|
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
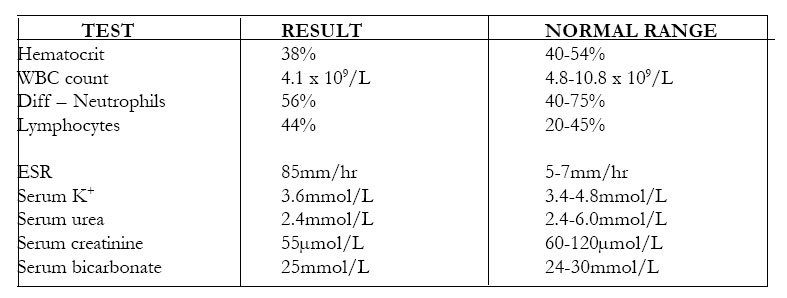
African Health Sciences, Vol. 2, No. 3, December, 2002, pp. 124-126 A 14-year-old Nigerian female with idiopathic intracranial hypertension (Pseudotumor cerebri or benign intracranial hypertension) A.C Onwuchekwa*, C.N. Nwankwo**, E.N. Chapp-Jumbo** Neurology Unit, Department of Medicine, University of Port Harcourt & University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria. Authors for Correspondences Dr E.N.Chapp-Jumbo Department of Medicine, University of Port Harcourt & University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria. Email: chap.jumbo@mwkl.co.uk Code Number: hs02053 ABSTRACTA 14-year-old secondary school girl presented with acute onset severe generalized headache associated with vomiting and diplopia. These followed an initial fever, which responded to chloroquine. She had been on perflacine for a left knee septic arthritis until onset of her symptoms. The main findings on physical examination were mild obesity, left abducent nerve palsy, bilateral papilledema and evidence of resolving arthritis of her left knee. The results of her investigations, including a brain CT scan were within normal limits. A diagnosis of IIH was made. She responded satisfactorily to oral acetazolamide with complete resolution of her symptoms and signs within 12 days of hospitalization and 2 weeks of follow-up. BACKGROUND & OBJECTIVE Idiopathic intra-cranial hypertension (IIH) is not commonly encountered and when it is, delay in initiation of medical treatment can lead to permanent visual impairment. It is a diagnosis of exclusion. This is the first reported case in Port Harcourt, Nigeria and it serves to create awareness and the importance of early treatment. CASE REPORT J.A. was a 14-year-old Nigerian female secondary school student referred from a peripheral primary health-care center on the 23/03/2001 with the complaints of severe generalized, throbbing headaches for 6 days, vomiting for 3 days and diplopia for one day, prior to presentation. The headaches were worse with straining and in the mornings with no associated neck pains. There was an initial fever that subsided with antimalarial treatment. She started vomiting three days into her illness and this was non-projectile, worse in the mornings and not proceeded by nausea. Diplopia was observed a day before presentation and worse with attempting to look towards her left. She had been taking oral pefloxacin mesylate (peflacine) for septic arthritis of her left knee secondary to trauma diagnosed a month earlier, until the onset of her illness. She denied travels to the meningitis belt of the country in the recent past, use of oral contraceptives or sexual exposure. She does not take alcohol or use tobacco in any form. There is no past history of similar illness or family history of migrainous headaches, diabetes, sickle cell disease or brain tumors. Physical examination showed that she was obese with a BMI of 30.6, conscious and alert, photophobic, afebrile, not pale, not jaundiced, acyanotic, mildly dehydrated and breathing normally. Her pulse rate was 72/minute and BP 120/70mmHg. She had no neck stiffness; Kernig’s and Brundzinsky’s signs were negative. Pupillary reaction to light and accommodation was normal bilaterally and there were no visual field defects. She had left abducent nerve palsy and fundocospy revealed both fundi to have pink discs with blurred margins and engorged vessels. The visual disc: cup ratio was 0.3 bilaterally and there was good macular reflex and background bilaterally. These findings were in keeping with bilateral papilloedema. Her muscle tone, power and reflexes were normal in all limbs and so were her sensation and coordination. Further systemic examination was unremarkable except for a mildly swollen and tender left knee joint with no redness or warmth but with some limitation of movement. A diagnosis of a Raised Intracranial Pressure ?cause, to rule out Idiopathic Intracranial Hypertension (IIH) or Metastatic Brain Abscess was made and she was admitted for investigation and treatment. Chest X-ray was within normal limits. The results of her investigations were as shown:
Brain CT scan revealed a normal cranial vault, sella and suture lines. The brain slices showed normal tissues and ventricular systems and there were no intracranial mass lesions. X-rays of the left knee joint revealed a narrowing of the medial tibio-femoral and patello-femoral joint spaces with spiking of the tibial spine, suggestive of secondary osteoarthritis. Urinalysis showed normal findings. Lumbar puncture was not done because of the signs of raised intracranial pressure and the diagnosis was uncertain initially. A definitive diagnosis of Idiopathic intracranial hypertension was eventually made and the patient was placed on a weight-reducing diet, oral actazolamide 50mg tds and analgesics. She responded satisfactorily on the above regimen with the resolution of her headaches and vomiting, while the ocular palsy gradually resolved and she was discharged on the 4/4/2001 after 12days of hospitalization. On follow-up visit two weeks later, she had completely recovered