 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences Vol.4, No. 1, April 2004, pp. 31-39 Health Providers’ Counselling of Caregivers in the Integrated Management of Childhood Illness (IMCI) Programme in Uganda Charles A.S. Karamagi1,2, Rosalind G.N. Lubanga3, Sarah Kiguli2, Paul J. Ekwaru1,2, Kristian Heggenhougen4 1 Makerere University, Faculty of Medicine, Clinical Epidemiology Unit Code Number: hs04006 ABSTRACT Background: IMCI was launched in Uganda in June 1995 and has so far been implemented in most districts. However, reports indicate that counselling is poorly performed and that health providers find IMCI counselling the most difficult component to implement. Keywords: Child, preschool; infant; health-provider; caregiver; counselling; IMCI-counselling; Uganda INTRODUCTION About 12 million deaths occur annually in under-5 year olds in developing countries. Seventy percent of these deaths are due to the common childhood illnesses (diarrhoea, pneumonia, measles, malaria, malnutrition) and often a combination of these conditions1,2 . The strategy of IntegratedManagement of Childhood Illness (IMCI) was developed by WHO and UNICEF and aims at reducing child mortality and morbidity in developing countries. It combines improved management of common childhood illness with proper nutrition and immunization 1,3. Studies have shown that the guidelines for the Integrated Management of Childhood Illness (IMCI) can lead to appropriate management of sick children by health workers in first-level health facilities4-11 . IMCI was launched in Uganda in June 1995 and has so far been implemented in most districts. Mukono District was the pioneer in IMCI implementation and about 50% of its health providers have been trained in IMCI case management12 . However, quarterly and bi-annualMinistry of Health reports on IMCI implementation indicate that health providers find IMCI counselling the most difficult component to implement12,13. Similar findings have been reported elsewhere 2,3,9- 11,14 . Counselling is a key component of the guidelines for IMCI. The aim of counselling is to put the mother at ease; build her self esteem and confidence; offer accurate information; and impart skills so as to empower her to take the decisions that improve the situation for herself, her baby and her family1,3,15-19. Among the expected outcomes of counselling are changes in caregiver knowledge, attitudes, skills and behaviour with regard to feeding, fluid administration, medication, immunization and follow up care for children under five years2,3,10. Case management in IMCI generally follows the principles of counselling. However, IMCI counselling departs from other forms of counselling mainly in the use of the highly structured algorithm that standardizes and simplifies the case management of the IMCI target conditions, and the mothers’ card that simplifies counselling on feeding. Trained health workers are able to use the algorithm and also provide adequate counselling14. Despite the advantage of using the algorithm, combining it with an un-structured process such as counselling on feeding is potentially challenging because of differences in communication techniques. In one study, although health workers usually communicated appropriate advice to the mothers and learned to check the mothers’ understanding of the advice, they failed to adequately solve problems in the majority of cases9. One difficulty with assessing IMCI counselling is the lack of a uniform definition. IMCI counselling is regarded by IMCI-trained health providers as the counselling that the health provider gives the caregiver regarding the feeding of the child. This view is supported by the fact that the module on Counsel the Mother targets feeding, while the other modules in IMCI do not mention counselling. On the other hand, trained counsellors argue that counselling occurs throughout the entire interaction between the health provider and the caregiver, and therefore IMCI counselling is incorporated in all the components of IMCI. A second difficulty with assessing IMCI counselling is the choice of the gold standard against which to gauge performance in IMCI counselling. Previously, IMCI counselling has been studied mostly by comparing health provider performance with that of more senior health providers, for example paediatricians6,8,9,14. However, this approach usually compares IMCI assessment, classification and drug therapy, and often leaves out the counselling on feeding. For the purpose of the study, we defined IMCI counselling as the entire process of interaction between the health provider and caregiver in the context of IMCI. We therefore set out to assess health providers’ counselling of caregivers and to determine factors that facilitate or constrain IMCI counselling in Mukono District. METHODS
