 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
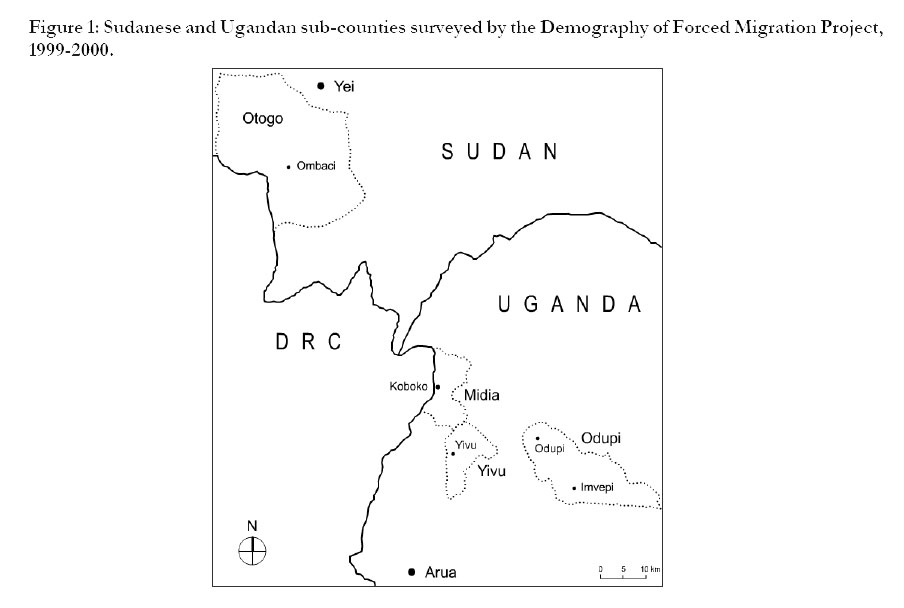
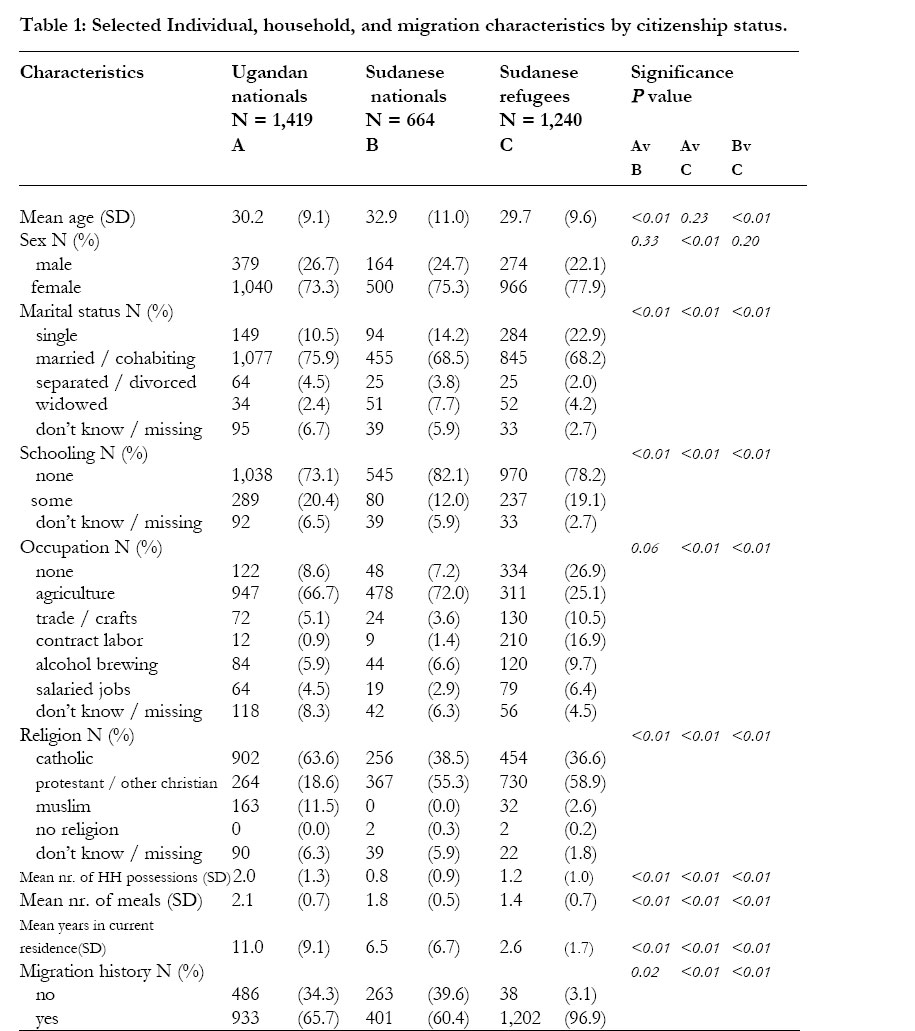
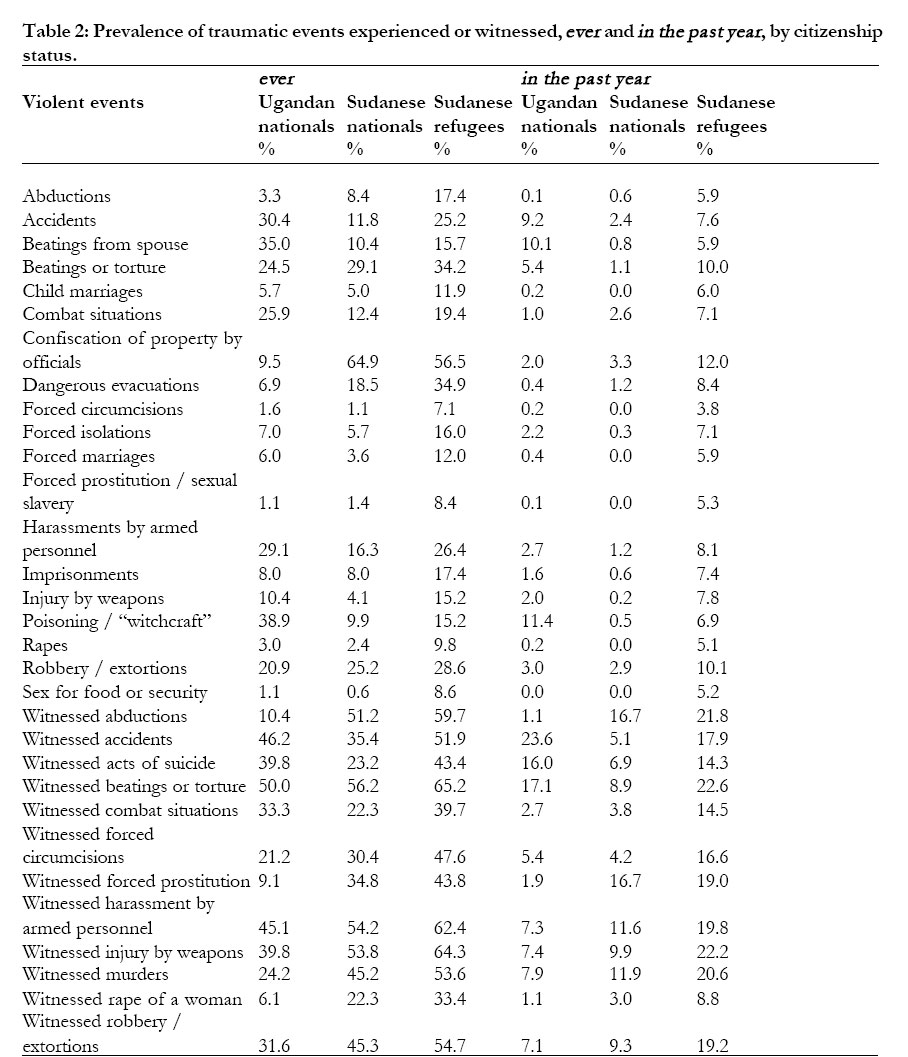
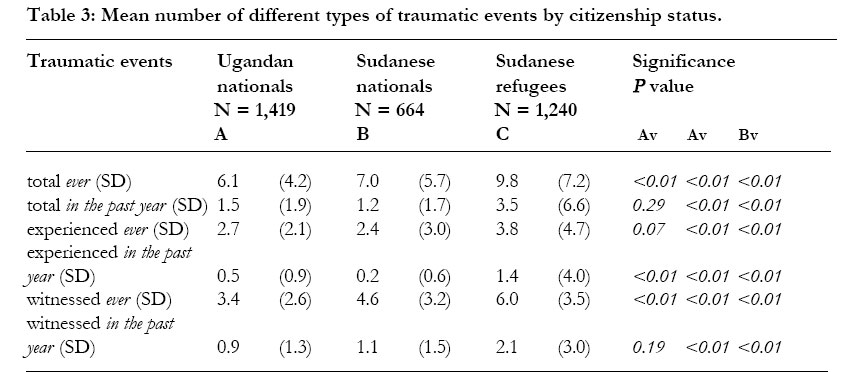
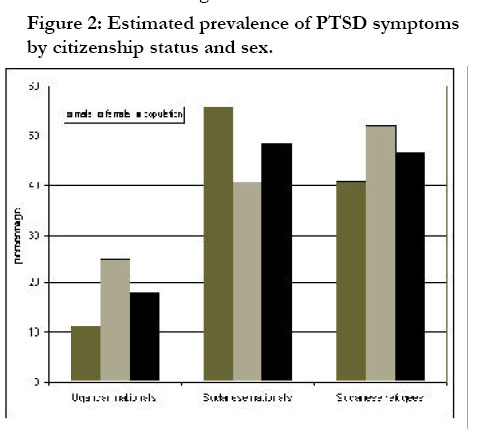
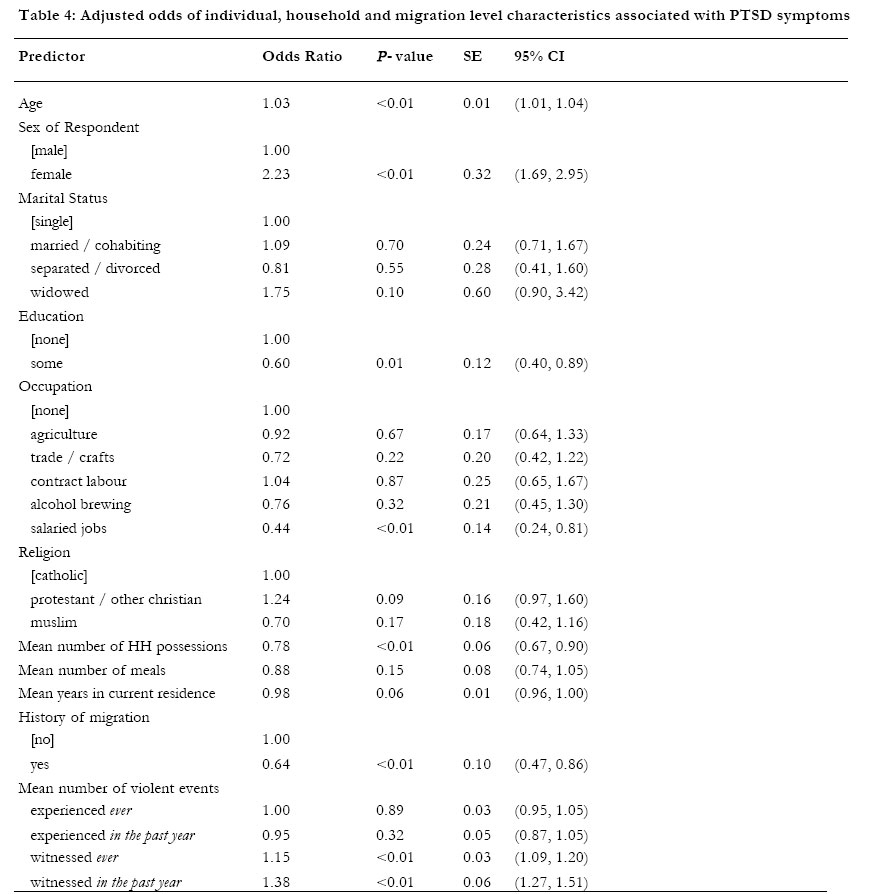
African Health Sciences, Vol. 4, No. 2, August, 2004, pp. 83-93 ORIGINAL ARTICLES Traumatic events and symptoms of post-traumatic stress disorder amongst Sudanese nationals, refugees and Ugandans in the West Nile. Unni Krishnan Karunakara1, Frank Neuner2, Margarete Schauer3, Kavita Singh4, Kenneth Hill5,Thomas Elbert6, Gilbert Burnha7 1. Médecins sans Frontières, PO Box 10014, 1001 EA Amsterdam, The Netherlands, Code Number: hs04016 ABSTRACTObjectives: To compare the incidence of traumatic events and its association with symptoms of post-traumatic stress disorder in three population groups in northern Uganda and southern Sudan. Keywords: forced migration, traumatic events, post-traumatic stress disorder, PTSD, Uganda, Sudan, refugees INTRODUCTIONSteady streams of refugees have crossed the border between the Sudan and Uganda since the mid 1950s, when thousands fled the Sudan to escape the civil war between the Government of Sudan (GoS) and southern rebel forces.12 The Addis Ababa peace agreement of 1972 led to the return of approximately 78,000 refugees from northern Uganda. Five years later, over 163,000 northern Ugandans sought refuge in southern Sudan, fleeing a bitter struggle for power in Uganda.1 3-5 The insecurity that prevailed among Ugandan refugees in southern Sudan has been well documented.6 Ugandan refugees returning to their homes between 1986 and 1989 were accompanied by their Sudanese hosts fleeing an escalation of fighting in the region. Between 1986 and 1994, over 100,000 southern Sudanese refugees crossed the border to Uganda.1 Housed in transit camps and later in settlements close to the border, these refugees were repeatedly attacked by Ugandan rebel groups backed by the GoS.4 7 In 1997, Ugandan rebels based in southern Sudan attacked the Ikafe refugee settlement, looting, raping, mutilating and killing several refugees. This attack prompted several refugees to return home and the relocation of others to the Imvepi refugee settlement. Out of the 175,000 to 200,000 Sudanese that have sought refuge in Uganda, approximately 12,000 are currently settled in Imvepi while another 8,000 opted to self-settle in the border town of Koboko. Populations that experience war and forced migration have a high burden of psychiatric morbidity, in particular, post-traumatic stress disorder (PTSD). PTSD encompasses symptoms of intrusive recollections of the traumatic events, avoidance behaviour, general hyper arousal and reduced functioning, and is associated with the experience or witnessing of life threatening traumatic events.8 9 A number of studies suggest that increasing severity of trauma,10 and the number of traumatic