|
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences Vol.4, No. 1, April 2004, pp. 58-62 PRACTICE POINTS Treatment of fissure in ano- revisited. Pravid J. Gupta Gupta Nursing Home, D/9 Laxminagar Nagpur-440022, India
Code Number: hs04009 ABSTRACT Introduction: Fissure in ano is a troubling and painful condition that affects a great majority of the population world over.
The nature and anatomy of fissure in ano is quite clear, and much is known about the various predisposing and contributing
factors that lead to initiation and progression of the disease. The preferred method of treating them, one that results in
optimal clinical results and the least pain and inconvenience to the patient, however, has been open to debate. Keywords- Fissure-in-ano, sphincterotomy, recurrence, anal spasm. INTRODUCTION Anal fissure is the most common cause of severe anal pain. It is equally one of the most common reasons of bleeding per anus in infants and young children. The pain of anal ulcer is intolerable and always disproportionate to the severity of the physical lesion. It may be so severe that patients may avoid defecation for days together until it becomes inevitable. This leads to hardening of the stools, which further tear the anoderm during defecation, setting a vicious cycle. The fissures can be classified into 1] Acute or superficial and 2] Chronic fissure in ano. Predisposing Factors: It has been proved that constipation is the primary and sole cause of initiation of a fissure1. Passage of hard stool, irregularity of diet, consumption of spicy and pungent food, faulty bowel habits, and lack of localhygiene can contribute for initiation of the pathology. In females, the ailment is usually triggered during pregnancy and following childbirth. It occurs as a superficial split in the anoderm that may heal by itself or may progress to a chronic fissure. Pathophysiology: The anoderm is more adherent to the underlying tissue in the posterior midline. The sphincter fibers form Y-shaped decussation in the posterior midline that is anchored to the mucosa. Blood supply to the anoderm at the posterior midline is significantly lower .The reduced blood supply to the lesion is indicated by the absence of granulation tissue at the base of the fissure and a very slow growth of the anoderm even when the traditional conservative treatment eases the trauma due to hard faeces. A well-developed idiopathic anal fissure rests directly over the internal sphincter and the circular fibers of this sphincter are visible on the floor of the fissure on naked eye inspection. The internal sphincter undergoes a perpetual state of spasm due to irritation and hypertrophies. Treatment of Superficial fissures: It has long been recognized that superficial fissures can be cured conservatively2. The following methods are usually advocated for such type of simple fissures.
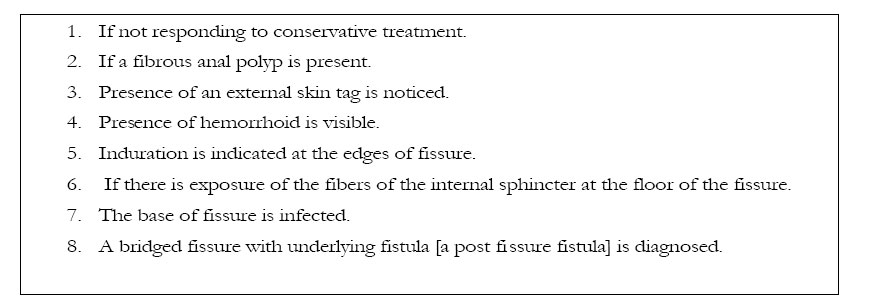
Chronic or complicated fissure in ano: The above mentioned approaches do not prove effective in the chronic variety of fissures in ano. These chronic or complicated fissures are not amicable to the aforesaid simple conservative line of treatment. A definitive therapy is needed to tackle this stubborn malady. The fissure is labeled as chronic or complicated if it fulfils the following criteria6 .