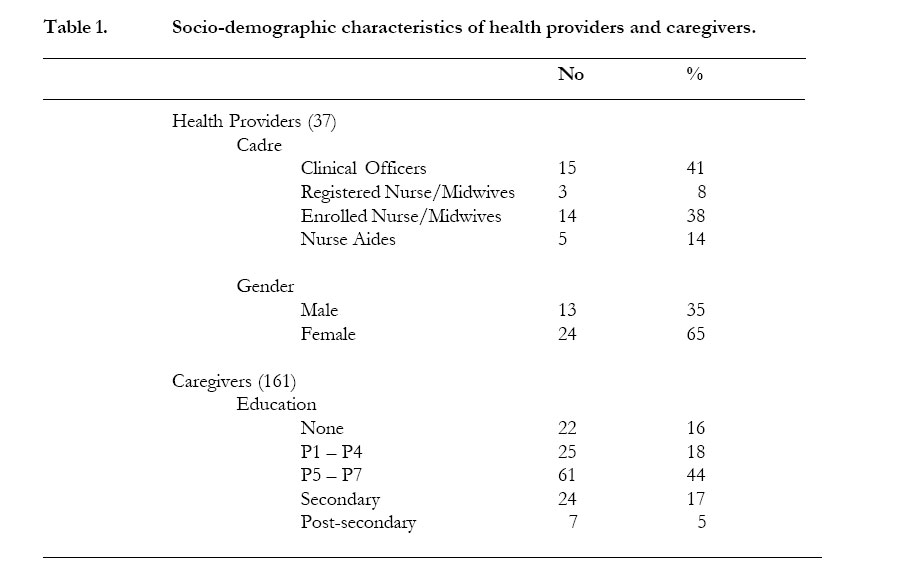
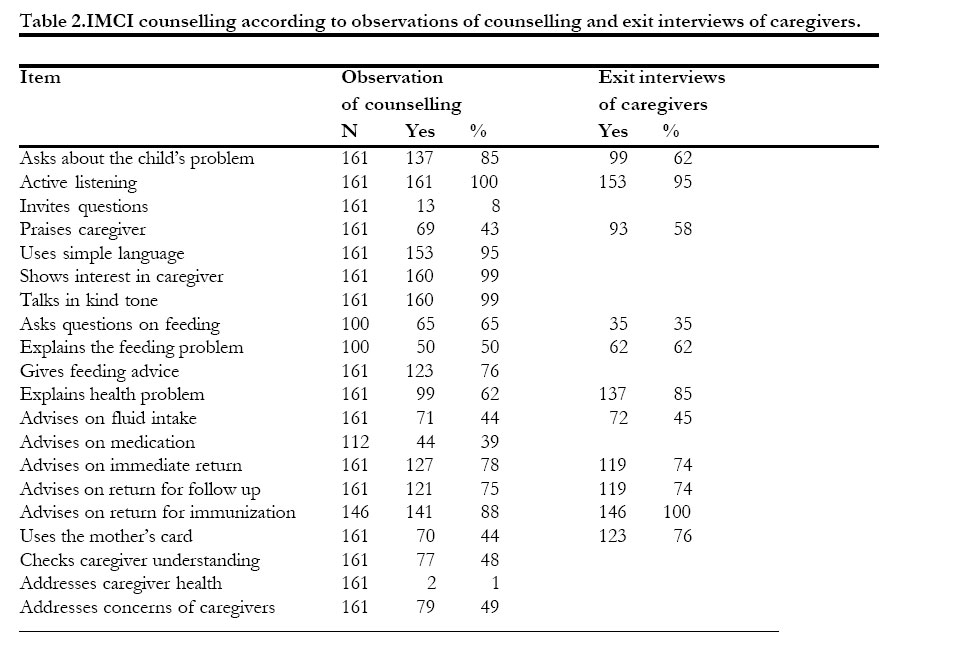
This was a cross-sectional study carried out between February and June 2000 in 19 health facilities in Mukono District. Thirty seven health providers were selected by random sampling stratified for cadre. The sampling frame was all IMCI-trained health workers in Mukono district in both in-patient and outpatient services. Health providers’ counselling was assessed by a medical doctor and a social scientist using a 20-item observation checklist that was developed with the help of IMCI experts and social scientists. In each health facility, the assessment was performed on two consecutive days so as to minimize bias due to the presence of the investigators. Each health provider was observed counselling up to 5 caregivers consecutively. The health providers were interviewed on Day 2 after completion of the observation of counselling. A total of 161 exit interviews of caregivers were conducted after the observation of counselling. In addition, eleven focus group discussions were held with caregivers in communities around randomly selected health units. Each group consisted of 6 to 12 caregivers. The discussions were conducted by a moderator using a schedule and a note-taker recorded the discussions verbatim and also by audiotape. The notes were transcribed and themes identified. Finally, seven supervisors and IMCI trainers were purposively selected and interviewed. Informed consent was obtained from all participants and the study was approved by the Department of Paediatrics and Child Health and the Uganda National Council of Science and Technology. The data was analyzed using Epi-Info Version 6.04 and SPSS 10.0 statistical software. Univariate analysis was performed to show the distribution of the variables and bivariate analysis to determine associations between variables. To control for confounding, standard binary logistic regression was performed. The dependent variables were the IMCI counselling items used in the observation checklist while the independent variables included age, sex, and type of health provider, IMCI experience, supervisory visits, and praise of health provider by supervisors. RESULTS The study involved 37 health providers in 19 health units. A total of 161 counselling sessions out of the planned 370 sessions (44%) were observed due to the low turn up of children at the health facilities. The study included all types of health units but the majority were dispensary maternity units (9/19, 47%). Of the 37 health providers observed, one-third were males and the rest were females, Table 1. The health providers had a mean age of 37 years (SD 9.45). The largest group of the health providers were Clinical Officers. All the caregivers were women and most were married (114/139, 82%). The median parity of the mothers was three children. Most of the mothers were literate with the majority having attained primary education, Table 1. The ages of the children ranged from 2 to 60 months with a mean age of 20 months (SD 15.2). The majority (71%) of the children seen were 2 years and below. The largest single source of livelihood for the child’s family was farming (40%). In the majority of the counselling sessions, the health providers asked the caregivers more than 5 of the 10 questions regarding the child’s problem, Table 2. The median number of questions asked was 8 with a range of 2 to 10 questions. In contrast, a smaller proportion of caregivers reported that the health providers had asked them about the child’s problem. Health providers listened actively to the caregivers by being attentive, encouraging, allowing the caregiver to explain, paraphrasing, and asking relevant questions in all the counselling sessions and this was confirmed by the majority of the caregivers. However, the health providers in only a minority of the sessions invited the caregivers to ask questions and yet the majority of the caregivers reported that they had questions that they would have liked to ask the health provider but did not ask. Health providers praised the caregivers on what they did correctly in almost half the counselling sessions and this was confirmed by the