events11 in particular, aggravate a victim’s PTSD symptoms. Sixteen out of 19 studies reviewed by March12 supported a dosage effect. However, a relationship between psycho-pathological symptoms and objective measures of trauma severity is multifaceted and far from clear.13 Prevalence of PTSD ranges between 14 and 37% in community samples of populations affected by war and forced migration,14-17 in comparison to 6 and 8% in communities in the United States.18 A recent study of different convenience samples of Sudanese refugees found prevalence rates of PTSD between 13 and 32%.19 Most modern conflicts and forced migrations occur in resource poor countries and stressors caused by poverty, lack of security, and violence may contribute to the development of PTSD. In addition to stressors associated with life in insecure environments, emotional and cognitive turmoil related to the experience of forced migration as well as the adaptation to new living conditions in countries of asylum or resettlement may lead to the maintenance of PTSD and foster the development of co-morbid depression in refugee populations.20 23 Refugee settlements breed violence and refugees are often victims of violent acts perpetrated by the army, militias, humanitarian workers and by their hosts.24-26 For many women and children, the very act of going to communal latrines27 or collecting firewood28 and water can be extremely dangerous. Very few studies have examined the impact of war and forced migration on the prevalence of PTSD in conflict areas.14-16 Most studies have taken place in a neighbouring country of asylum 29-31 or in a third country of resettlement.20-22 32-36 Researching dynamics of forced migration and war is not only logistically challenging but also can have deep political implications and is complicated by the fact that appropriate tools and methodologies do not yet exist for the study forced migration.37 38 Studies among forced migrants and waraffected populations have so far used instruments that have been validated for other populations.14-17 This study compared the incidence of violent traumatic events and its association with symptoms of PTSD in three population groups (Sudanese nationals living in conflict areas, Sudanese refugees living in and outside refugee settlements, and Ugandan nationals living in politically stable areas) in northern Uganda and southern Sudan using a single-round cross-sectional demographic survey. The survey was approved by the Uganda National Council of Science and Technology, Johns Hopkins University School of Public Health Committee on Human Research and the University of Konstanz Ethical Review Board. METHODS Survey Population A demographic survey of residents of the sub-counties of Odupi, Midia and Yivu in northern Uganda and of Otogo in southern Sudan was conducted between September 1, 1999 and March 4, 2000. Residents of these sub-counties had not only experienced war and forced migration but were