without any sequelae and her fundal re-examination and visual fields were normal. DISCUSSIONThis is the first reported case of IIH in UPTH, PH. It is not commonly encountered. A review of neurological admissions from Kenya1 showed no reported case of IIA. This rare neurological disease entity was first recognized by Quinke in 1897 2. It has previously been described by various terminologies such as toxic hydrocephalus, otitic hydrocephalus, hypertensive meningeal hydrops, pseudoabscess, pseudotumor cerebri and lately benign intracranial hypertension in 1955. However the name IIH has been suggested because about 20-50% of cases experience permanent visual impairment 2. No age group is immune to the disease but there is a female preponderance in a ratio of M: F, 1:3. There is a strong association with obesity and weight gain during the twelve months prior to diagnosis. Patients present with symptoms similar to those of our patient, including infrequent ones such as intermittent and paroxysmal alteration of consciousness, tinnitus and paraesthesias; seizures are thought never to be part of the classic symptoms. The most consistent finding is papilledema and there may also be ocular palsies, both present in our patient. The diagnostic criteria 2,3,4 include symptoms related to intracranial hypertension – headache, in the absence of focal neurological symptoms; signs related to intracranial hypertension – papilledema and enlarged blind spots in the absence of focal neurological signs except for 6th nerve palsy; documented intracranial hypertension; normal CSF cellular content and biochemistry and a normal cranial CT or MRI. Our patient met these diagnostic criteria, except the CSF findings. The diagnosis of IIH is one of exclusion. The diagnostic studies required include plain skull radiographs, which shows sutural diastasis in the young, in addition to demineralization of the sella. It is diagnostic of intracranial hypertension, but this is seen only in 10% of patients 3. Electroencephalogram (EEG) is normal in nearly 90% of adult patients but there is a higher incidence of abnormal studies in patients below 20 years of age 3. Isotope brain scans are normal in a vast majority of patients. CT scan and MRI are usually normal while CSF findings include an elevated pressure, usually greater then 250 mm H20 with variable levels of protein 5. There are numbers of clinical conditions which meet the modified Dandy’s criteria for association with IIH2, these include hematological disorders such as iron deficiency anemia, pernicious anemia and polycythemia rubra vera; endocrine disorders like corticosteroid deficiencies, corticosteroid excess, thyroid and parathyroid diseases and pituitary diseases such adenomas and acromegaly; metabolic or nutritional disorders such as cystic fibrosis, galactokinase, galactosemia, hyper- or hypovitaminosis A, vitamin D deficiencies and rickets; drugs such as anabolic steroids, phenytoin, chlorpromazine, lithium carbonate, tetracycline, nalidixic acid, nitrofurantoin, sulfamethoxazole, amiodarone, and indomethacin. Our patient was taking a quinolone, pefloxacin, of which nalidixic acid is a member, until the onset of her illness. It is difficult to say the role of this drug in the genesis of her illness as the other strong factors like her gender and obesity were at play. Some disease conditions, which are also associated with this entity according to the modified Dandy’s criteria, include sarcoidosis, systemic lupus erythematosis (SLE), any obstruction to cranial venous outflow such as head injury, chronic ear infections and obstruction of flow through the arachnoid granulations. The treatment of IIH requires critical decisions relating to timing, which should be before the onset of permanent optic nerve death and the type of therapy. Medical treatment should be instituted first with weight reducing diet, acetazolamide 2-4g/day. Other drugs that have been used with success include glycerol 0.25-1.0g/ kg/dose bd or tds, frusemide 20-60 mg daily and paradoxically, corticosteroids 40-60 mg/day. Other interventions found useful in selected cases include, serial lumbar punctures twice weekly initially then weekly until resolution of signs and symptoms of disease 2. Surgery is indicated when existing visual field defects enlarge or deepen during the course of medical treatment; when new visual scotomas occur; when a Marcus-Gunn’s pupil develops or when visual acuity falls. This usually takes the form of optic nerve sheath incision and CSF shunting 6. The long-term prognosis in this condition is good as observed in our patient with the exception of permanent visual loss, which has been documented in a sizeable number of patients 2. Poor prognostic factors include an older patient and a female sex and recurrence rate is up to 12% 2. CONCLUSIONIIH was previously thought to be benign but it is now known to cause permanent visual impairment in 20 –50% of its victims especially when treatment is delayed. This case reminds us of the need to bear in mind, occurrences of ‘rare’ diseases and the importance of prompt initiation of treatment. REFERENCES:
Copyright © 2002 - Makerere Medical School, Uganda |
| |||||||||