 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 2, No. 3, December, 2002, pp. 127-135 PRACTICE POINTS Corporate response to the HIV/AIDS epidemic in Uganda – time for a paradigm shift? Samson Kirondea and John Lukwagob 7 Sandown Hills 103 Katherine Street Sandown, Sandton 2196 South Africaa Code Number: hs02054 ABSTRACTThe HIV/AIDS epidemic is likely to remain the pre-eminent global health concern for the foreseeable future. In Uganda, while significant progress has been made by the government over the past decade in bringing down the rate of new infections, the HIV/AIDS burden in the country remains huge and vigilant efforts must be continued if this burden is to further decrease. INTRODUCTION The overwhelming share of the global HIV burden is borne by developing countries, where 95% of HIV infected people live. According to UNAIDS, out of the 24 countries in the world with an adult HIV seroprevalence of more than 5% in 1999, 23 were in sub-Saharan Africa. Of the global total of an estimated 40 million people who were living with HIV/AIDS at the end of 2001, 70% were from sub-Saharan Africa, which houses only 10% of the world’s population.1 The United States Bureau of Census has predicted that by the year 2010, 8 to 31 years of life will have been lost in those countries worst affected by HIV/AIDS in sub-Saharan Africa. HIV/AIDS has also led to a resurgence of other diseases, notably tuberculosis, a paucity of hospital beds available for the treatment of other illnesses and poses an immense threat by reversing the gains made over many years of trying to improve public health service delivery in sub-Saharan Africa. This region bears the brunt of the global HIV/ AIDS epidemic and yet by a cruel twist of fate, it is also the region where poverty is most pervasive (almost nine out of every ten people in Africa’s poorest countries subsist on less than US$ 2 a day)2 and hence has the least resources to effectively cope with an epidemic of HIV’s enormity. The Ugandan situation clearly depicts the ravages of the HIV scourge. Uganda has been facing an HIV/AIDS epidemic for almost two decades during which time the epidemic has had devastating effects on society. By 1996, the country was being described as the nation with the highest prevalence of HIV in the world.3,4 In 1999 alone, about 110 000 people are believed to have died from AIDS related illnesses and currently, some 1.4 million Ugandans (almost 7% of the population) are living with HIV. In addition to