 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 3, No. 3, August, 2003, pp. 117-123 Sexual practices of women within six months of childbirth in Mulago hospital, Uganda Emmanuel Odar1, Julius Wandabwa2, Paul Kiondo21 Mulago hospital, P. O. Box 7051, Kampala, Uganda 2 Makerere Medical School, P. O. Box 7072 Kampala, Uganda Code Number: hs03021 ABSTRACT Objectives: To establish the sexual practices and their associated morbidity among women within 6 months of childbirth in Kampala Uganda. INTRODUCTION The postpartum period receives very little attention and care compared to pregnancy and labour in spite of the fact that the majority of maternal deaths and disabilities occur during this period. The attention usually shifts to the newborn baby and the mother gets little care both at home and at a health facility 1 . In a recent survey of postnatal care in Aberdeen Maternity hospital in the United Kingdom, up to 87% of women experienced at least one health problem after delivery2 . Barret et al found that in the first three months after delivery up to 83% of the mothers experienced sexual problems. These included dyspareunia, lack of vaginal lubrication, difficulty in achieving orgasm, vaginal loosening, loss of sexual desire and bleeding or irritation after sexual intercourse.3 Similarly, Basson et al found sexual problems such as arousal, orgasm and sexual pain disorders to be highly prevalent especially after delivery.4 Health professionals assume that women will resume normal sexual function after delivery and therefore do not bother to give sexual practice advice. Instead emphasis is put on contraception-related advice. The explanation may lie in the fact that at the six-week checks approximately 60% of women will not have resumed sexual intercourse. Thus the six-week check may be too early to discover chronic problems. 3 In some traditional societies such as the Yoruba in Nigeria, and in some parts of Uganda, women and their husbands are obliged to observe a long time of sexual abstinence after childbirth. One of the main beliefs behind this is that "the man’s semen would find its way into the breast of the mother and contaminate the milk that the child is suckling and hence harm its health". In some societies like among the Yoruba in Nigeria abstinence can be as long as 33 months. This practice has forced women to have long birth intervals and hence reduced fertility levels. On the other hand the amongst the Banyankole society in Uganda, spouses are culturally obliged to resume sexual intercourse shortly after delivery to cerebrate the arrival of the new baby5. This can be as short as 4 days. The implication of this custom on fertility is remarkable. It means that these women have a higher chance of becoming than those who abstain. This would result in high levels of fertility. The women believe that this practice helps in ‘’healing’’ of the perenial tears and the uterus, as it is believed that the semen has some chemical elements with healing properties. Some men also claim that they resume sexual intercourse to congratulate the wife on producing the child. 5 Several studies have explored sexual function after hysterectomy, 6,7 but few studies have looked at sexual intercourse after childbirth. Childbirth brings about a change in sexual relationship such as perineal pain, dyspareunia, decrease in the frequency of sexual intercourse and women’s sexual desire.1,3 Hormonal effects associated with breast-feeding appear to be associated with vaginal dryness and loss of libido, although this finding is not consistent. 