 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences Vol.4, No. 1, April 2004, pp. 3-8 ORIGINAL ARTICLES Vitamin A deficiency among Moroccan women and children Nasri I,1* El Bouhali B, 1 Aguenaou H, 2 Mokhtar N.2 1 Hassan II University. Faculty of Sciences and Techniques. Laboratory of Pharmacology and Physiology. Mohammedia, Morocco. Code Number: hs04002 ABSTRACT: Background: Vitamin A deficiency (VAD), attributable to an inadequate food intake, constitutes a problem in developing
countries. The determination of plasma vitamin A (VA) is a reliable method for assessing VA status of the population. In this
context, high performance liquid chromatography (HPLC) has become the method of choice for VA analysis. INTRODUCTION Vitamin A (VA) and its metabolites intervene in vision, growth, reproduction and the immune system. The discovery of nuclear receptors for retinoic acid enabled a better comprehension of the molecular mechanisms involved in retinoids action1, 2 . Several metabolic and genetic pathways have been described for the interaction of retinoids with nuclear receptors. The most prominent clinical symptoms of vitamin A deficiency (VAD) are eye lesions. The extreme consequences of VAD are irreversible blindness and often death. When the plasma VA (retinol) concentration is less than 0.70μmol/l, the vitamin A status is deficient. Vitamin A deficiency is essentially attributed to inadequate dietary intake. The episodic consumption of food sources of preformed VA such as dairy products, liver, eggs and cereal rich alimentation characterize the most affected countries. In developing countries, blindness, measles and severe diarrhoea are related to VAD3, 4 . The World Health Organization (WHO) estimated that 250 million children mainly in the developing countries are affected by VAD5 . VAD is now recognized to increase childhood and maternal mortality. About 800 000 deaths of children and women in reproductive age are attributable to VAD6, 7 . When maternal VA status is low, breastfed infants are likely to become deficient8 . The evaluation of VA intake of the population by food frequency questionnaires is practical and quick, but it is still not precise due to variability of consumption. The percentage of the population, who consume less than the recommended dietary allowance is higher than that identified as deficient by biochemical or clinical examination9 . The biochemical determination of plasma VA is a reliable method. This biochemical indicator correlates well with hepatic depletion in VA10 . Since the beginning of VA estimation by colorimetry, which was improved and adapted to small samples11 , considerable analytic progress has been achieved. high performance liquid chromatography (HPLC) has become the method of choice for the separation and quantification of retinoids 12, 13 . Similar protocols have been used for analysis of several substances, like vitamin E and the carotenoids14 . An escalation in the search for the lower limit of detection is also noted15 . In this paper, we describe the vitamin A deficiency profile of Moroccan children and women, obtained by the specific HPLC analysis of plasma retinol. MATERIALS and METHODS Extraction of vitamin A The health ministry teams collected and centrifuged the blood from the population in the same day to get plasma. The manipulations were done in a laboratory equipped with dim yellow light. A 200 µl aliquot of plasma was submitted to extraction with 1 ml of hexane containing the BHT as antioxidant after deproteinisation with ethanol containing retinol acetate as the internal standard. The internal standard was used to assess losses during extraction procedures. The organic phase was dried under nitrogen