also ethnically and culturally similar, thereby reducing the possibility of potential political, cultural or societal biases. A multi-stage sampling technique was used to select sites for the survey. The sub-counties were selected purposively based on the absence or presence of the refugees. The Imvepi Refugee Settlement was situated in Odupi, while Midia had substantial numbers of ‘selfsettled’ refugees co-existing with their Ugandan hosts. Yivu, with no refugees, served as a comparison group in the study of the effect of post migration residential arrangements on the lives of refugees as well as their hosts. The relatively stable security situation that existed at the time of the survey, allowed access to Otogo, home to many of the refugees surveyed in Uganda. Villages — the primary sampling unit — to be surveyed in the subcounties were selected randomly. Households — the ultimate sampling unit — were selected systematically. Sample size calculation was based on available under-5 mortality figures so as to calculate the most conservative figure possible. Calculations were made for comparing populations with a design effect factor to account for deviations from a simple random design. In total, 3,371 individuals from 1,842 households were interviewed providing sufficient power for statistical analyses. Analysis was restricted to 3,323 individuals for whom complete data was available. Survey Questionnaire A demographic questionnaire with a section on household composition and characteristics (Part A with 60 questions) and another section (Part B with 257 questions) on individual characteristics, reproductive and child health as well as migration and security histories was developed. Key informant interviews provided an understanding of local perceptions of fertility, mortality and helped develop a checklist of trauma categories. An event calendar was created to support the respondent’s assessment of age. The questionnaire was written in English and translated to Lugbara for the Ugandans and to Arabic (colloquial Juba version) for the Sudanese. This was achieved by using Back-Translation (Double Translation) and Decentering (Symmetrical) techniques.39 The goal was to achieve a conceptually and semantically equivalent translation while maintaining ‘colloquialness’.40-42 Symptoms of PTSD were assessed using an internationally recognized instrument — Post-traumatic Stress Diagnostic Scale (PDS)43 — modified for rating through trained interviewers. PDS is widely used in North America and Europe as a screening instrument for the diagnoses and severity of PTSD on the basis of the DSMIV Criteria. Traumatic events were assessed using a checklist consisting of possible war and non-war related traumatic events and included 19 experienced events and 12 witnessed events (see table 2) that were coded as number of events experienced, ever (i.e., lifetime experience) or in the past year. As most respondents did not have regular