 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences Vol. 3, No. 1, April 2003, pp. 33-39 Screening for disability in a community: the ‘ten questions’ screen for children, in Bondo, Kenya. Emily Muga Partnerships Department, Tropical Institute of Community Health and Development (TICH) in Africa. Correspondence: Partnerships Department, Tropical Institute of Community Health and Development (TICH) in Africa. P.O Box 2224 Kisumu-Kenya, Tel: 254-35-44853/23972 E-mail: adminkisumu@tichinafrica.org Code Number: hs03007 ABSTRACT Background: Although the need for early identification and interventions of disabilities is evident, the current state of routine screening practice in Kenya needs intensive training of screeners before more rigorous techniques are introduced. INTRODUCTION AND BACKGROUND The 1989 Kenyan population census revealed that persons with disabilities constitute 6 % of the population of 21 millions. Currently, about 1.7 million persons in Kenya have disabilities1 . This is a significant portion of the population and might continue to increase due to rapid population growth. There is still a wide disparity between the needs of persons with disabilities and provision of services in Kenya. Without effective action, the major consequences of disabilities will be an increase in the number of dependents. Most of the disabling conditions are preventable, with malnutrition, birth trauma, accidents, and inadequate prevention and treatment of communicable diseases contributing to the majority of disabilities. Screening and therapeutic services for disabled children are relatively sparse and expensive. Availability of those services to children is often related to the ability of parents to identify the impairment, seek advice and pay for the service with limited access to specialized services. Yet most people with disabilities live in rural poor communities. In Kenya few children are being screened for disability2. There is need for programs, which provide services for early identification and intervention for disabled children irrespective of whether the disability happens before, during or after birth2 . The training and education of disabled children begin only when the child reaches school age or later, instead of beginning at an early age. Today, almost two thirds of all disabled children are incorrectly placed due to lack of proper assessment before the children are admitted to the special schools, and only a small proportion of disabled children receive formal education. Due to the large number of children to be screened, any method of case identification that is to be recommended for use in developing countries must be, at once, sensitive, specific, inexpensive, simple and accurate3 . The requirement of accuracy is the most difficult to satisfy. Educational Assessment and Resource Centers (EARC) in Kenya. In Kenya, there are 52 district-based EARC countrywide complimented by 345 sub-centers all involved in assessment and advice of the parents of children with disabilities3. EARC main objective is to equalize education opportunities for children with special needs and facilitate their full integration into the school system and their community. This approach includes early identification of children with special education needs, sensitization, counseling and training of disabled children and their families, parents, teachers, local administration and others in meeting the special needs of these children. It also emphasizes prevention of disabling conditions, creation of public awareness on disability and handicap and early intervention and integration of these children in the school system. EARC is established in an existing special school or a unit for the disabled children in a regular school for all disabled children aged 0-16 years for psychological and educational assessment. This assessment presupposes that the child will voluntarily or involuntarily exhibit some behavior that can either be observed or recorded. This is then compared with the behavior of a non-disabled child of the same age to determine whether it is normal, deviant or delayed. To date, 80,000 children have been identified. There is recognition that a lot more have not been reached1. The capacity