at 40 °C. The residue was dissolved in 150 µl of methanol. A 20 µl volume was automatically injected into the HPLC system. The samples were analyzed in duplicate. The sampling of Moroccan children (aged 6 months to 6 years) was stratified into three levels. The first consisted of children from two chains of mountains: the Rif and the Atlas. The second included those from the plains and the third from the rest of the country. The sample size was 1453 children. The sampling of women (aged 15 to 49 years) was chosen from two representative plains of agricultural population of Morocco. The Gharb area is located in the northwest of the country while, Doukkala is in the west center on the Atlantic coast. Both regions were represented by 494 and 510 women respectively. The results were analyzed by Epi Info software. The difference between the means of VA were compared using ANOVA, while categorical variables were compared using the chi-square test. High Performance Liquid Chromatography
The chromatographic system consisted of the following Thermo-Spectra-Physics equipment: a TSP-P100 pump related to an automated sampler injector TSP-P1000. Peak responses were measured by a variable wavelength detector TSP-UV150 operating at 325 nm with an output to a chromatographic data handling system. The VA was separated from the other constituents in analytical Nucleosil column, C-18 (5 µm, dimension: 240 mm x 4.7 mm). Some modifications were introduced comparatively with the usual method12, 13. The mobile phase was composed only of methanol and was recycled by discontinuous fractions of one liter. Each fraction was exposed to direct sunlight for one hour and then filtered and degassed using ultrasonic agitation. It was then directly reused as mobile phase. The flow-rate was fixed to 1.4 ml/min. The vitamin A assessment technique was controlled by the Swiss Institute of Vitamins (SIV, University of Lausanne). Two areas Errachidia and Beni-Mellal provided 60 identical samples (in quadruplicate). The samples were separated in two groups of 60 samples (two samples per children). Each group was analyzed simultaneously in the LAN and in the SIV (in duplicate). After the end of the analysis, the LAN communicated the results to the SIV for comparison. RESULTS
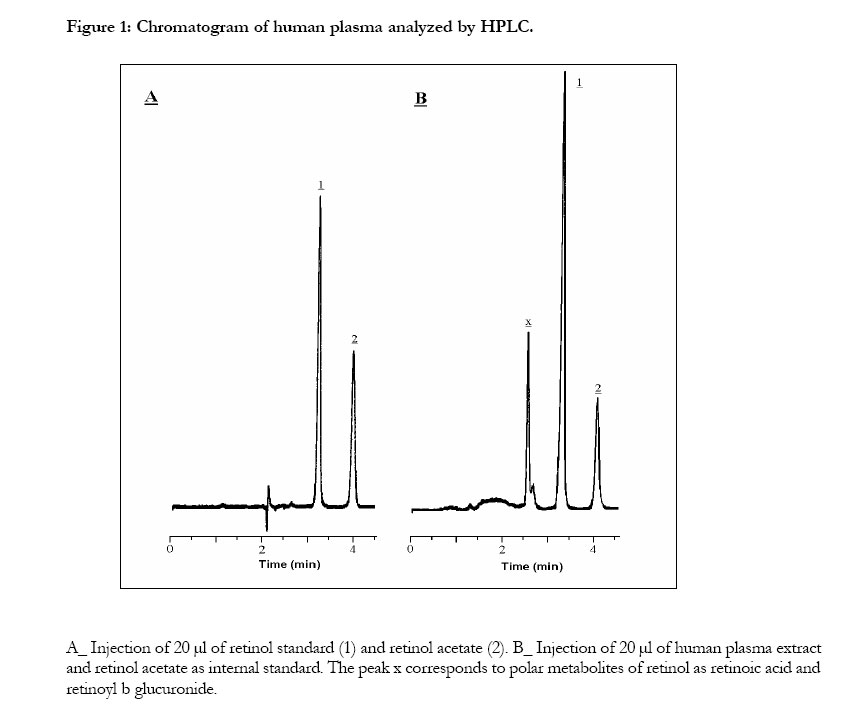
The response of retinol, calculated on increasing concentrations (50 to 600 µg/l), was linear with an equation of regression: y = 1.2939x - 0.0062, r = 0.9991. Figure 1 shows the chromatographic separation obtained from standard solutions and human plasma extract. Each run was less than 6 minutes duration. The retinol had a retention time of 3.25 minutes and 4.05 minutes for the internal standard. All compounds are resolute in relation to the peak of retinol. During the dosage of 2457 human plasma (in duplicate) the column changed only once. The evaluation of the extraction recovery was fulfilled by the calculation of the retinol concentration in the plasma samples with and without addition of different amounts of retinol standard. The recovery rate was of 98.7 ± 3.1 %. The reproducibility was estimated by intra-day repeatability by calculating the coefficient of variation of a concentration of plasma stock. The coefficient of variation calculated was 1.97 %. The detection limit was 12.1 µg/l. The mobile phase was recycled four times without alteration of the chromatographic parameters or of the base line. There was no significant difference between the results obtained by the LAN and the SIV (table 1). The cases of VAD identified on a sample of 60 were 18 for the LAN and 17 for the SIV. The difference be tween both prevalences of VAD (30 % and 28.3 %) was not significant (Khi2=0.04, p=0.840).