8 There is a positive association between levels of dyspareunia and perineal damage (in particular, episiotomy).2,3,9 It is interesting to note that some women prefer elective caesarian section to vaginal delivery since they believe that they will have a smaller chance of dyspaerunia. Obviously this is relevant to is relevant to the debate about the mode of delivery. 2,3 Despite the studies made in popularizing reproductive health and the rights of women in Uganda, there is very little information regarding resumption of sexual practices after child birth. Therefore the general objective of this study was to establish the time taken to resume sexual intercourse, the sexual morbidity associated with resumption and the prevalence of sexual problems encountered by postpartum women attending immunization clinics in Mulago Hospital in Uganda. MATERIALS AND METHODS Design: The study was a cross sectional descriptive study Participants
Women who had brought their babies for vaccination in Mulago Hospital immunization clinics. Setting: Mulago Hospital Child immunization clinics. Sample size calculation
The sample of 216 was estimated using a formula by Kish and Leisie15. We assumed the expected prevalence of sexual dysfunction to be 83% as found in the UK Study3 with a of precision mean 5% at 95% confidence. Inclusion criteria
Sampling procedure and data collection
All the women who had brought their babies for immunization and met the inclusion criteria were recruited. Eligible mothers were consecutively recruited until the sample size of 216 was achieved. One of us (E.O) interviewed the respondents using partially coded questionnaires with both closed and open-ended questions. Variables
Sociodemographic characteristics, time to resumption of sexual intercourse, problems encountered and the health seeking behaviour, were recorded. The data collected was coded and fed into a computer using EPI INFO 6.4 statistical package, cleaned and analyzed with assistance of a statistician. Tests of significance were done using the chi squared test and presented using odds ratio with 95% confidence interval. Ethical considerations
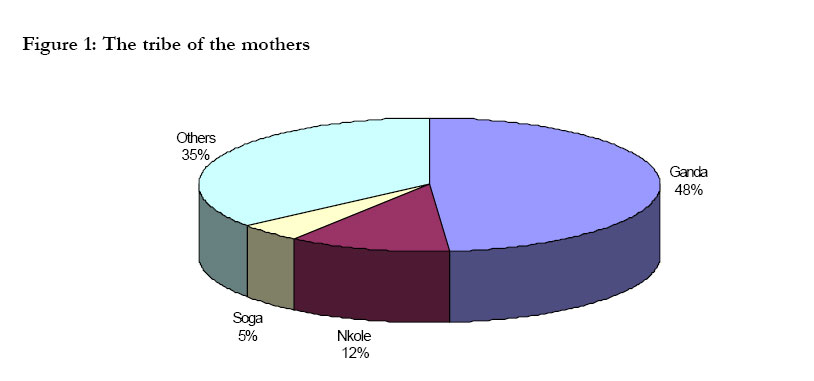
Permission was obtained from the Makerere University Faculty of Medicine research committee, the Mulago Hospital research committee and the National Council of Science and Technology. Informed consent was obtained from the mothers before interviews were conducted. Use of numbers ensured confidentiality and no names appeared anywhere on the questionnaires. RESULTS Socio demographic characteristics of the mothers The majority of the mothers(62.5%) were in the age group 20-29 years.The youngest mother was 17 years while the oldest was 45 years with the mean age of 25 years (SD= 6.02). The minimum age of 17 years corresponded to the early age at first pregnancy and childbirth in our society. The majority of mothers were Baganda (48.0%) and the rest of the tribes in Uganda were represented as shown in figure 1. The literacy rate of the mothers was high(94.9%) which compares with that of Kampala of 88.4%(Uganda National population census 1991) Most respondents were married(76.5%), the rest were single (13.8%),cohabiting or divorced(5.7%). Reproductive characteristics of women following delivery. Of those who resumed menstrual periods the earliest time reported for return of menstruation was 2 weeks and the latest time was 24 weeks with mean time of resumption of 9.79 weeks. By 6weeks 39% of women had resumed menstrual periods. Most mothers delivered vaginally (80.6%) and 39.4% had an episiotomy done or vaginal laceration. Most episiotomies(87.2%) healed well, though 12.8% became infected. Sexual practices among women in the postpartum period.