incomes, socio-economic status was determined by their occupation as well as household possessions such as blankets, water containers, cooking pots and agricultural tools. The number of meals on the day prior to the survey was chosen as indicator of the respondent’s access to food. Interviews Twenty-four interviewers, two supervisors and a project assistant were hired locally from the Ugandan national and Sudanese refugee communities. Project researchers and a consultant trained the team in quantitative research methodology and interviewing techniques. A workshop on sexual and gender-based-violence was conducted before the survey to increase awareness and sensitivity of the teamtowards respondents. All interviews were conducted in Lugbara and Arabic within a six-month period. A team of Ugandan interviewers surveyed the Ugandan population in Lugbara while another team of Sudanese interviewers surveyed the Sudanese national and refugee populations in Juba Arabic. All female respondents were interviewed by female interviewers. Male respondents in the same household were interviewed simultaneously by male interviewers. Efforts were made to separate the men from women so that sensitive questions could be answered in a private manner. Each interview lasted approximately two hours. One eligible respondent, usually the head of the household, responded to the household questionnaire. Individual questionnaires were administered to all eligible females and randomly selected eligible males in a household. Signed informed consent was obtained and respondents received no monetary reward for taking part in the survey. Demographic characteristics of 3,323 individuals, categorized by place of residence and citizenship status were analysed. The average age of respondents was 30.5 years. The majority of respondents were female (75%) and had never attended school (77%). More than one third of all respondents (37%) identified themselves as refugees in Uganda at the time of the survey and 76% of the respondents reported at least one experience of forced migration in their life. Individual, household, and migration characteristics of the three population groups — Ugandan nationals, Sudanese nationals and Sudanese refugees — are presented in table 1. The 3 groups differed substantially in their socio-economic characteristics. Ugandan nationals were more likely to be married or co-habiting (76%) than Sudanese nationals or refugees (68%). Majority of the Ugandan (67%) and Sudanese (72%) nationals were engaged in subsistence farming while only one out of every four Sudanese refugee (25%) was a farmer. Many refugees were unemployed (27%) or were temporary contract labourers (17%). As expected, Ugandan nationals were better off than the Sudanese groups with significantly more household possessions. Sudanese refugees reported lower mean daily food intakes (1.4) than either Ugandan (2.1) or Sudanese (1.8) nationals. Prevalence of traumatic events ever