Table1: Comparison of the plasma VA assessed by High Performance Liquid Chromatography in the Laboratory of Alimentation and Nutrition (LAN) and in the Swiss Institute of Vitamin (SIV).
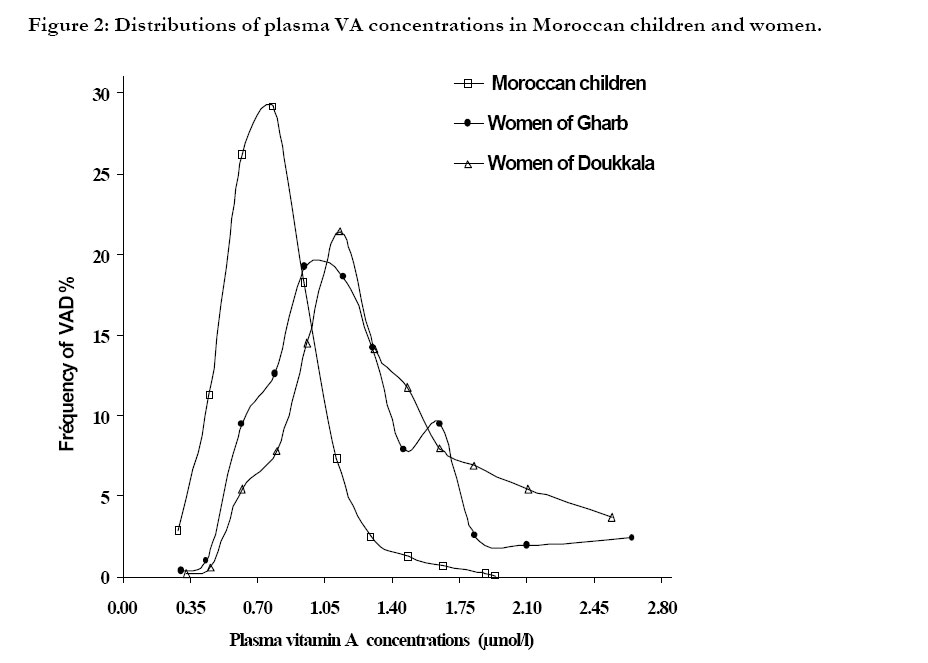
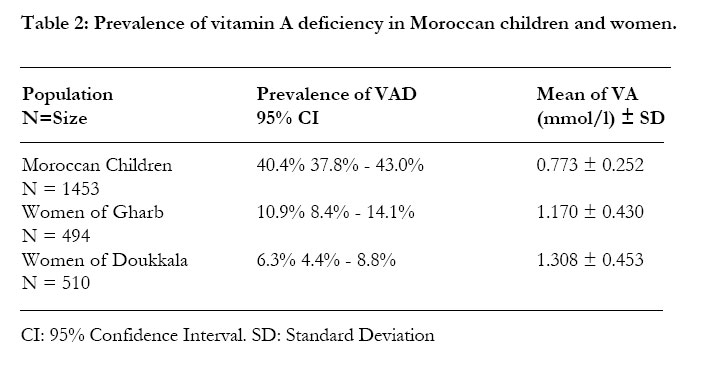
The VA distributions for children and women are represented in the figure 2. The distribution in children’s VA was significantly (p<0.01) moved toward the weak concentrations. The mean concentration of plasma VA of children was 0.773 μmol/l against 1.17 μmol/l of Gharb women and 1.308 μmol/ l for Doukkala women (p<0.01). In all cases, no distribution shows the existence of a class having a mean superior to 3.49μmol/l indicating an excellent dietary intake. The highest prevalence of VAD was reported in the children with 40.4 %. The prevalence of VAD was lowest in the women with 10.9 % for the Gharb and 6.3 % for the Doukkala areas (table 2). The VAD women of the two regions was of a similar magnitude whereas the prevalence of the VAD was considerably more elevated in children. (X2 = 143.5, p<0.01 and X2 = 202.9, p<0.01). DISCUSSION
The choice of mobile phase consisting of only one solvent, methanol, makes the recycling easy. Continuous recycling of the mobile phase contributes to lowering of the cost of the dosage of VA by HPLC. However, it generates water coming from the injected plasma. The enrichment by water increases the retention time of retinol and internal standard16. The discontinuous recycling of the mobile phase has eliminated this handicap. In this way, one liter of methanol was recycled four times, according to the previous method, and then the pump was supplied with fresh mobile phase. The absence of water in the mobile phase gives a low detection limit. This has permitted, especially on samples obtained from children, to adapt the HPLC analysis for volumes of 100 µl. We proceeded to do the VA assessment in 133 samples where it was impossible to extract 200 µl of plasma. The method of analysis has been simplified to take into consideration only the retinol, which is a biochemical indicator admitted by the WHO to determine the VA status of a population. In countries where basic needs are not satisfied, the costly and sophisticated analysis with a high technical profile remains inadequate17. VA deficiency in Morocco is a public health problem. This deficiency is severe among children and moderate among women. Although the prevalence of VAD is low among women, VA