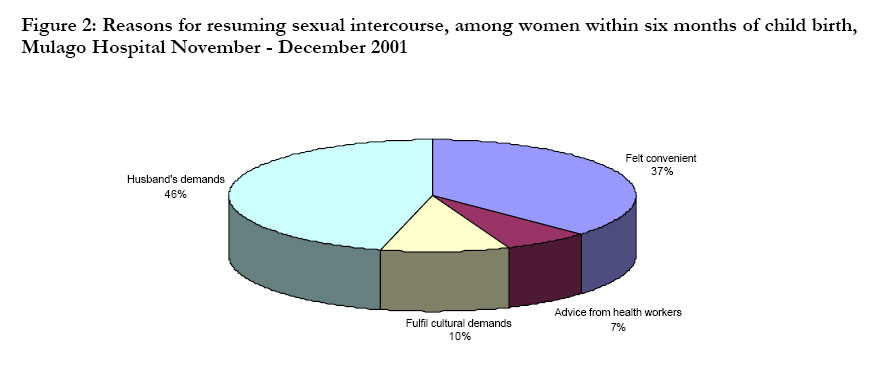
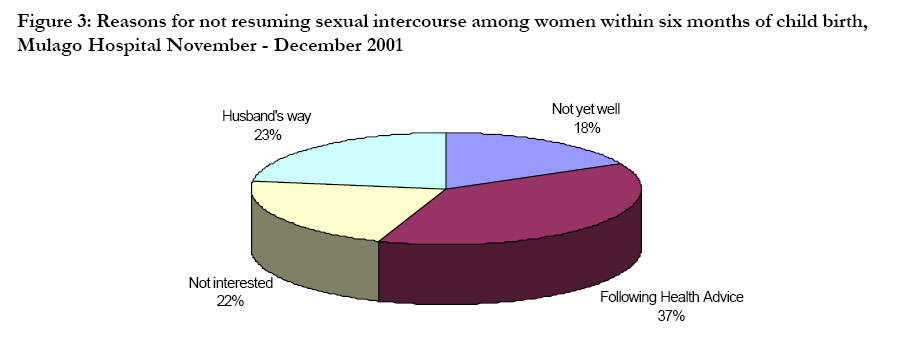
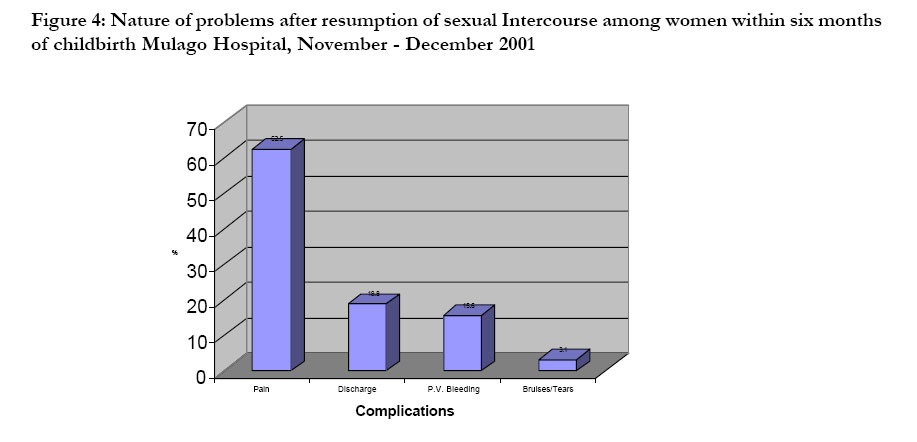
One hundred and forty four of the women(66.4%) had resumed sexual intercourse. Half of these(49.3%) had done so during the puerperium. The earliest time was within the first week and the latest time was in the 24th week with mean time for resumption of 7.87 + 4.9 weeks. Of the women who resumed sexual intercourse within the pueperium 8.5% had done so within the first week. The advice to mothers by the health workers on discharge after childbirth varied, some workers advised mothers to resume sexual intercourse within 6 weeks while others said after six weeks.. The reasons that were given for the resumption of sexual intercourse are shown in figure 2. These included husbands’ demands, advise from health workers, others felt it was just convenient as long as they were feeling well even in the puerperium or to fulfil cultural demands. The reasons that were given for not resuming sexual intercourse are shown in figure 3. Twenty six mothers had not resumed sexual intercourse because they were not told when it was safe to resume sexual relations. Thirty-two women (22.2%) experienced significant levels of morbidity and these were vaginal bleeding, dyspaerunia, tears or bruises and vaginal discharge. These are shown in figure 4. Factors associated with resumption of sex among the mothers within the puerperium
Some mothers resumed sexual intercourse because they were fulfilling cultural demands, but this was not significant. Though the number of respondents were few, the mothers from western Uganda (Banyankole, Bakiga, Batoro, etc) were more likely to resume sexual intercourse within the early days of puerperium. The education level of the mothers perineal or genital damage at the time of delivery, and the mode of delivery were associated with early resumption of before 6weeks.This is shown in table 1. Table 1: Factors associated with resumption of sexual intercourse among women within six weeks of childbirth in Mulago Hospital November – December 2001
Health seeking behaviour of women when having problems after resumption of sex. Of the 32 women with problems only 19 sought for help. The mean age of mothers who sought help was 28.0 years, and those who did not seek help was 21.0 years. The difference in the age was statistically significant;( P=0.016486). The other factors viz. tribe, education level, marital status and parity against the health seeking behaviour are shown in table2. Table 2: Health seeking behaviour of the mothers
Mean age of those who sought treatment 29 years (SD + 7.44) range 20 – 45 yrs Mean age of those who did not seek treatment 23(SD6.71) range 17 – 42 yrs T- test t = 2.540, p = 0.0156.
