 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
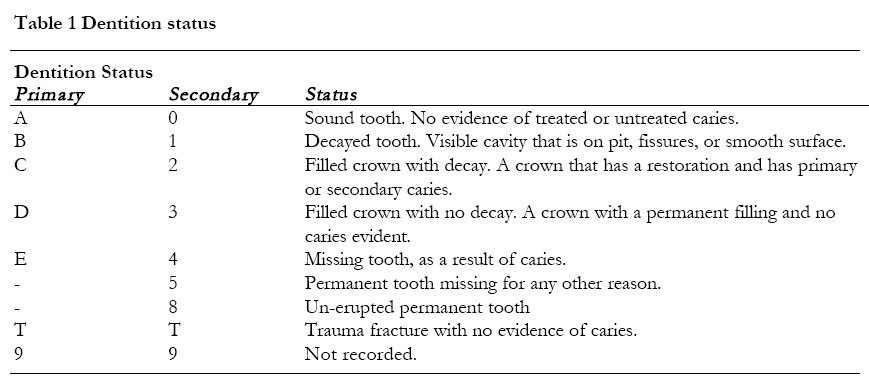
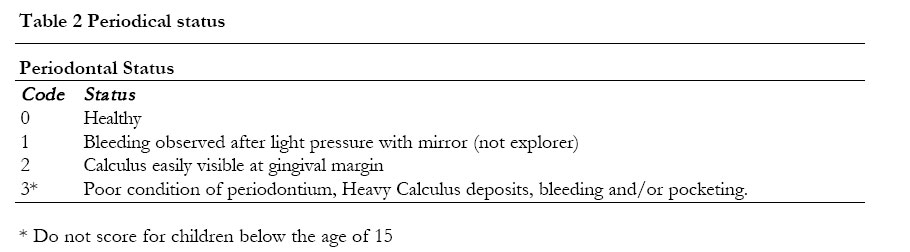
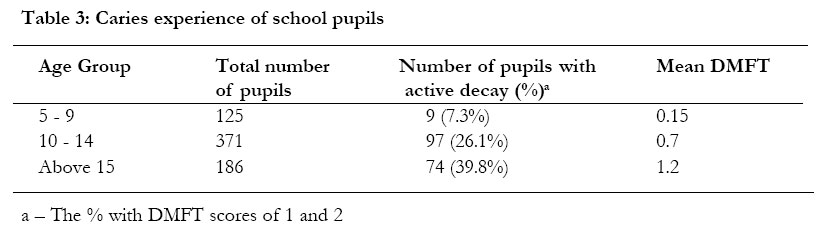
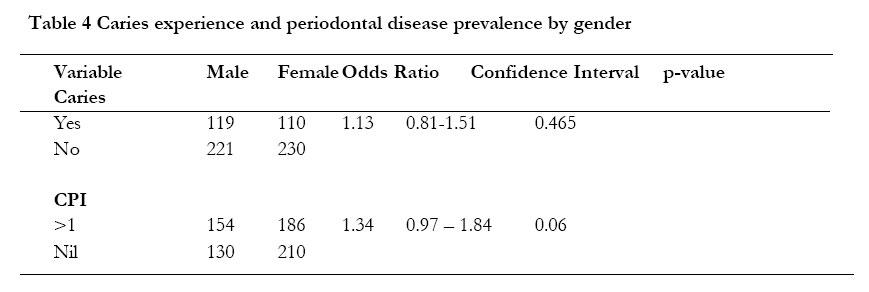
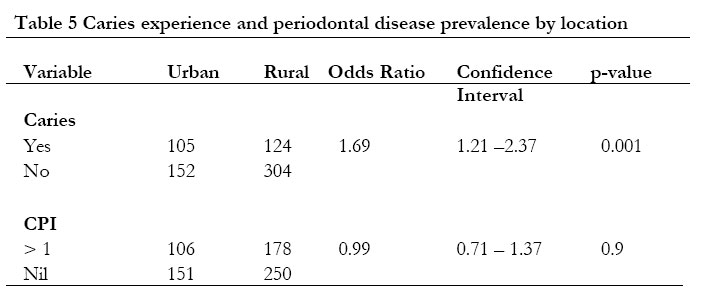
African Health Sciences 2003; Vol. 3 , No. 1, pp. 19 - 22 Baseline survey of oral health of primary and secondary school pupils in Uganda. *Margaret Wandera1 and J Twa-Twa2 1-University Hospital, Makerere University Kampala, Uganda. *Correspondence: Dr. Margaret Wandera, P. O. Box 5164, Kampala, Uganda. Tel; 077-415291 Email: mawandy@hotmail.com Code Number: hs03005 ABSTRACT Background: Among the issues that determine the performance of a child at school is health. In recognition of this, the Uganda government has embarked on a school health program for the success of universal primary education. Although dental health is an important component of school health there is little information on it. Objective: This study aimed at collecting information on dental health of pupils in school for evaluation and planning. INTRODUCTION The Uganda government has embarked on a comprehensive school health program to ensure that universal education as a response to poverty alleviation succeeds. It is thereby committed to empowering children and adolescents with knowledge and skills that enable them to practice healthy living. Furthermore, the school age children 6-17 years and 18-24 years make up 37% and 13% respectively of the population of Uganda, providing a favorable group to undertake health interventions. The environment, that is, existing infrastructure, available services, feeding programs), community and individual health practices determine the health of children in school. A planned and sustained campaign to eradicate or minimize the causes and outcomes of poor health in schools requires good health data of the existing situation. Oral diseases were identified among the common diseases that interfere with schoolwork due to the fact that the common oral diseases; dental caries and periodontitis, tend to cause pain and discomfort subsequently leading to absenteeism and poor performance. There is no adequate data on these conditions in relation to Uganda school health, however, there is population based data that report on increase of dental caries with age. The studies observed high prevalence of periodontal disease in all age groups and report endemic dental fluorosis in some parts of the country 1,2,3. . These observations need to be affirmed for this age group. WHO4 recommends development of Oral health services and manpower structures, data in addition to being available, should be recent because of the observed changing trends seen in various populations. OBJECTIVES The School Health Baseline Survey aimed at assessing the health status and health determinants of school pupils in Uganda. The Uganda government has set up a school health program, which will use the information gathered to strengthen medical and dental care services for school pupils. This paper deals specifically with oral health, where the prevalence of dental caries, periodontal disease and fluorosis were assessed. MATERIALS AND METHOD Sample size. The overall sample size was determined using a cluster sampling technique with a design effect of 1.58, homogeneity of 0.02(general disease) and assuming a prevalence of 50% of whom 30% (945) were for clinical