 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences Vol 3, No 1, April 2003, pp 7 - 14. Family communication about HIV/AIDS and sexual behaviour among senior secondary school students in Accra, Ghana Samuel Adu-Mireku Department of Social Sciences, Fayetteville State University, 1200 Murchison Road, Fayetteville, NC 28301, USA Correspondence to: Samuel Adu-Mireku
Department of Social Sciences
Fayetteville State University,
1200 Murchison Road
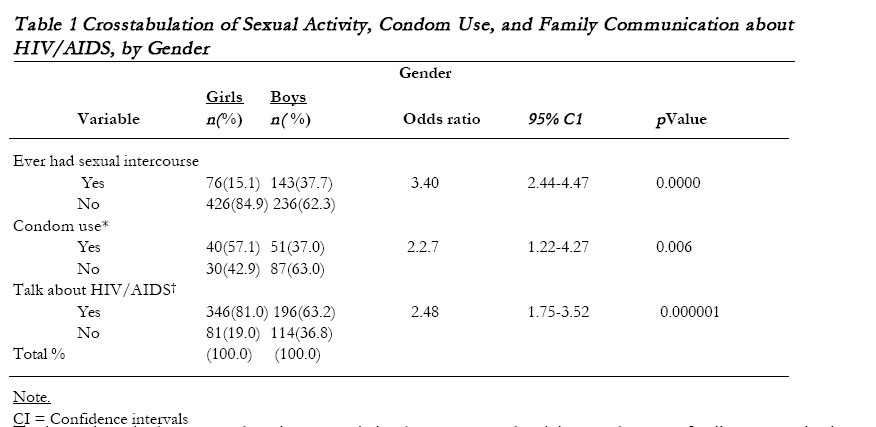
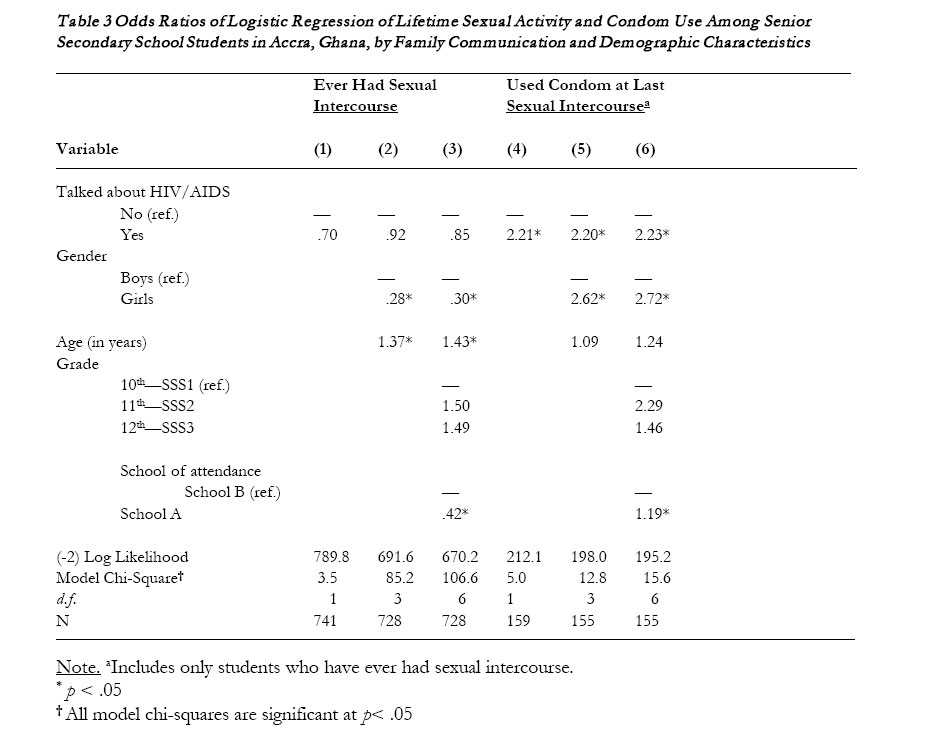
Fayetteville, NC 28301, USA Code Number: hs03003 ABSTRACT Background: Sexually active adolescents in Ghana are increasingly at risk of HIV and other sexually transmitted infections. As a primary agent of socialization, the family can exert a strong influence on adolescent sexual behaviour. Therefore, to aid in the design and implementation of effective prevention programmes, it is important to understand the role of the family in influencing sexual behaviour among school-going adolescents. Key words : Ghana, adolescent health, risky sexual behaviour, condom use, gender differences. INTRODUCTION As the HIV/AIDS epidemic continues to create serious public health concerns in Ghana and other sub-Saharan African countries, there is an urgent need to better understand the social processes and factors that influence sexual behaviour so that effective prevention programmes can be designed and implemented. Any such effort must begin with a focus on adolescents and young people, whose responsible sexual behaviours are more likely to positively impact the current struggle against the HIV/AIDS epidemic1 . The factual bas indicate1 , today, more than half of new infected HIV cases are among persons between the ages of 15 and 24. In Ghana, it is estimated that 1.2 million people will be living with HIV/AIDS by the year 2005, with the majority expected to be adolescents and young people2 . This estimate is not surprising because previous studies on adolescents and youth in Ghana have documented that they are engaging in sexual activities; they are doing so at an early age; and they are not using condoms consistently 3-8 . By engaging in risky sexual behaviours, adolescents and youth in Ghana face a number of serious negative health consequences, including placing themselves at risk of acquiring HIV and other sexually transmitted diseases. In light of the previous findings, research efforts must continue to identify the social factors and processes that are likely to positively impact the sexual behaviours of adolescents in the country. For many years, because the family plays a primary role in the socialization of children, researchers have focused on how family members influence adolescent sexual behaviour. In the United States, for example, a large body of research has examined the relationship between parent-adolescent communication about sexual issues, including HIV/AIDS, and sexual behaviour9-11. The findings from the U.S. studies, so far, have yielded inconsistent results. The majority of the studies, however, have reported that adolescents who discussed sexual issues, including HIV/AIDS, with parents were less likely than those who did not to engage in risky sexual behaviours9, 12-13. In Ghana, to date, none of the studies on adolescents and youth has examined this important question of whether or not students are communicating with their parents and other family members about HIV/AIDS, and whether or not such family communication is associated with safer sexual behaviour. An extension of cross-cultural research on this topic to Ghanaian adolescents is important for two main reasons. First, in Ghana, as in the United States, the institution of the family plays a significant role in the life of adolescents. Therefore, research efforts in Ghana should focus on how the family influences sexual behaviours of adolescents. Ultimately, significant findings from such research should help in the effort to design and implement feasible HIV/AIDS prevention programmes. Second, considering the health risks posed to Ghanaian school-age adolescents that are sexually active, the lack of data and research that examine the association between sexual activities, risk behaviours, and family communication, is a major gap in the existing literature on adolescents and youth in Ghana. This