of the existing special education schools and institutions is 10,300 and approximately 11,700 children have been integrated in the main stream. The ‘Ten Questions’ Screen. The ‘ten questions’ is the process of growth towards standardizing criteria and methods (cheap and more accessible) of examination for recognition of disabilities in community settings. It is an instrument for screening disabilities in children (appendix II). It contains ten questions and probe questions that follow each of the questions. The questions are intended to be appropriate and useful for detecting disabilities in virtually all cultures and for all children aged 2-9 years. The checklist is translated into the local language. The ten questions were tested previously in the International Pilot Study on Severe Childhood Disability (IPSSD)4 and found to be sensitive for detecting severe mental retardation. However, they were also found to generate excess false positives. The purpose of the probe (in the ten questions) is to distinguish children who are truly disabled from those who are not. The usefulness of the probe has been investigated in the studies carried out in Bangladesh5, Jamaica6. A survey carried out in Dhaka, Bangladesh, as part of a collaborative study to test the validity of the questionnaire (‘ten question’) for screening serious childhood disabilities found that approximately 7 % of the children were positive on the screen. The sensitivity, specificity and negative predictive value of the ‘ten questions’ were perfect or near perfect for the severe and moderate (serious) disabilities. The positive predictive value was only 22%, but 70% of children classified as false positive were having mild disabilities or other conditions for which early detection and treatment could be beneficial. No major age and gender differences in the validity of the questionnaire were apparent5. Another study using the ‘ten questions’ to identify disabilities in children aged 2-9 years in Clarendon, Jamaica, found that sensitivity of the ‘ten questions’ as a whole varied in different strata of the group and amongst different disabilities, from perfect in girls under 6 years, fits and motor disabilities and for serious disability in all groups except boys over 5 years with cognitive disability. Specificity was good but the false positive rate was unacceptably high (74 %)6. Numerous studies have demonstrated that early intervention programs do have a positive effect on the young disabled child’s development. The increased understanding of the importance of the early years for the normal child’s development and of the relation between early environmental factors and general development have influenced the understanding of the importance of the very early years also for the disabled children, who may be especially vulnerable and sensitive to the early experiences8. The early years represent not only the most rapid development in all areas of human development but they are also critical and irreversible. It is possible that if problems are identified early, intervention can remedy the problem of some children; limit the effect of the disability and prevent the development of secondary disabilities in many children8. Study objectivesThe objectives of the study were to
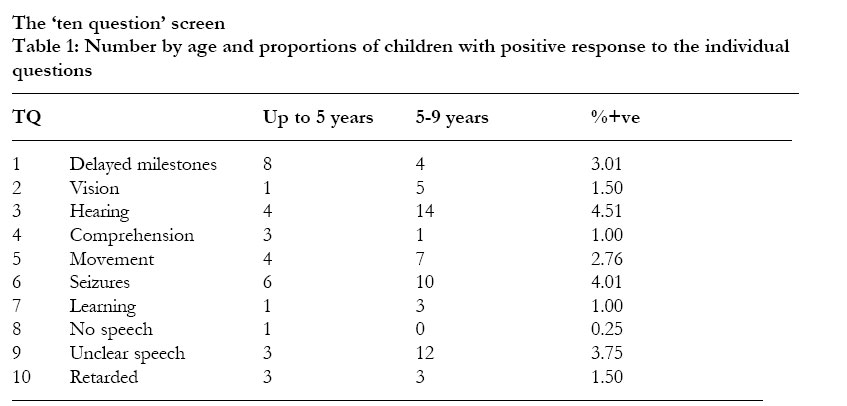
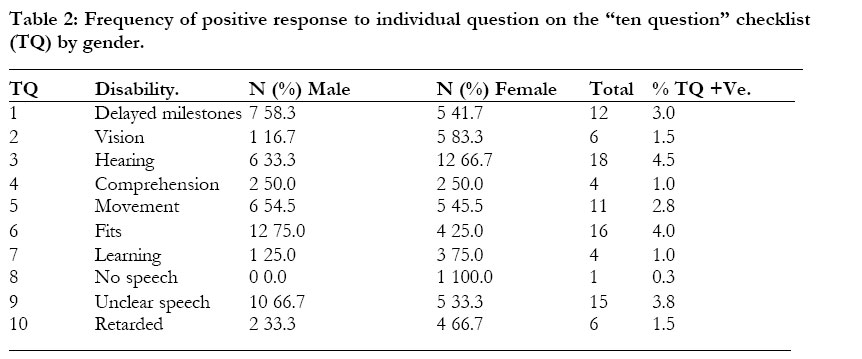
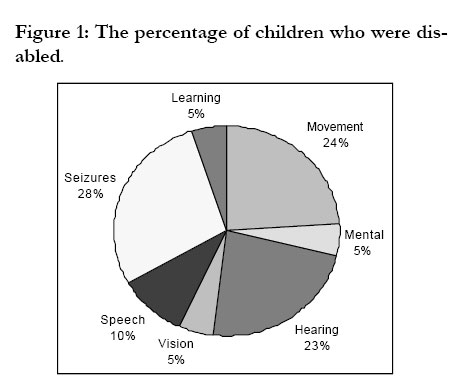
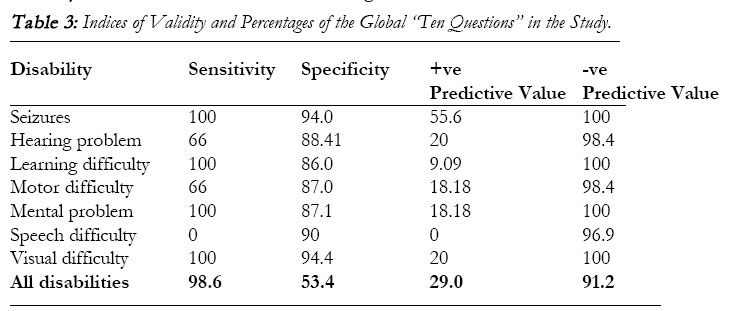
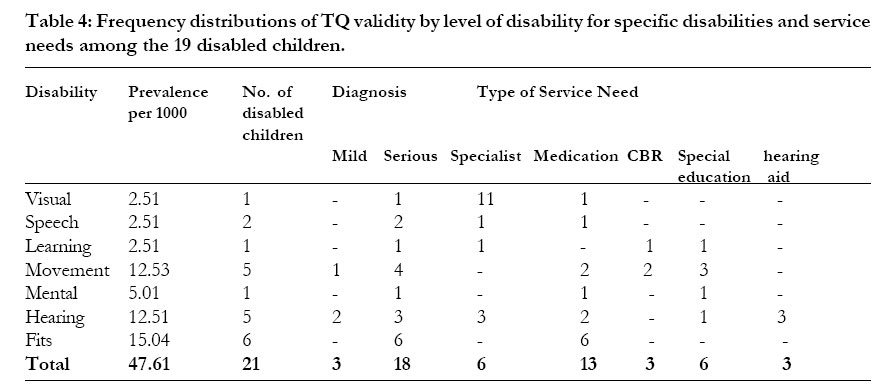
Research Design A comparative study was conducted using quantitative research methodology via a multi-stage data collection procedure. First, the EARC assessment personnel independently carried out the assessment of the children in the sub location. They announced the exercise in the sub location’s “barazas”, churches, markets, health facilities and schools and conducted it as routine. A house-tohouse survey using the “‘ten questions’” screen followed. The structured interview checklist (the “‘ten questions’”) and a guide to collect background information were administered in a face-to-face interview of the child’s caregivers. Then, a postscreening verification test was carried out among some of the children identified as disabled on the basis of the ‘ten