caregivers. In most of the counselling sessions, the health providers used simple language, talked in a kind tone of voice, and showed interest in the caregivers. Health providers asked questions on feeding in 65 of the 100 counselling sessions with feeding problems, although only 35 caregivers reported that they had been asked questions on feeding. In 50 of the same counselling sessions, the health providers explained the feeding problem while 62 out of 100 caregivers reported that health providers had explained to them the feeding problem. Health providers gave advice on feeding in the majority of the counselling sessions. Health providers explained the health problem to the caregivers in the majority of the counselling sessions. Similarly, the majority of the caregivers reported that they had understood the explanation of the health providers regarding the child’s health problem. Health providers advised the caregivers on fluid intake in less than half of the counselling sessions and this was confirmed by the caregivers. In 68 of 112 counselling sessions, health providers did not advise the caregivers on medication when it was prescribed. In the majority of sessions, health providers advised the caregivers to return immediately, return for follow-up, and return for immunization. The majority of caregivers confirmed that health providers had advised them to return immediately, return for follow-up, and return for immunization. Health providers addressed the concerns of the caregivers in about half of the sessions. Health providers used the mother’s card when giving advice to the caregivers in less than half the sessions and this was confirmed by finding that 21% of the caregivers reported that the health providers had ever used the mothers’ cards while counselling. Similarly, health workers infrequently checked the caregivers’ understanding of advice given. In the majority of the counselling sessions, the health providers did not address the caregiver’s health, while in 22 out of 45 sessions, the health providers did not address the concerns of the caregiver. Twelve percent of the children were referred but most health facilities did not have pre-referral drugs for treatment of the children before they were referred. IMCI-trained health workers felt they were able to offer quality services and had stopped wasting drugs. However, they find IMCI time consuming and yet there are many patients that must be attended to. Furthermore it is not possible to check whether mothers do what they are counselled to do. The health workers expressed the need for demonstration facilities for nutrition education and other topics. They were unhappy about frequent shortages of drugs, ORS, and mothers’ cards. They reported that sometimes caregivers do not want to be referred, complain of being delayed, while others come expecting to be treated with certain drugs e.g. injections. This makes the IMCI approach more difficult. They felt that supervisory visits are very beneficial but complained that many planned visits never take place. The use of mothers’ cards was significantly associated with sex of health provider with females more likely to use mothers’ cards than males in the bivariate analysis, Table 3. The use of mothers’ cards was also associated with cadre of health provider with Nurse Aids more likely to use mothers’ cards than other health providers. Older health providers (50-59 years) were more likely to advise caregivers on medication than younger health providers (X2 = 15.64, p = 0.016). Male health providers (X2 = 6.22, p = 0.045) and those aged 30-39 years (X2 = 19.244, p = 0.004) were more likely to explain the feeding problem to the caregivers. Health providers aged 30 or more years were more likely to give feeding advice than younger health providers (X2 = 9.62, p = 0.022). Table 3. Cross tabulation of Sex and Cadre of Health Provider by Use of Mother’s card
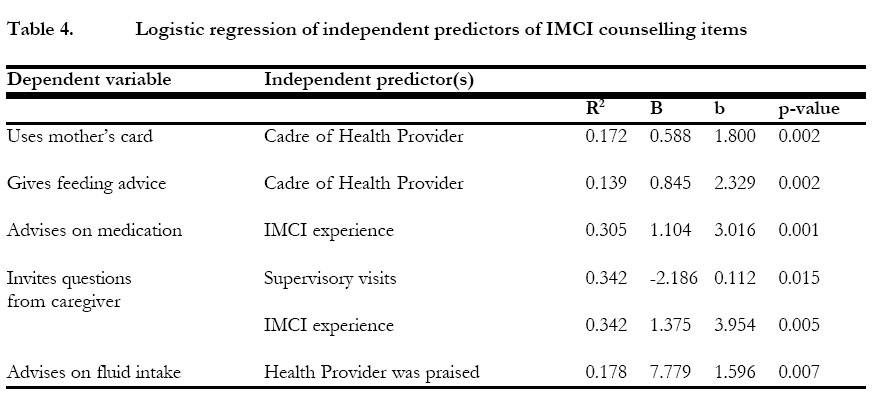