study, therefore, examined the association between student-family communication about HIV/AIDS and sexual activity and condom use among Senior Secondary School (SSS) students in Accra, Ghana. Following previous studies in the U.S.9-13, this study also examined whether or not there are socio-demographic differences in student-family communication about HIV/AIDS, sexual activity, and condom use. However, unlike previous studies on adolescents and youth in Ghana, this study focused exclusively on schoolgoing adolescents. By focusing exclusively on secondary school students in Ghana, it might be easier to measure the success or failure of prevention efforts against school-going adolescent mortality and morbidity as well as enhance ongoing health education programmes and policies within the context of schools. METHOD Data collection procedures and sample The setting for this study was Accra. With a population of 1.67 million, the Accra metropolitan area is the most urbanized region in Ghana (14). Data for the study were collected during a five-week period—from July to August 2000. Two schools were randomly selected from a list of senior secondary schools in Accra. The two schools, labelled ‘A’ and ‘B’, have three grade levels—SSS1 (10th grade), SSS2 (11th grade), and SSS3 (12th grade). School A enrolled more students than School B (1863 vs. 1301), but the gender distribution at the two schools was comparable (59.9% girls in School A vs. 58.1% girls in School B). Slightly more residential students were enrolled in School A than in School B (24.2% vs. 19.3%). School A is located in one of the best residential communities in Accra, and its buildings and campus are more attractive. Administrators at the two schools indicated that students in School A have higher socio-economic backgrounds. Initially, a sample of 1000 students from both schools was randomly selected based on the number of classes in each grade. With a response rate of 89.4%, the sample size was 894 students from both schools. Instrument Because of its established reliability and extensive use in the United States and other countries, a slightly modified version of the 1999 Youth Risk Behavior Survey (YRBS) questionnaire, an instrument which was developed by the Centers for Disease Control and Prevention (CDC), was used to collect data for the study15, 16 . The survey included questions on tobacco use, alcohol use, marijuana use, sexual activity, condom use, and other risk behaviours. In this article, questions dealing with family communication, sexual activity, and condom use are analysed. Ghana Education Service (GES), a unit of the country’s Ministry of Education, reviewed the questionnaire and approved the survey. Administrators at the two selected schools also reviewed the questionnaire and endorsed the Ministry’s approval for the survey to be administered. The survey was administered with the assistance of a female graduate student from a local university. Completing the survey was voluntary, and respondents were advised of their right to decline participation at any time. In addition, respondents were advised that they could refuse to answer or leave blank any question they found uncomfortable. The questionnaires were not precoded to ensure anonymity of students. Measures Sexual activity. Students were asked whether they have ever had sexual intercourse, with yes = 1, no = 0 response options. Previous studies17 have distinguished between sexual experience (a student who has had sexual intercourse at least once in her or his lifetime) and current sexual activity (a student who has had sexual intercourse in the past three months). The present analysis includes only sexual experience. Condom use. Students were asked whether they or their partners used a condom during the last time they had sexual intercourse. The two response options were yes = 1, no = 0. In Ghana, the main mode of transmission of HIV is sexual intercourse2, 18 . Therefore, the rate of condom use among adolescents is a key determinant of exposure to sexual risks and it is included in the present study. Student-family communication. Students were asked whether they have ever talked about HIV/AIDS with their parents or other adults in their family. The response options were dichotomised as yes = 1, no = 0. Other adults are included in family communication because of