questions’ house-to-house survey method (that had not been identified by EARC assessment in the first stage). The same number of children assumed normal by the ‘ten questions’ house-to-house survey method was also included in this exercise. The three EARC assessment personnel each visited these children independently for verification. The Sample Design There is a multi-stage sampling in this study. The population to be sampled was identified (2 - 9 year olds). Next, all the sampled children were stratified by villages and listed. The last stage was the assignment of the measures of size and selection11. The 6 villages of the sub location were used as the study clusters in the house-to-house survey. Mapping to track all the children age 2-9 years old within the clusters followed. At the verification stage, purposive sampling was used. Data Analysis The data was edited, processed, tabulated and analyzed by the statistical package for social sciences (SPSS) using both descriptive statistics and analytical methods. To test for independence of various classifications in the cross tabulations, the chi-squared test was used. Cross-tabulating the results from the ‘ten questions’ results and the EARC assessment results as the gold standard carried out the test of specificity, sensitivity and predictive value. Quality ControlThe questionnaire was developed in English and translated into Dholuo (the local language) and re-translated back to English by two independent persons. A third person moderated the final questionnaire. All forms used in data collection were translated in Dholuo using the translated version. RESULTSBackground of the children aged 2 – 9 years within the study area. The study covered 399 children. 206 (51.6 %) were male and 193 (48.4 %) were female. The majority (four-yearolds) were 66 children (16.5 %) and the lowest (nine-yearolds) were 32 children (8.0 %). Children under five constituted 54.6 %. The average number of children 2-9 years per mother was two. Births within health institutions constituted 71 %. Over 70 % of the persons responding to the questions were mothers of the children, 3 % fathers. 21 % were the child’s relative and 0.3 % was the child’s sibling. 98 % of the respondents were taking care of the children on a daily basis. The EARC screen.During the EARC screen, three children were from the study sub location and in the target age range representing hearing problems, mental retardation and motor difficulties each. An informal interview with the mothers of these children revealed that they attended the screening on the teachers’ advice that the children should be taken to special schools. The EARC screen is a requirement for the special school placement. Many people do not realize the existence of the EARC screen until they have a child who needs to be taken to special schools. The EARC screen is viewed as an initiative of the government implemented through the school system and not a community screen for disabilities. Its activities are geared towards educational placement of the children in different schools according to their appropriate conditions. The ‘ten questions’ screen. Table 1: Number by age and proportions of children with positiveresponse to the individual questions. Based on the ‘ten questions’ screen, 64 out of 399 children were disabled. All other ages had approximately 10 13 children with disabilities except for age 4 with 22 for age two with three only. On the last column, hearing problem presented a prevalence of 4.5 % and seizures was 4 %. The prevalence of disability in general was 16 %. Table 2. There were 64 disabled children and, 15 of them with multiple disabilities, therefore a total of 93 disabilities were identified. Seizures were often identified as accompanying other problems. 