examination. The design was computed with a 5% confidence. Sample population. A multistage cluster sampling technique was used to select children from 5 districts. The districts were representative of 5 regions: North, East, Central, West and the capital city, Kampala. At the district level, schools were selected from 2 sub-counties, one urban and one rural. Primary and secondary schools visited had to be registered with the government, and had to have all classes. Since there were more primary than secondary schools5 the recruitment ratio was 6:1 (primary: secondary). Individuals were randomly selected from every class in the selected schools, grade one to grade seven and secondary one to secondary six. Oral examination. Five Public Health Dental Assistants were trained on how to score using standardized simplified versions of Decayed Missing and Filled teeth (DMFT and Community Periodontal Index-CPI6 (see Table 1 and 2). They also recorded presence of dental fluorosis. There was no distinction made on the level of severity of dental fluorosis. A value of 1 was given for presence of fluorosis and 0 (zero) when no fluorosis was observed on the teeth. The methods were pilot tested and adjusted for the main study. All Oral examinations were done with a mouth mirror and an explorer using natural light. Permission to conduct the study was obtained from the Ministry of Education and Sports, Ministry of Health, Uganda National Council of Science and Technology, District Leaders and Head teachers. Data analysis was done with Statistical Package for Social Scientists (SPSS® ). RESULTS A total of 685 pupils (342 male, 343 female) were clinically examined. The age ranged from 5 to 22 years. The distribution of the children is shown in the Figures 1 and 2. Dental Caries. DMFT scoring found of all the children to be caries-free and 33.4% (229) had caries experience, of whom 26.3%(180) had active decay. The mean DMFT of the entire group was calculated as 0.7 (sd:1.4) with D-component accounting for 78%. Pearson’s chi-square statistic of bi-variate association was calculated and revealed a significant relationship (p<0.001) between the age of an individual and DMFT. The urban school children had higher caries prevalence than the rural school children, found to be statistically significant (p=0.001) (See tables 3 and 4). Periodontal Status. Fifty nine percent of the children had a healthy periodontium. Forty one percent (284) had at least 1 affected sextant. There was no remarkable variation in this distribution regardless of location and sex as shown in table 5. In the individuals above 15 years, severe periodontal involvement, e.g. pocketing was seen in 9.6 %(18). Fluorosis. 16.6% (113) of the children were found to have some degree of fluorosis with a higher proportion 84% (95) of them attending rural schools. The school children of Kabale and Mbale contributed 36.3%(41) and 38.1%(43) respectively to the population found with fluorosis. In Kabale this accounted for 45.5%(41) of all children examined, while in Mbale this was 29%(43). DISCUSSION In the event of Universal Primary Education these findings are a good representation of the school children in Uganda. WHO6 has recommended index ages and age groups for Oral Health surveys that have not been used here as the sample design of this ‘baseline survey’ was for additional clinical examinations besides the oral examinations. To overcome this, the data