the role of the extendedfamily in the social structure of Ghana19 . Gender. The question, ‘What is your sex?’ measured this variable. The coding categories were girls = 1, boys = 0. Previous studies have noted the need to examine gender differences in sexual activity and sexual risk behaviours, especially among adolescents and youth20 . Age. Asking students to respond to the question, ‘What is your age?’ measured this variable. Age is measured as a continuous variable. Grade level. The three grade levels were coded into a dummy variable (SSS1—10th grade = 0; SSS2—11th grade = 1; SSS3—12th grade = 2). School. A dummy variable was created for the two schools to test whether the schools differed significantly in relationship to the outcome variables. The coding categories were School A = 1, School B = 0. Data analysis The data were analysed using SPSS for Windows Version 11.0 software21, 22 . Descriptive analyses were conducted by calculating the frequency distribution of gender and other study variables. To test for statistically significant associations between sexual activity, condom use, and family communication about HIV/AIDS and gender, a series of chisquare analyses were conducted. A second set of chi-square analyses was done to test the association between the three variables and school of attendance. With two dichotomous dependent variables, logistic regression was used to estimate the effect of family communication and demographic variables on sexual activity and condom use. The analyses for the two dependent variables were done in three steps. In step 1, the effect of only family communication on the dependent variables was assessed. Next, in step 2, gender and age were added as controls to the first model. These two key demographic variables are important because previous studies have reported differential effects of communication on sexual behaviour among adolescents, depending on their gender and age9,10, 12. Finally, in step 3, grade level and school of attendance were added to the second model. In steps 2 and 3, the effect of family communication on the outcome variables and controlling for the added variables were examined. The results are presented as odds ratios, which estimate the effect on the odds of the outcome variable for each unit change in the independent variable. For dichotomous independent variables, odds ratios measure the effect of being in one category (girls) compared to another (boys). If the odds ratio is less than 1, it indicates a decrease in the odds of the outcome; odds ratios greater than 1 indicate an increase in the outcome; and odds ratios equal to 1 indicate no effect23 . Diagnostics tests did not indicate multicollinearity among the variables. The alpha level to determine significance for all statistical tests was set at .05. RESULTS Descriptive analysis Before presenting the results of the multivariate logistic regression models, it is instructive to present descriptive information about the sample and variables. The sample was composed of 56.9% girls and 43.1% boys, which is representative of the gender distribution of the student population at the two schools. The mean age of respondents was 17.4 years (SD = 1.40). Overall, 25% reported that they have ever had sexual intercourse (i.e., they are sexually experienced). Of those who were sexually experienced, 25.7% had their first sexual intercourse at age 11 years or younger; and by 16 years, 64.7% had had their first sexual intercourse. The descriptive analyses also examined condom use among the respondents who are sexually experienced. The finding indicates that 55.7% of the students responded that they or their partners did not use a condom at last sexual intercourse. In Table 1, the results of chi-square analyses of sexual activity, condom use, and family communication by gender are presented. Table 1 shows that boys were more likely than girls to have ever had sexual intercourse, that is, to be sexually experienced (odds ratio = 2.44; 95% CI = 2.44-4.74). Table 1 also shows significant gender differences in whether respondents or their partners used a condom at last sexual intercourse. Boys were less likely than girls to report condom use (odds ratio = 2.2.7; 95% CI = 1.22-4.27). Furthermore, boys were less likely than girls to have ever talked about HIV/AIDS with their parents or other family