and in the past year for the three population groups are presented in table 2. Most of the traumatic events — ever or in the past year — were more prevalent in Sudanese refugees. This was determined by calculating the mean number of the different types of traumatic events reported by respondents, separately for experiences ever and in the past year. The resulting values are presented in table 3. The mean number of different types of traumatic events experienced differed significantly between the three populations. Sudanese refugee men and women have the highest exposure to different types of traumatic events, especially sexual violence, ever and in the past year. Post-hoc analyses revealed that each population group differed from the other groups (p<0.01) for traumatic event exposure ever, with the Sudanese groups reporting more events than Ugandan nationals. Post-hoc analyses also revealed that only the Sudanese refugees differed from the other populations with respect to traumatic event exposure in the past one year, with the difference between the Ugandan and the Sudanese nationals not being significant. Traumatic event exposure, ever and in the past one year, were further tabulated by experienced and witnessed events. The differences in the three population groups were significant with Sudanese refugees reporting the highest numbers of experienced as well as witnessed traumatic events Prevalence of PTSD symptoms by citizenship status and sex is presented in Figure 2. As expected the Sudanese groups had a higher burden of PTSD symptoms than the Ugandans. Fifty percent of all Sudanese refugees interviewed presented with symptoms of PTSD compared to 44% of Sudanese nationals and 21% of Ugandan nationals. The difference in prevalence between the groups is significant (p<0.01) with significant pair wise differences between Ugandan and the Sudanese nationals (p<0.01), Ugandan nationals and the Sudanese refugees (p<0.01), and the two Sudanese groups (p<0.05). The prevalence of PTSD symptoms among males and females differed significantly in the Ugandan national (p<0.01) Sudanese national (p<0.01) and the Sudanese refugee (p<0.01) population groups. Examination of the sex differential reveals an interesting pattern. While more females than males suffer from the symptoms of PTSD in Uganda, Ugandan nationals as well as Sudanese refugees, there is a reversal in the sex ratio in the Sudan. Assuming a male-female ratio of 1, population prevalence of PTSD can be estimated at 18% for Ugandan nationals, 48% for Sudanese nationals and 46% for Sudanese refugees. Individual, household, and migration variables that were 90% significant in bivariate analyses, after controlling for age, were entered into a multiple logistic regression model to determine associations with PTSD outcomes. About 31% (adjusted count R2) of the variance in the probability of developing PTSD symptoms is explained by the regression analysis model. Results of the