these effects an estimated 1 million children have been orphaned (the largest number of orphans arising from the effects of the HIV epidemic in the world) and sadly a large proportion of Ugandans personally know at least one individual, either within their own family or close circle of friends, who has succumbed to the epidemic. Despite these odds some progress in combating the epidemic in Uganda has been made over the past 15 years. With the leadership of the President, Uganda launched a tireless prevention and awareness campaign that has reversed the trend of the epidemic by almost 50% in some areas.5 HIV infection prevalence rates from the major sentinel surveillance sites in different parts of the country have continued to show declining trends. The weighted overall antenatal prevalence rate was 6.1% in 2000 down from 6.8% in 1999.6 Additionally, there has also been an observed decline in the HIV incidence for adults of all ages in the Kyamulibwa Medical Research Council cohort from 8.0/1000 person years of observation in 1990 to 5.2/1000 person years in 1999.7 So effective have has the awareness campaign been that currently more than 95% of Ugandans are now aware HIV/AIDS and the major modes of transmission.5 Meeting the Burden caused by the HIV/AIDS epidemic in Uganda The government of Uganda together with its development partners has since the beginning of the epidemic taken a leading role in advocating for and implementing of prevention and awareness campaigns all over the country. To date the following HIV/AIDS intervention strategies have been incorporated into the national health policy:
More recently, some government parastatals such as the Bank and Uganda as well as other institutions such as the theme groups of the United Nations Organization in Uganda have started providing anti-retroviral (ARV) treatment to their sick employees. The overall effect of these interventions has been a slowing down in new infection rates over the past decade. Despite these noble efforts however, the current HIV infection rate is still unacceptably high. A significant number of new infections are still occurring and due to the maturing of the epidemic many of the people who got infected during the ‘HIV heydays’ of the early and mid 1990s are now becoming ill with AIDS. This presents a huge burden whose traditional bearers, namely the government and nongovernmental organizations (NGOs); are unlikely to contain. The excess burden that government and NGOs are not currently