The dependent variables in our logistic regression were the IMCI counselling items used in the observation checklist while the independent variables included age, sex, and type of health provider, IMCI experience, supervisory visits, and praise of health provider by supervisors. Cadre of health provider was associated with the use of mothers’ cards and giving feeding advice, Table 4. IMCI experience independently predicted giving advice on medication and inviting questions from caregiver. The praise of the health provider by the supervisor on the last supervisory visit was associated with giving advice on fluid intake. Supervisory visits to health providers by IMCI supervisors independently predicted invitation of questions from caregiver. DISCUSSION The limitations of the study were the fewer than expected number of sick children in the health units, and the few Registered Nurse/Midwives in the study. The study was conducted during the rainy season. Epidemics of malaria tend to occur at the end of the rainy season and this could partly explain the reason why there were fewer than expected children seen at the health units since the study took place at the beginning of the rainy season. Other factors such as availability of alternative health services or the fee-for-service that was charged as part of the policy of cost-sharing may also have contributed to the low turn up of children in government health facilities. There were few Registered Nurse/Midwives in the study and this could have introduced some error in determining their performance in counselling. By the time the study was conducted, relatively few Registered Nurses/Midwives had been trained in IMCI. Furthermore most of the IMCItrained Registered Nurse/Midwives were deployed in inpatient care in hospitals. The exit interviews of caregivers generally reported higher frequencies of IMCI tasks performed by the health providers than what was observed during counselling, possibly due to social desirability. The health providers assessed the child’s problem quite well with a median of 8 out of 10 questions being asked. Health providers find assessment of the child’s problem relatively easy to perform because it is not very different from the way assessment is carried out in conventional diagnostic work up. Studies have however shown that recognition of common conditions is usually higher than that of uncommon conditions 5,9. Interestingly, a smaller proportion of caregivers than were observed confirmed that the health providers had assessed the child’s problem well. Caregivers may not appreciate the importance of questions directed at problems other than those they perceive to be important. In a study documenting care-seeking practices of mother caretakers in Sri Lanka, although malnutrition was highly prevalent it was not recognised by mother caretakers as an illness 20. Similarly a study in rural Ghana reported that caregivers did not recognize several danger symptoms due to a different local illness classification system 21. Health providers listened to the caregivers, used simple language, talked in a kind tone of voice and showed interest in the caregivers very well. Listening is an essential communication skill but difficult task to perform. Listening is difficult to measure and in this study a number of surrogate behaviour (paraphrasing, encouraging etc) were used to assess listening, possibly introducing some measurement error. It is also possible that listening may have been overestimated because of the Hawthorne effect since the health providers were keenly aware of being observed. Nevertheless the majority of the mothers reported that the health providers had listened to them. Health providers did not invite questions or praise the caregivers for what they did correctly including bringing the child to the health unit. Health providers are often criticized for not allowing caregivers to ask questions. Caregivers who ask questions are often considered to be too knowledgable and attempting to usurp the role of the health provider, and are usually reprimanded by the health provider. It is also uncommon for health providers to praise the caregiver, many arguing that there is nothing to give praise for. Inviting questions from the caregiver and praising her may improve communication between the health provider and the caregiver and possibly increase compliance to medication or behaviour change. Counselling on feeding was not well done with about half the health providers assessing the feeding and explaining the feeding problem. On the contrary, health providers gave general advice on feeding in the majority of the counselling sessions. This study suggests that although health providers usually provide general counselling on feeding, their performance in assessing feeding and giving targeted feeding advice is less than desirable. This may reflect inadequate understanding of nutrition counselling or a reluctance to engage in it given the effort required to do it well. Explaining the health problem to the caregiver was not well