has been handled in age groups that can best represent the recommended index ages and age groups. Age profiles are useful in that they reveal information on trends and severity of disease. In this survey, prevalence of dental caries as shown by the mean DMFT of 0.7 is considered low4. The increasing prevalence with age is expected, however, there is also an increasing prevalence of dental caries in the Ugandan children over a period of 20 years. The reported mean DMFT of the 10 to 14 years old was 0.2 by Moller et al.2, then 0.45 by Tiromwe et al.3. This upward trend in developing countries has been attributed to some extent to change in traditional diets and socio-economic status7. This may also explain the higher prevalence of dental caries seen in urban as compared to rural populations. The D-component comprising 78% of the DMFT may reveal an unmet treatment need and needs further investigation. WHO4 quotes periodontal disease in approximately 50% of a population as moderate prevalence, therefore Uganda school children had a close to moderate prevalence in all categories of the population. This method did not use W.H.O periodontal probes therefore to minimize intraexaminer errors a simplified version of CPI had to be developed (Table 2). This may have led to under-reporting of marginal gingivitis. Previous studies, for example Tiromwe et al.3, who scored plaque found a prevalence over 80% in all age groups. This survey reveals moderate periodontal disease and rising dental caries prevalence. The increase in prevalence demonstrates an urgency of developing a program to control the disease levels rather than wait for unfavorable disease levels. Educating individuals on sound dietary habits and dental hygiene at schools reportedly is effective in control of these two conditions.8 It is therefore important for the Uganda government to include Oral Health Education at school as a preventive method in the school health program. At these disease levels W.H.O4 recommends interventions aimed at the following measurable goals, reduction of tooth loss due to caries and reduction gingivitis prevalence. Kabale and Mbale contributed the majority of the population with fluorosis. Kabale district lies within the Western branch of the African Rift Valley, while Mbale district is a mountainous region west of the Eastern branch of the African Rift Valley. The African Rift Valley is known to have endemic fluorosis primarily due to the high fluoride content in water9. Rural areas had higher dental fluorosis prevalence perhaps due to various water sources, unlike urban areas that tend to have piped water. It is hoped that this information stimulates interest in acquiring more and better information related to oral health and fluoride in Ugandan populations. This information can then be used to design preventive programs. CONCLUSION There is an upward trend in the caries prevalence. The Uganda government should design a preventive program to reverse the rising prevalence of caries, reduce prevalence of gingivitis, at the same time providing adequate services for the affected individuals. Furthermore, appropriate defluoridation programs should be considered to control fluorosis in the endemic areas. REFERENCES
Copyright © 2003 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs03005t3.jpg] [hs03005t1.jpg] [hs03005t5.jpg] [hs03005t2.jpg] [hs03005t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}