It has been experienced that fissure, complicated by any of the above facts, neither heal spontaneously nor does it respond to conservative therapy7 . MATERIALS AND METHODS: Various therapies advocated for treating these chronic fissures and which are presently in practice have been summed up in the following paragraphs. Such proven therapies may be grouped into nonoperative and operative maneuvers. Non-operative techniques- 1] Injection of Botulin Toxin: Botulin toxin is known to cause paresis of the sphincter and thus 20 Units of type A botulinum toxin [Botox] diluted to 50 U/ml is injected bilaterally to the fissure. The toxin exerts its effects on the acetylcholine releasing parasympathetic peripheral nerve endings as well as the ganglionic nerve endings, thereby leading to flaccid paralysis of the internal sphincter. This causes sphincter paresis for about 3 months, a period which is sufficient for healing of a chronic non-complicated [not associated with sentinel tag, internal hemorrhoids, anal polyps or post fissure fistula] fissure8. It is well tolerated and can be administered on an outpatient basis. The healing rate reported is about 79%. Drawback: The toxicity of the drug, accidental injection in the surrounding tissue amounting to general poisoning, haematoma and infection reported had discouraged regular use of this therapy9 . 2] Oral Nifedipine: Nifedipine is an L-type calcium channel antagonist. L-type calcium channels are the principal calcium channels in the GI smooth muscles. It has been used with variable effects in the management of achalasia cardia. In the treatment of anal fissures, 20 mg of Nifedipine is given twice daily. Nifedipine is found effective in relieving the sphincter spasm10. It is known for achieving increase in the local blood supply by an independent mechanism. This allows faster healing. Drawback: It is, however, supposed to cause reversible internal anal sphincterolysis. Most of these drugs have a short duration of action and need to be administered 2-3 times daily. Similarly, side effects like headache, palpitations, flushing, dizziness, colicky abdominal pain; ankle edema, reduced taste and smell, nausea and dyplopia have been reported 3] Local application of vasodilators: Nitric oxide is an important neurotransmitter mediating internal anal sphincter relaxation. It has been proved that chronic anal fissure is ischemic in origin due to poor blood supply and spasm of internal anal sphincter. Nitric oxide donors such as glyceril trinitrate [GTN] or isosorbid di nitrate are known to cause a chemical sphincterotomy leading to healing of fissure11 . A 2%GTN ointment applied twice to the anoderm for 6 weeks results in a complete healing in 98% of patients12. A few patients do experience mild headache during therapy. In another study, Topical diltiazem ointment was used as an agent for chemical sphincterotomy for chronic anal fissure. The Study claims to offer significant healing rate and reduced incidences of side effects13 . Drawbacks-However, during the course of therapy, strict dietary restrictions to smoothen the stool are necessary. Headache during therapy is a major concern with the incidence as high as 20- 100%. Though the application of GTN has a high healing rate; it also has a high recurrence rate. 4] Direct current probe treatment: This method is tried in patients of chronic anal fissures with associated internal hemorrhoids. A study claimed that when the DC probe [Ultroid, Homeron] was applied to the internal hemorrhoids, the patients were relieved of anal pain and healing occurred in 90% of patients14 . Drawbacks: However, this mode of treatment requires special equipment and the procedure takes a very long time to be performed [about 10minutes for each hemorrhoid]. Moreover, the mechanism of action on the part of fissure is also not understood. A case of complication in the form of perianal abscess and fistula requiring surgery has been reported following DC probe treatment15 . 5] Endoscopic anal dilatation: In this procedure, anal dilatation is performed with a two-valved anoscope under local anesthesia as an office procedure16 . In the study, 93% patients were found symptom free one month after the procedure, and only a few had a recurrence. This procedure is said to be free of discharge or defect of continence either transient or permanent. In another series, a Parks’ retractor or a recto sigmoid balloon has been used for sphincter dilatation. Out of 495 patients treated through this procedure, it is reported that in as many as 87- 88% of the patients, the fissures were healed within 3 months 17 . Drawback: As many references are not available in support of this technique, it will be hazardous to comment on the efficacy or otherwise of this procedure. 6] Chemical cauterization: This is done by using silver nitrate or phenol-in-glycerine. This procedure may be repeated a couple of times until healing occur. It takes about 4 to 8 weeks for complete healing of the fissure. Drawbacks: The toxicity of the drugs, accidental injection in the surrounding tissue amounting to general poisoning, hematoma and infection reported had refrain the surgeons from regularly resorting to this method. Operative techniques 7] Stretching of anal sphincter [Lord’s anal dilatation]: Anal dilation was described by Recamier in 1838. This was one of the most favored and accepted methods of treating the anal fissures 18. The primary cause of attraction for the procedure is its extreme simplicity. Since almost no instruments are needed for this procedure, it could be performed at the primary health centers or inadequately equipped hospitals situated at small townships. Anal dilatation helps in healing of the fissure by reducing the anal canal pressure. If performed with due care by avoiding excessive manipulation, it does not cause any damage to the external anal sphincter as feared. In experienced hands, incontinence of stools or flatus is seldom seen19 . Drawback: However, recent studies have shown that anal dilation has a higher risk of fissure persistence and higher risk of incontinence20 . Although the procedure in itself is curative, in cases with associated pathologies, it has to be supplemented with an additional procedure. 