not able to absorb predominantly falls on households and extended families of those affected, who in most cases are ill prepared to bear the brunt of the costs involved. The corporate sector in Uganda clearly has a role to play in sharing some of the burden of the epidemic, especially among the people it employs. When companies recognize the threat posed by HIV among their employees, they can pursue three basic strategies for mitigating the anticipated short- and long-term financial consequences on their businesses. They could:8
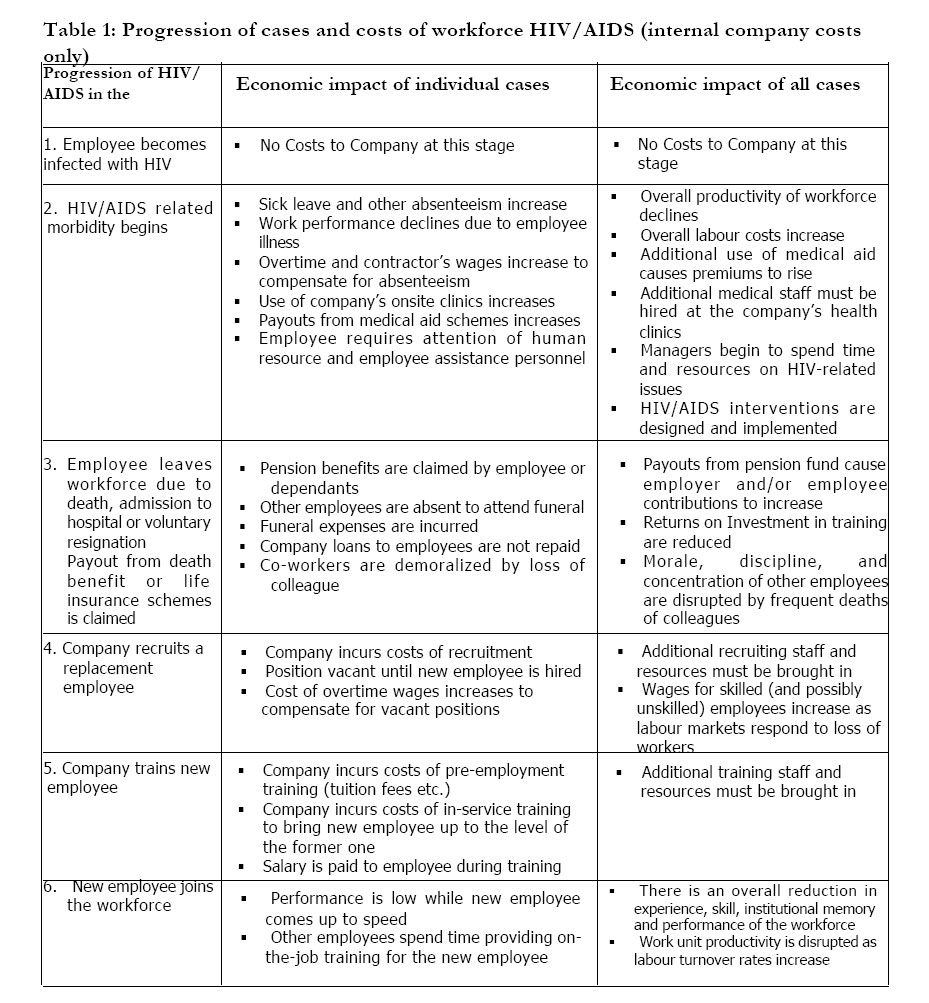
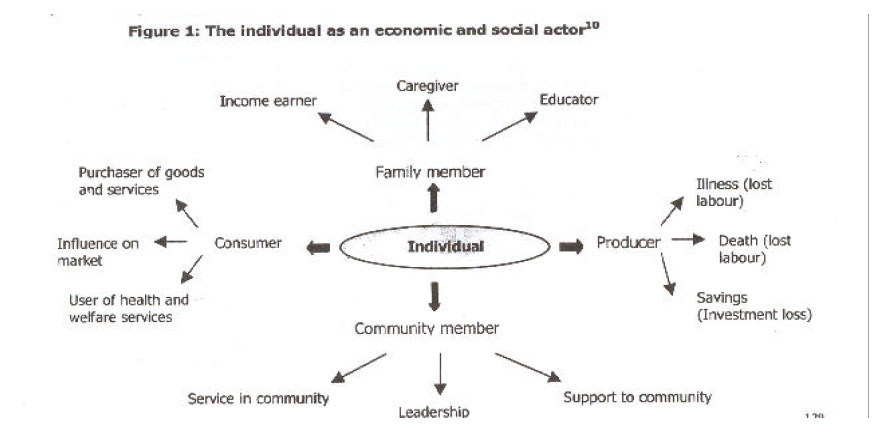
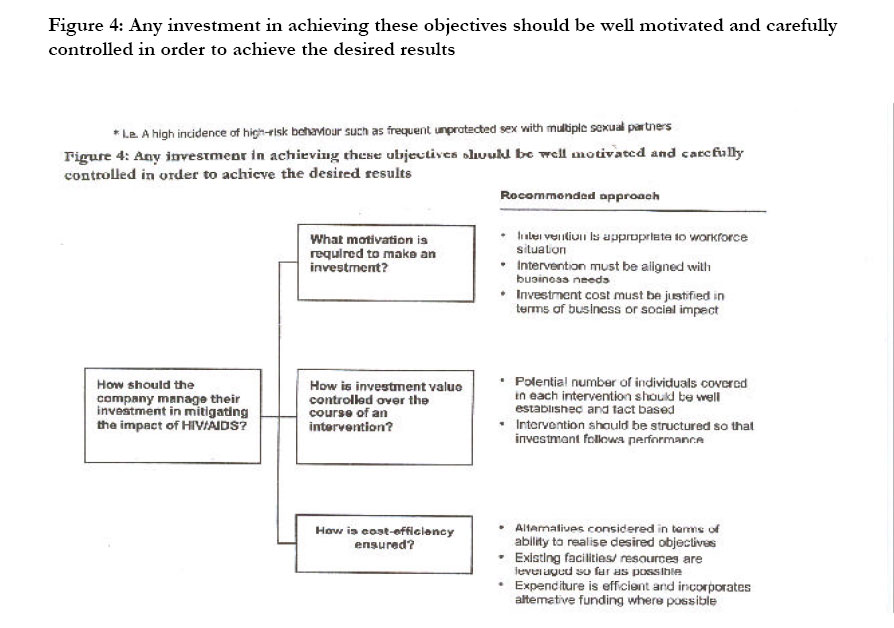
It has oft been stated that the ‘business of business is business’ and therefore the private sector may have an incentive in pursuing strategy 3 (burden shifting) or at a minimum, strategy 1. HIV/AIDS can be looked at as primarily being a social disease but which could also have significant business impact. Unfortunately, few studies in sub-Saharan Africa have rigorously attempted to quantify the cost of impact HIV/AIDS has on individual businesses which could partly explain why corporate response to the epidemic has been lukewarm at best in most countries of the region.10 While this is so we argue that added social responsibility is not mutually exclusive from profit maximizing strategies that are demanded of the corporate world by their shareholders. There is extensive experience that can be borrowed from other fields on how to balance the good for society with profit maximizing goals of business and seek for solutions that promote both sets of objectives. In the environmental field for example, many industries in the developed world have found that the mandatory safety, health and environmental technologies they have implemented as required by government regulations have also served to reduce their operating costs by making their processes more efficient. Likewise, businesses that can do more to prevent an erosion of core skills and knowledge through the loss of skilled employees to AIDS, ultimately stand to financially benefit from the increased longevity of these HIV+ employees. The same logic would apply to those businesses that have an interest in having a healthy consumer base that has disposable income to spend on buying commodities, which is otherwise not diverted to anti-retroviral treatment or to care for the orphans the AIDS epidemic leaves in its wake. Rationale The rationale for this paper derives