distribution remains close to the low concentrations. In comparison with developed countries, this study shows that VA levels in the study population is low. Information from large epidemiological studies shows that the range of 0.7-1.05 µmol/l for plasma retinol may signal inadequate VA intake for some individuals, particularly for post adolescence age groups18. Considering this range we note that 31.8 % of women of Gharb and 28.6 % of Doukkala regions were at risk of developing a VAD. Very often pregnant women in developing countries are vitamin A deficient and no modification occurs in their status during breastfeeding. During the first months of breast-feeding, new borns depend on their mothers to build and maintain a stock in VA19. In Morocco, a country in demographic transition, the infantile mortality remains 45.5 ‰ in urban areas and 90 ‰ in rural areas. The average number of children per women is 3.69. A strong link exists between the nutritional status of the mother and the child. A deficient mother in VA will probably see her children become deficient in VA. Therefore it is not surprising that the prevalence of VAD in children is higher than VAD in women. CONCLUSION
The use of HPLC analysis of VA, for the first time in Morocco, has demonstrated that vitamin A deficiency, is a public health problem. The findings of this study indicate that the national prevalence of VAD in children was 40.4 % and ranged from 10.9 % in Gharb to the 6.3 % in Doukkala for the women. The mean plasma VA concentration of all children (n = 1453) was 0.773µmo/l. against 1.17µmol/l for women living in Gharb (n = 494) and 1.308µmol/l for Doukkala women (n = 510). In all cases, means of plasma VA are low. This observation was confirmed by the absence of fraction indicating an excellent dietary intake for VA (mean plasma VA > 3.49µmol/l). The collaboration between the universities and the ministry of health permitted the installation in Morocco of the VA analysis by HPLC. This tool will be useful in the evaluation of intervention programs against vitamin A deficiency and in future epidemiological studies. ACKNOWLEDGMENTS
REFERENCES
We thank Dr. M Bui ( Swiss Institute of Vitamins, Lausanne University) for her collaboration and also all teams of the ministry of health of Morocco for their logistic support.
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04002f2.jpg] [hs04002f1.jpg] [hs04002t1.jpg] [hs04002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}