members (odds ratio = 2.48; 95% CI = 1.75-3.52). Multivariate analysis Results from the logistic regression analyses of family communication on sexual activity and condom use are presented in Table 3. Columns 1, 2, and 3 show the relative odds that students were sexually experienced. Column 1 shows that family communication about HIV/ AIDS by itself has no significant influence on being sexually experienced. Given that prior research has noted the importance of demographic characteristics in sexual activity, in column 2, gender and age are added as controls. The results indicate that girls are less likely than boys to be sexually experienced (OR = .28). That is, the odds of being sexually experienced are 72% less likely for girls than boys. Column 2 also shows that age is associated with being sexually experienced. For a year’s increase in age, the odds of being sexually experienced increase by a factor of 1.37. Controlling for gender and age, however, does not affect the effect of family communication on sexual experience, which remains insignificant. In column 3, grade level and school of attendance are included as additional controls. The results show that being sexually experienced is associated with the school a student attends (OR = .42), but not with grade level. Respondents who attend School A are 58% less likely than students who attend School B to be sexually experienced. Column 3 also shows that, controlling for these factors hardly affected the effect of gender and age on being sexually experienced. Furthermore, controlling for all four factors did not affect the effect of family communication about HIV/AIDS on being sexually experienced, which remains insignificant. Columns 4, 5, and 6 show the relative odds of using a condom at last sexual intercourse. The results in column 4 indicate that respondents who have ever talked about HIV/AIDS with parents or other family members are significantly more likely than those who have never talked with parents or other family members to report condom use at last sexual intercourse (OR = 2.21). In column 5, gender and age are added as controls. The results indicate that condom use is significantly associated with gender, but not with age. Girls were significantly more likely than boys to report condom use at last sexual intercourse (OR = 2.62). Controlling for the two variables appear to have little effect on the association between family communication and condom use. Finally, in column 6, grade level and school of attendance are added as additional controls to column 5. As indicated in column 6, condom use is significantly associated with school of attendance, but not with grade level. The odds of using a condom at last sexual intercourse is greater for respondents who attend School A than for those who attend School B (OR = 1.19). By comparing columns 5 and 6, the results show that the addition of grade and school of attendance hardly affected the effect of family communication and gender on condom use. DISCUSSION This study examined sexual activity and condom use and the extent to which they are affected by family communication about HIV/AIDS among a sample of senior secondary school students in Accra, Ghana. The findings of the study are noteworthy. A quarter of the students had engaged in sexual intercourse, with boys more likely to do so than girls. Similarly, a quarter of the sexually experienced students initiated sexual intercourse when they were 11 years old or younger, and by the age of 16, over 64 percent had already initiated sexual activity. These findings suggest that information about sexual activity must be conveyed to students early. The findings also indicated that the sexually experienced students are at great risk of exposure to HIV and other sexually transmitted diseases. It is notable that only 44.3% of the sexually experienced students reported that they or their partners did use a condom at last sexual intercourse. Adih and Alexander (1996) reported a much lower percent of condom use at last sexual intercourse in their study of youth in Ghana3 . The present finding suggests the urgent need for students to receive information about condom use before initiating sexual intercourse. In addition, considering that 25.7% of the sexually experienced students had initiated first sexual intercourse at age 11 years or