8] Excision of the anal fissure [fissurectomy]: A triangular part of the anoderm is excised along with the fissure itself. This procedure is usually preceded by anal stretch. Drawback: Howsoever, good and reliable this operation is, it leaves behind a large and rather uncomfortable external wound, which takes a long time to heal20 . 9] Fissurectomy with immediate skin grafting: To expedite healing and shorten the convalescence, application of a split thickness graft to the wound is advocated by a section of the proctologists. Drawbacks: The procedure is time consuming, rather a finicky one. It needs a hospital stay of about a week to keep patients bowel held up to avoid possible detachment of the graft. Precisely, for these reasons, the procedure could not get enough acclamation and acceptance. 10] Division of internal anal sphincter: Division of internal sphincter fibers to relieve the sphincter spasm is presently considered the preferred therapy for chronic, recurrent and non-healing fissures21 . Two techniques have been described. A. Open posterior internal sphincterotomy. Posterior sphincterotomy is done by dividing the sphincter fibers through the fissure wound. Drawbacks-The wound is slow to heal and has a tendency to lead to a posterior midline keyhole defect that may cause a persistent seepage or difficulty in continence. B. Lateral subcutaneous internal sphincterotomy. It is one of the most favored procedures. The reasons for this are the simplicity of the procedure, minimal anesthesia requirements, and good results. The lists of complications that can arise due to the procedure are formidable; but with careful and experienced hands these could be effectively handled and the procedure could be made safe and simple. Drawbacks: The most common complications encountered are bleeding needing hospitalization, abscess and fistula formation, incontinence to flatus and feces, and recurrence. Both the procedures can be done either under a local or a general anesthesia depending upon personal preference of the surgeon based on his experience and the attitude of the patient. 11] Combined outpatient surgical and cyrotherapeutical treatment: A lateral anal sphincterotomy, which is done under local anesthesia, is followed by fissure curettage with N protosside cryosound23. This is claimed to be quicker and more effective procedure. Drawback: The additional maneuver is not found to be of any specific advantage and so it has not found many takers. 12] Carbon dioxide laser surgery: It involves laser vaporization of the fissure locally. The internal sphincter can be incised using this laser. In long-standing fissures, some degree of anal stenosis is present. It can be used to give relieving incisions in the three quadrants other than the fissure before the fissure is attended. Drawbacks: The high cost of the laser unit seems to be the major deterrent in its wider acceptance. 13] Lateral subcutaneous internal sphincterotomy and radio frequency surgery: In an attempt to improve on the available options, a fusion of method of sphincterotomy with radiofrequency is described. The procedure has been claimed to be effective in cases where the fissure is associated with pathologies like sentinel tags, hypertrophied anal papillae, fibrous polyps, post fissure fistula or internal hemorrhoids which can be tackled simultaneously while the fissure is being treated24-25 . The radio frequency surgical unit used is Ellman Dual Frequency 4MHz by Ellman International [Hewlett, NY], which incorporates threefold function of cutting, cutting and coagulation or pure coagulation. It is claimed that the edges of the fibrosed fissure can be refashioned with the help of the radio frequency surgery. The entire procedure is quick and is virtually bloodless26 . Drawbacks: Being a new introduction with no controlled or randomized trials available, this treatment modality needs further studies to analyze long-term results. Conclusion: Revisiting the trends of treatment of chronic anal fissures, it can be concluded that conservative treatments with nitroglycerine, botulin toxin, and oral nifedipine are all effective methods that may reduce the need for anesthesia and surgery in many of the patients. These could always be offered to the patients who are not willing for operative procedure. Surgical manipulation should be sought in case of recurrence or failure of conservative treatment. While all the available options are explained to the patient with complete information about the method, cure rates, complications, and reversibility of the disease, the surgeon should analyze the optimum treatment for the particular patient in order to make a good and safe choice and then offer to the patient the result of the best of judgment of his own. REFERENCES:
Copyright © 2004 - Makerere Medical School, Uganda |
| |||||||||