5 % have hearing impairment. Of the disabled children, 12 (3 %) of the sampled population were having problems of delay of normal development while 11 (3 %) have various movement difficulties. Post screening verification.Among the 72 children evaluated, only 19 children (15 boys and 4 girls) were confirmed to have a disability. It was in movement, seizures and hearing that five children were evaluated with disabilities. Out of the 19 children who were truly disabled, 15 (79 %) were boys. The chi square test result showed no statistical significance of this variation. The figure 1 above shows that fits constitute (28 %) the majority of all disabilities during the post verification of the “ten questions” screen. Movement disabilities consisted of 24 % and various hearing losses were 23 %. Speech difficulty was 10 %. Vision, mental and learning disabilities were 5 % each. Table 3. During the post verification stage, the sensitivity, specificity and negative predictive value of the ‘ten questions’ were found to be high. As in table 4, each disability had over 85 % except for speech and language development difficulty that was not sensitive to the screen. The positive predictive value was 20 % for visual and hearing problems, eighteen per cent for motor and mental difficulties, and 9.09 % for learning difficulty. The positive predictive value for seizures was 56 %. For all disabilities combined, sensitivity is 78.6 % and specificity is 53.5 %. The negative predictive value was 91.2 while the positive predictive value was only 29.0 %. The false positive rate was was 71 % and false negative rate was 8.8 %. Table 5 indicates that seizures had a prevalence rate of 15.04/1000. Movement and hearing represented 12.53/1000 and 2.51/1000 respectively. Speech, learning and vision had 2.51/ 1000 and mental had 5.01/1000. 18 of the disabled children were diagnosed with moderate and severe (serious) disabilities and three with mild disabilities. 13 children needed medical attention while six required specialist attention. Six other children needed special schools. Three children required community-based rehabilitation and hearing aid. DISCUSSIONSThe EARC Screen is a case defining process of measuring the existence and degree of disability in children. The study findings indicate that the parents usually seek this screen only when it is already known that the child has a problem and needs to be placed in a special school. The special schools never admit the children without recommendation and referral by the EARC personnel. Consequently, EARC services do not adequately identify all disabled children in the community. EARC also screens the children who are severely disabled leaving out children with mild disabilities and medical conditions which when left untreated could lead to possible disablement. Therefore, this screen is not practical in cases where there is need for prevention and treatment of conditions that could lead to disability. The several sets of tools and equipment used in the screen makes it cumbersome for developing countries where there are many children with potential disability are because of many potentially disabling conditions. Using the ‘ten questions’ screen, the prevalence of all disability in the study area was found to be 16 % of the population. Other studies using the global ‘ten questions’ screen also found a similar prevalence5. The study by Zaman and others5 found the prevalence of all disability as 16 % while the study by Thorburn and others found 18 %6. The results of the current study imply this tool can be used by community persons to screen for disabilities in children aged 2 – 9 years in their communities once the questionnaire is translated into the local language. The ‘ten questions’ is therefore, a sensitive screen for the six types of disabilities in 2 – 9 years old children with serious disabilities. The sensitivity is much lower for the cognitive disabilities. All children identified by the EARC as disabled were positive on the ‘ten questions’ screen. Even there is a high level of false positives with the ‘ten questions’, it can be used to screen all cases of disabilities in children aged 2 – 9 years in communities. However, with a positive predictive value of only 30 %, this screen cannot function on its own as a case-defining tool but should provide good basis for screening and referral for a more rigorous evaluation. The highest false positive rate was found in the question about hearing problems. All children found positive by the ‘ten questions’ instrument as having hearing impairment, had some ear discharges and/or infections of otitis media not receiving medical attention. Many parents neither gave