younger, this information must be given at an early age. The most important finding of this study is the association between family communication about HIV/ AIDS and condom use. This finding is consistent with previous studies that have shown the importance of family communication about sexual issues9 . The present result is encouraging because the increased use of condoms attributable to family communication is likely to reduce sexually related risks among sexually active school-age adolescents in Ghana. It may, however, be necessary in future research to build upon the present finding and examine additional aspects of family communication, especially the role of fathers and mothers. The assessment of each parent’s role in family communication is critical in a society such as Ghana, where traditional norms greatly inhibit discussions of sexual issues with parents, especially with fathers. Another important finding is the significant association between sexual activity, condom use, and school of attendance. Students attending School A, which has better facilities were less likely to be sexually experienced but more likely to use a condom. Differences in socioeconomic background of students at the two schools may be one plausible explanation. Another possible explanation may be due to the content and process of family communication, which cannot be determined from the data of the present study. It would be insightful for future research to collect data on these factors in order to better explain the role of school of attendance in sexual behaviours. Implications of the study The findings of this study have implications for health educators and health care practitioners seeking to better understand the prevalence of sexual activity and risk behaviours among school-age children in Ghana and perhaps other sub-Saharan African countries. The percentage of sexually experienced students who are not using condoms at sexual intercourse suggests that current educational efforts and strategies are inadequate. The findings of this study suggest that school-based interventions programmes must involve parents because of the strong association between family communication and condom use. Limitations of the study The implications of the study, however, need to be examined within the context of the study’s limitations. First, as an exploratory study, it was limited to two senior secondary schools in Accra. Being the capital city of Ghana, life in Accra is different from life in peri-urban and rural areas of the country. At the two selected schools, 77.8% of the students were non-residential. By contrast, schools in peri-urban and rural areas of the country tend to have higher percentages of boarding (residential) students. Therefore, the student population from which the sample was drawn may differ from the population of students in schools located in peri-urban and rural areas of the country in terms of contextual factors. Second, the data analysed for this study are cross-sectional; therefore, no definitive statements regarding the causal relations between family communication and the outcome variables can be made. CONCLUSION These limitations notwithstanding, the findings of this study contribute significantly to the growing literature on adolescents in Ghana. The next logical step for future research is to use the YRBS questionnaire to conduct a nationwide survey of junior and secondary school students in Ghana. The addition of junior secondary schools to the population of schools in this study is critical because of the reported early initiation of sexual intercourse. Furthermore, the inclusion of students from peri-urban and rural schools will address one of the limitations of the present study. In addition, there is a need to examine the content of discussions between students and family members as well as the extent to which outcomes of such discussions are dependent upon the sex of students and family members. In conclusion, the findings of this study should provide baseline data to which future surveys using the YRBS questionnaire may be compared. ACKNOWLEDGEMENTS I would like to thank Vida Benson for her assistance in data collection. REFERENCES
Copyright © 2003 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs03003t3.jpg] [hs03003t2.jpg] [hs03003t1.jpg] |
| |||||||||

{kind=link}
{kind=link}