from the important role employers in the private sector can play in combating the HIV/AIDS epidemic in Uganda. Within Uganda, approximately 90 000 people are employed by the corporate sector, with a further 400 000 dependants.9 This represents a small but significant proportion of the population in terms of income earning and tax paying capacity. Workplace-led or based initiatives against HIV/AIDS can effectively be used to reach this population. The overall response to HIV/AIDS from the corporate sector in Uganda has not been systematically addressed and only scanty information is available about this response in the literature. While it is arguable that many large businesses in Uganda have financially contributed towards fighting the epidemic in some way or another, few have comprehensive programmes in place that directly address the issue of HIV/AIDS among their employees. A pilot survey done by the authors among 5 of the biggest private sector companies in the country revealed that company-led or based HIV/ AIDS interventions often tend to be of a very limited scope. Those companies that have onsite clinics for their employees tend to provide only STD treatment and counseling as HIV prevention interventions. Comprehensive VCT is often not provided and no company was found to provide ARV therapy for sick employees. Some companies had policies whereby skilled employees where allowed to see a physician of their choice for treatment and then claim a refund for expenses incurred, but only up to the limit preset by the company. This obviously meant that expensive ARV treatment was often not covered by the medical insurance policy. Such corporate responses may in part be due to the lack of will power to commit what is often thought of as massive financial resources towards a cause whose exact business impact is difficult to quantify. Additionally we believe there is a lack of effective inter-business coordination and monitoring structures that could allow cost sharing for such interventions in the private sector. The need therefore has arisen for a more coordinated response from the private sector. Such an initiative however requires support from other key stakeholders notably Government, local and international NGOs, other civil organizations as well as the community. The aim of this paper is to propose a conceptual process in which the corporate sector can become more actively involved in combating the HIV/AIDS epidemic in Uganda. While the financial analysis