in Mulago, the national referral hospital of Uganda. This may be explained by the failure to make a diagnosis of congenital lobar emphysema at peripheral units as in this child or a true reflection of the prevalence of the disease. Several factors have been associated with the development of congenital lobar emphysema. In 50% of cases there is decreased bronchial cartilage tissue. This defect produces a ball valve effect with consequent overinflation.1, 2Vascular abnormalities that produce compression3, bronchial stenosis2, bronchogenic cysts4, and congenital cytomegaloviral infection have also been associated.5 Congenital lobar emphysema has been described in twins6 but in up to 40% of cases, the cause is unclear.2 Our patient had a normal vascular anatomy and bronchial cartilage on gross examination nor were there any other lung abnormalities. Concurrent congenital heart disease (usually patent ductus arteriosus, or ventricular septal defect, occurs in 15% of cases. 7 Our patients had neither of these on echocardiography. A case has been described where combined sequestration, bronchogenic cyst and dysgenetic lung simulated congenital lobar emphysema radiographically in a newborn.8 The age of onset of symptoms of congenital lobar emphysema ranges from a few days after birth to six months.7Most patients develop symptoms in the neonatal period and the male: female ratio is 3: 1. 9 As in this child, respiratory distress is the commonest mode of presentation. There is dyspnoea, wheezing, grunting respiration, tachypnoea and sometimes progressive cyanosis. Similar symptoms may occur in bronchopneumonia, cyanotic congenital heart diseases, and several congenital abnormalities of the lung. 2, 10, 11In more than 50% of cases, the left upper lobe is involved2 and there is a shift of the mediastinum as was the case here.2 The basic investigation in congenital lobar emphysema is the chest radiograph from which a diagnosis can be made and is readily available. In an Indian series, a correct diagnosis on chest radiography before referral was made in only 4 out of 10 cases even though the diagnosis could be arrived at in the 10 cases using the initial radiographs.7 Computerized tomography, bronchoscopy and angiopulmography are also used in the diagnosis.1, 2 In this child a computerized tomography scan was done to exclude an extrinsic mass effect as the cause of the over inflated lung and to demonstrate the bronchial anatomy before surgery. Other radiological investigations including scintigraphic ventilation perfusion lung scans, angiography, Magnetic Resonance imaging (MRI), and Barium oesophagography would have been successfull. Scintigraphic ventilation perfusion lung scans would have shown poor perfusion and slow ventilation of the involved lobe. Angiography either by direct pulmonary artery injection or digital subtraction methods shows slow and poor arterial filling. Angiography and MRI have been used to ensure that the patient does not have an anomalous pulmonary artery. Barium oesophagography is performed to exclude a bronchogenic cyst or pulmonary sling. 12 Congenital lobar emphysema may be confused with tension pneumothorax. In CLE the pulmonary vessels extend to the periphery of the hyper-inflated lobe and there is no visualization of a pleural line unlike in a pneumothorax. Decubitus and cross lateral radiographs may aid in distinguishing between CLE and a pneumothorax. In some centres, prenatal ultrasonography has resulted in early diagnosis. Prenatal diagnosis can also be done using magnetic resonance imaging. Congenital lobar emphysema can be distinguished from other lesions on ultrasonography by differences in echogenicity and reflectivity. 13 Operative surgery with lobectomy is the commonest mode of treatment.2 Depending on the symptoms, conservative measures are sometimes taken but this may fail in the presence of inter-current infections. Resection of vascular rings may be the only surgical procedure where this is the cause.7 In over 85% of cases, the long term outcome after surgery is excellent with complete cure.14 Our patient improved immediately after surgery with normalization of the SaO2 within 12 hours. In summary, the diagnosis of CLE may present a diagnostic challenge and a high index of suspicion in neonates with progressive respiratory distress is important if the diagnosis is to be made promptly. The outcome of surgery is good in most cases. (Figure 2)
Copyright © 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02052f2.jpg] [hs02052f1.jpg] |
| |||||||||

{kind=link}
{kind=link}