DISCUSSION
Sexual health of women is not well addressed since sexual issues are considered to be private issues. Sexual morbidity increases significantly after childbirth. When sexual questions are asked routinely in medical practice rather than waiting for the patient to broach the subject, twice as many problems are reported.10 In this study half of the mothers (49.3%) who resumed sex did so during the pueperium. The mean time for resumption of sexual intercourse was 7.87+ 4.9 weeks. This is shorter than the one reported in Nigeria of 16.5 weeks.11 The difference could be accounted for by cultural difference although in this study culture was found not to affect resumption of sexual activity. Women cited many reasons as to why they resumed sexual intercourse early and especially in puerperium. The demand by husbands was an important factor because 46% of mothers who resumed early reported that their husbands demanded to have sex. Similarly, culture is an important factor since 10.0% of women who resumed sexual relations did so because they were fulfilling cultural demands. For instance, in some cultures it was stated that a woman was expected to resume sexual intercourse within the first week after delivery‘’so as to help in the healing of the wounds’’ and ‘’to bring good health to the baby’’. Burton et al also reported this in their survey on Ankole women.5 Other women resumed sexual intercourse early because ‘’they were entering a new house’’ or some mothers thought that ‘’as long as they were feeling well’’ they were justified to resume sexual intercourse even in the pueperium. In our study, 22.2% of mothers reported a high morbidity. This was similar to that reported by Brown and Lumley 10 of 26.3% among Australian women and Walraven et al12 among Gambian women reported 27%. However, Barrett et al reported a higher figure of 83% at the first 3 months declining to 64% at 6 months of childbirth.13 Their figure was higher because they included other qualities of sexual responses like the desire, arousal and the problems associated with orgasm following childbirth. These problems included vaginal bleeding and discharge, bruises or tears, and dyspaerunia. These have been reported in other studies as well.3,10, 11 Other than causing physical injuries to the mothers such as bruises, bleeding and pain when sexual intercourse is resumed during pueperium, chances of transmission of diseases including HIV are high when healing of the genital mucosa is incomplete. Half of the mothers with sexual problems sought assistance but they felt shy to talk about these problems. The majority went to less qualified personnel for advice and treatment. The rest were too shy to seek treatment and either administered their own treatment or they said the problem was over on the same day. CONCLUSION
Most women resumed sexual intercourse within six months of delivery and had high morbidity. This indicates that there is need to develop educational programmes on sexual practices after child birth and pass the information to women and their spouses. ACKNOWLEDGEMENT
We would like to thank Mr. Gideon Kikampikaho, the Deputy Director of Mulago hospital for giving us permission to publish the work. We acknowledge with thanks, Prof. Mirembe for the support and advice while conducting this study. Lastly but not least the in-charge of the Immunisation Clinics and Maureen Ssekisolo for the secretarial work. REFERENCES
From African Health Sciences a year ago.
Safe sex advice is good. Background: Young people in Uganda are advised by the Ministry of Health and other authorities to abstain from sex in order to avoid the human immunodeficiency virus (HIV), other sexually transmitted diseases (STD) and early pregnancies. If they cannot abstain they should use condoms and they should stay faithful to their partner. Copyright © 2003 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs03021t2.jpg] [hs03021t1.jpg] [hs03021f3.jpg] [hs03021f2.jpg] [hs03021f1.jpg] [hs03021f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}