necessary to calculate the present value of HIV infections and ultimately the cost to individual companies is outside the scope of this work, we have attempted to highlight where the major ‘buckets’ of costs for businesses may lie in a series of Figures and Tables in the subsequent sections of this paper. The costs of the HIV/AIDS epidemicWhile it is difficult to quantify these costs in any accurate manner, HIV/AIDS related costs stem from both internal and external effects. These costs become particularly more important in a situation where the HIV epidemic has matured and the number of people dying of AIDS is visible throughout all strata of society as is now the case with the Ugandan epidemic. Figure 1 below illustrates how an HIV infected individual could have widespread effects on society as a whole. External costs are caused by such factors as a decrease in disposable income among affected families, which results in decreased demand for company products, rising costs associated with breakdown in society etc. These can be are extremely difficult for corporate firms to manage or control. The overall economic impact of an adult AIDS death on surviving household members varies according to the following characteristics:11
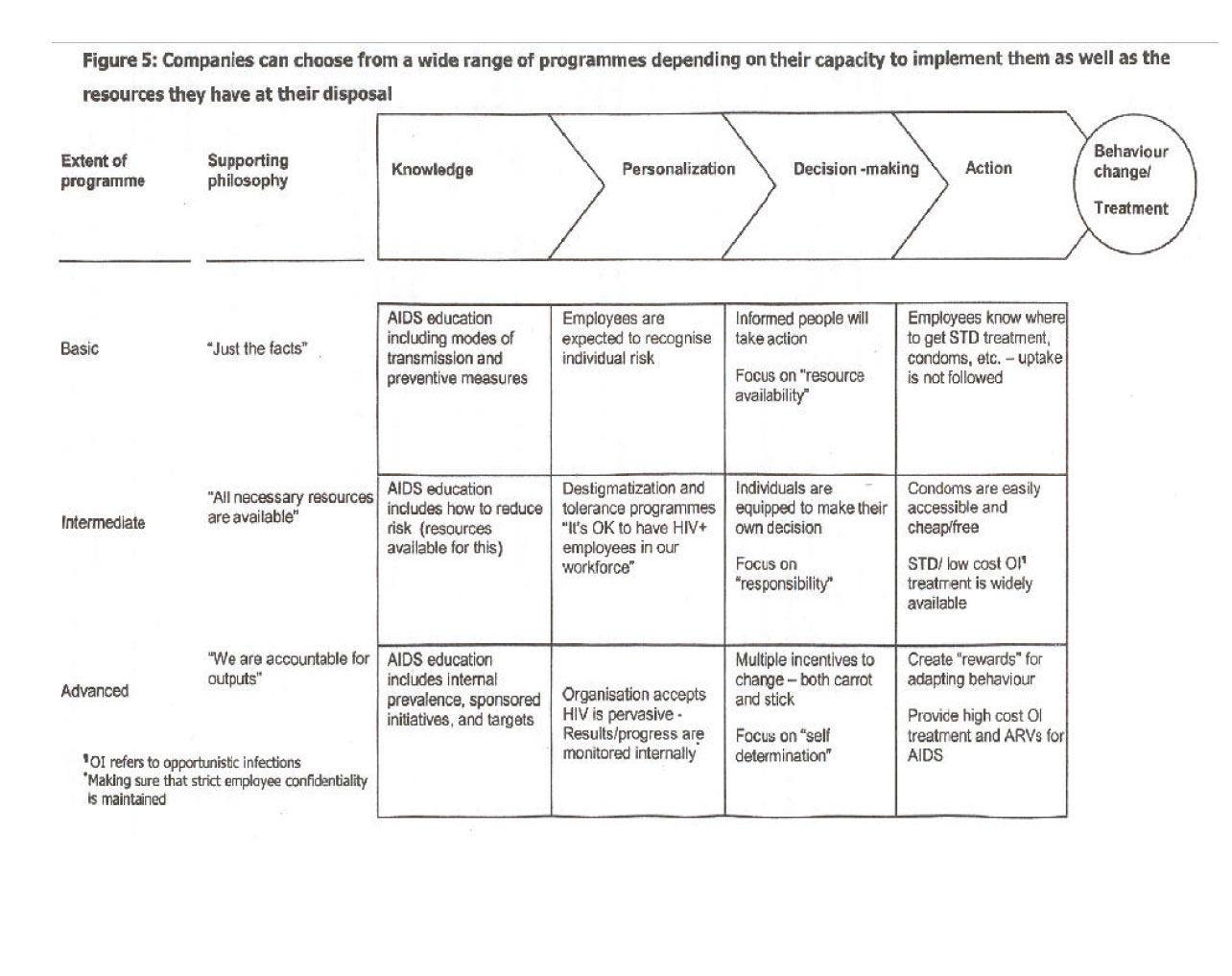
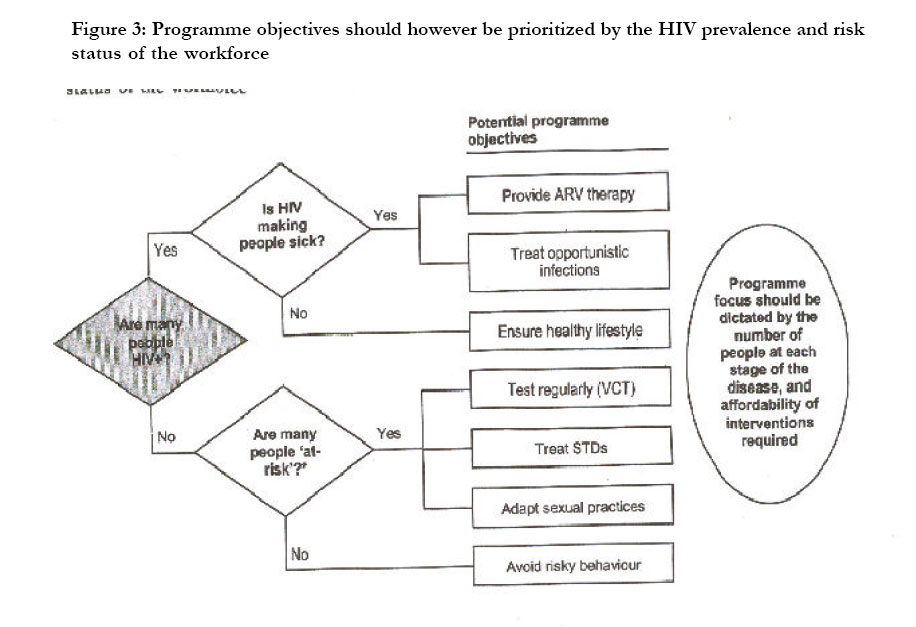
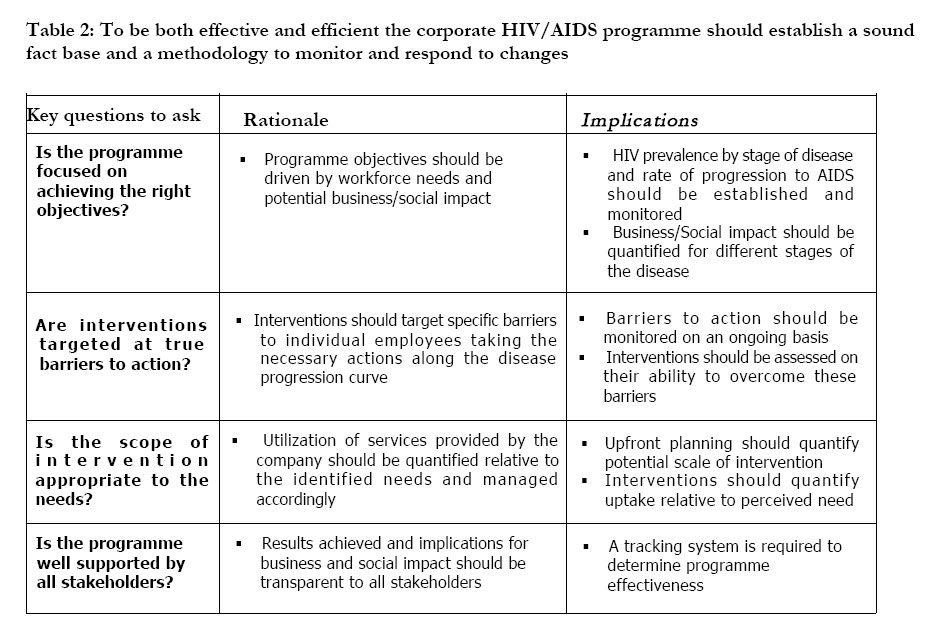
Sources of internal costs of HIV/AIDS to businesses are outlined in Table 1 below. The type of programme an individual company should run can range from basic to advanced depending on such factors as the workforce needs, expenditure required to run a programme vis-a vis the company’s finances, and other amount of collaboration that exists with other stakeholders. Companies should seek as much as possible not to duplicate programmes that are easily accessible to their workforce and to provide interventions in the most cost effective manner possible. For example, Voluntary counseling and testing (VCT) services are already freely provided at a number of sites within the country, the role of companies here may be as basic as trying to destigmatize the issue of HIV/AIDS within their workforce and to encourage employees to utilize these services. Figure 5 is an illustration about the range of components that can be included in a basic, intermediate and advanced HIV/AIDS control programme along a ‘Knowledge-Personalization-Decision-Action’ funnel for individual employees. CONCLUSIONSThis paper proposes a framework through