appropriate care to ears of their children nor sought treatment for mild ear infection, which could lead to hearing loss. The parents do not associate these ear infections with deafness. Almost all children who had hearing loss had, at one time, had a severe attack of malaria, measles or mumps. Bondi found cerebral malaria as an important cause of neurological deficit, including hearing loss, in Nigerian children9. Stanfield explains that deafness in children is caused by damage to the nervous system by meningitis, cerebral malaria and others or result from chronic otitis media10. All the children who were screened by the ‘ten questions’ for motor problems were found to have physical disabilities. This maybe because normal and abnormal movement of the body parts are easily recognized. The ‘ten questions’ is an interview in which most responses are based on assumptions and conclusions derived from observation of behavior by the caregiver. This tool therefore identifies problems that are of great concern to families. Since the Kenyan government is not likely to provide for all the needs of the children at once, it is a pragmatic tool to use. Sensitivity depends on the awareness of the caregiver of the child’s behavior and whether that behavior is regarded as a problem. In Nyang’oma sub location where this study was conducted, this awareness using sensitivity as a criterion, is appropriate for seizures, learning, mental and visual disabilities. Its performance is high when all disabilities are combined and when hearing and motor disabilities coincide. It is however, imperfect for speech disabilities in which the concern is not significantly high to prompt action by the caregiver. Service need assessment: Service need assessment was done among all the children in the post verification evaluation. It is recognized that there is a huge gap between the needs of children with disabilities and the service provision. From the findings of this study, most children with disabilities in Nyang’oma sub location needed medical attention. In theory, most families have access to health services. However the cost of drugs and health seeking behavior of the people are also great determinants of access. These will almost certainly deter long-term treatment. Many needs of children with disabilities can be dealt with at the district level, and do not require highly specialized personnel. CONCLUSIONSThe EARC screen identifies accurately severe disabilities in all the children screened. It also specifically defines the degree and type of disability. The EARC method entirely depends on the ability of the teachers to identify any problem in the school child and advice. Ideally, in rural schools where the ratio of teacher to pupils is approximately 1:45, the teachers may not be particularly keen on affected children. Unless the problem is profound and the child has reached school age and is in school, it may be difficult to identify them using this screen. The ‘ten questions’ screen on the other hand screens children from their households. It gives a chance to all the children in the household including the younger children who are not yet in school, to be screened. Despite its high false positive rate, it offers a good basis for the disability expert to start designing community-based identification and intervention of the disabled children in the community. It helps create awareness about childhood disability in the community. Assuming that the number of children with disabilities is the same in rural Kenya and using the study finding as a guide, there is need for bridging the service gaps to help the children with disabilities realize their full potentials. It can be concluded that both the “ten questions” and EARC methods can be integrated into making the community identification of disabled children 2 9 years old. The ‘ten questions’ can be used to screen out potentially disabled children and then the EARC be used to diagnose the type and degree of the disability and refer the ill children for treatment. REFERENCES
Copyright © 2003 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs03007t4.jpg] [hs03007t1.jpg] [hs03007f1.jpg] [hs03007t3.jpg] [hs03007t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}