done by the health providers. Worse still, giving advice on fluid intake and medication was poorly performed by the health providers. It is not surprising that health providers did not do well in explaining the health problem to the caregivers since the common practice is for the health provider to make the diagnosis and prescribe the medication without any explanation given. What was surprising was the finding that advising on fluid intake and medication was poorly performed considering the effort that has been put on oral rehydration therapy and appropriate medication by the Ministry of Health. It is possible that such advice may not have been given in some instances because dispensing of drugs and fluids was done by someone other than the index health provider who assessed the child. Counselling on return immediately for treatment, return for follow up and immunization were performed quite well. Furthermore the caregivers confirmed that the health providers counselled them on when to return to the health unit. The study suggests that health providers generally do a good job in advising caregivers on when to return to the health unit. Nurse Aids were associated with use of mothers’ cards and giving feeding advice. Nurse Aids have less training than other health providers and are likely to use IMCI job aids including the mothers’ cards more readily than their more trained colleagues. It is also not surprising that Nurse Aids were more likely to give feeding advice since they were using the mothers’ cards that focus on feeding instructions. Health providers who had worked longest in IMCI counselling were more likely to advise caregivers on medication than health providers with less experience. This finding is not surprising since learned skills usually improve with experience. Contrary to expectations, IMCI experience was not similarly associated with other IMCI counselling items covered by the observation checklist because of small cell numbers on logistic regression. Health providers with more IMCI experience and those who had received more supervisory visits were more likely to invite questions from the caregivers than health providers with less experience or supervisory visits. Inviting questions from caregivers encourages two-way communication between the health provider and the caregiver. It is a learned communication skill that is likely to improve with re-enforcement from experience and supervision, a fact that is consistent with the findings of the study. In the study, very few health providers invited questions from caregivers and yet the majority of the caregivers reported that they had questions that they would have liked to ask but did not ask. Unasked and therefore unanswered questions may interfere with the way caregivers receive and act on the advice of the health providers. Since caregivers do not readily ask questions perhaps out of fear of being reprimanded by the health provider or due to cultural constraints, the responsibility of the health providers to invite questions from caregivers assumes even greater significance. Health providers who were praised for their performance during supervisory visits were more likely to advise caregivers on fluid intake than those who were not praised. This finding could be interpreted in two ways since a causal relationship cannot be inferred from the study design. Praise of the health providers provides positive feedback and possibly increases confidence and motivation, and improves skills of health providers. The finding may also suggest that health providers received praise because of their good performance. As for IMCI experience, praise was not associated with other items of IMCI counselling in the observation checklist because of small cell numbers on logistic regression. The infrequent use of mothers’ cards could have been due to unavailability of the mother’s cards in some of the health facilities. However, the cards were available in most health facilities where for the most part they were kept under storage. The reason for not using the cards was not very clear and appeared to be a result of general apathy of health providers in use of IMCI job aids. The mothers’ cards were designed to support communication with mothers. Caregivers who had received mothers’ cards on previous visits said that the cards helped them to follow what they had been advised to do and even to share the advice with neighbours. Contrary to the findings of our study, previous studies had shown that mothers’ cards are highly appreciated by both health workers and caregivers and are used by health workers whether or not they have already been trained in IMCI 3 . During the study, 12 percent of the children were referred because of severe disease. The referral rate was within the range of 7% to 16% reported in published studies in Africa but higher than that reported in a recent observational study at first-level health facilities in Uganda, the United Republic of Tanzania, and Niger, which found that 9.6% of the children required urgent referral to a hospital 22. We observed that most health units did not have prereferral drugs especially quinine and chloramphenicol. Ensuring the availability of prereferral drugs has presented a special challenge to the health services, and in a study from Uganda in which trained health workers were followed up at 4 months, intra-muscular Chloramphenicol was available in 8/22(36%), while intra-muscular Quinine was available in 10/22(45%)3,8. The health of the mothers was an issue that often came up in the survey. Many mothers complained of fevers, gynaecological symptoms or had questions about family planning. What surprised us was that the caregivers would go through the interview with the health provider without mentioning their concerns, and then present their concerns to the survey team during the exit interview. It is possible that the caregivers wanted to take advantage of the doctors in the survey team. In any case the health providers did not inquire about the caregivers’ own health. Group discussions confirmed that caregivers often have health problems of their own but that the health providers do not give them opportunity to inquire about their health problems. This is unfortunate since the caregivers’ health may influence how they receive the IMCI counselling and the care they offer to the children. Some health units had a separate room for counselling caregivers but we did not show any association between availability of a separate room for counselling and quality of counselling. The lack of a separate room may have inhibited some mothers from asking questions relative to their own health. Privacy is a key issue in counselling and therefore a separate room is usually recommended. However, counselling in the presence of other caregivers has the advantage of reaching a greater audience and also reenforcing the knowledge of other caregivers. Time required for case management varied from 8 minutes to 20 minutes with a mean of 15 minutes. Some health providers did not appear to be familiar with the IMCI charts, while others may have been nervous and tried to do everything correctly in our presence. A study in western Uganda showed that consultations took on average 7.2 minutes, longer than usual for several African countries23. In conclusion, the study showed that the performance of health providers was good in nine out of 20 IMCI counselling items but poor in the rest. Cadre of health provider, IMCI experience, number of supervisory visits and praise of health provider were independent predictors of using mothers’ cards, advising on medication, inviting questions from caregivers, and advising on fluid intake respectively. Improvements in IMCI counselling could be achieved through greater emphasis on use of IMCI job aids; strengthening support supervision and providing positive feedback to health providers. The issue of availability of pre-referral drugs should be addressed by ensuring that these drugs are part of the essential drug kit. Finally, health providers should be trained and encouraged to address the health of the caregivers as well. Acknowledgements This study was funded by the Applied Research on Child Health (ARCH) Project Grant No. 004 of the Harvard Institute for International Development (HIID) now at the Center for International Health and Development at Boston University School of Public Health. We are indebted to Dr Jessica Nsungwa-Sabitti and the Ministry of Health for facilitating the data collection; the research assistants without whose hard work these data could not have been accumulated; the health providers, caregivers and children who participated in the study; and Professor Thorkild Tylleskar who reviewed the manuscript. We also acknowledge the support of the International Clinical Epidemiology Network (INCLEN). REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04006t4.jpg] [hs04006t2.jpg] [hs04006t1.jpg] [hs04006t3.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}