which businesses can think about how they can get involved in sharing the burden of HIV/AIDS in Uganda more equitably. We are not suggesting that companies bear all the costs of treatment for their HIV infected workforce. Co-payment schemes whereby affected employees can contribute to the treatment fund should also be explored, in addition to trying to source for additional funding for the more costly interventions from international donor organizations. By adopting strategies like these; the burden sharing even for AIDS management can be made affordable at least for a larger proportion of the affected population even in high burden but resource limited settings like Uganda. Organizations like the Uganda Business Coalition on HIV/AIDS can assist in coordinating company response in the corporate sector. Currently one great advantage for those companies that would wish to pursue ‘advanced’ programmes (see Figure 5) for their employees is that the price of the treatment of some of the more common opportunistic infections has dropped dramatically. As an example; due to a great philanthropic effort by Pfizer, fluconazole, which only a few years ago was a prohibitively expensive drug used for the treatment of cryptococcal meningitis is now provided free of charge at major government hospitals. Additionally the cost of anti-retroviral therapy in Uganda has reduced more than 80% over the past four years thanks largely to a collaborative effort between high burden countries, UNAIDS, and the drug manufacturers. These noble efforts mean that for the first time since the advent of the HIV/AIDS epidemic, specialized treatment could become affordable to a large number of those infected and Uganda can finally complement the behavioural change strategies that have been the mainstay of controlling the epidemic for the last two decades. However, if the corporate sector is to be persuaded to make larger investments in care and treatment than is currently the case, there is an urgent need for further research and communication on several key issues. Notable among these are the following:
The onus is on health and economic researchers to do the relevant contextual research to provide the right answers to these germane issues that we have raised. REFERENCES
Copyright © 2002 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs02054f5.jpg] [hs02054f3.jpg] [hs02054f1.jpg] [hs02054t2.jpg] [hs02054f4.jpg] [hs02054f2.jpg] [hs02054t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}