analyses, odds ratios and robust estimates of variance with significance levels and confidence intervals, are presented in table 4. The analyses revealed associations with socio-economic, migration and trauma related variables after controlling for the influence of age. The likelihood of developing symptoms of PTSD increased with age, with women significantly more likely to suffer than men. Having some education or a salaried job were protective factors while neither marital status nor religion had significant associations with the development of PTSD symptoms in the sampled population. Household possessions, an indicator of income, decreased risk of PTSD in individuals. Other household level variables such as number of meals and number of years spent in current residence were not significantly associated with a PTSD outcome in this model. Migration history was significantly associated with PTSD outcomes. Contrary to expectations, a history of migration reduced the risk of PTSD after controlling for age, socio-economic factors and traumatic experiences. Likelihood of developing symptoms of PTSD increased however with the witnessing of traumatic events, ever and in the past year. DISCUSSIONThe results of the study indicate a substantial mental health burden, especially in the Sudanese populations. It is important to note that the presence of symptoms alone does not mean an impairment of functions in the individual. In spite of ethnic and cultural similarities, there were significant socio-economic differences in the three groups. Important differences were found with regard to the respondents’ marital status, religion, occupation, education, economical situation and migration history. Even though a high number of Ugandans report having had at least one experience of forced migration (66%), political stability seems to have helped improve their lives. They have more possessions and are better educated than the Sudanese. War has wreaked havoc on the lives of the Sudanese. The data seems to suggest that flight from one’s home is indeed a successful strategy against the possible experiencing or witnessing of traumatic events. The experience of migration in itself does not seem to predict PTSD when controlled for age, socio-economic factors and traumatic events. The breakdown of economy has meant that the Sudanese nationals have very few possessions. Poverty combined with insecurity has led many Sudanese to seek refuge in Uganda where they have access to food, health care and education. There are signs, however, that food aid and land provided for cultivation has not had its intended effect. Much of the land put aside for refugees was arid and rocky and not suitable for agriculture. The two groups that reported high land ownership also had higher daily intake of food, highlighting the importance of land ownership and agriculture in nutrition. It is possible that those who own land are less likely to migrate. Far fewer refugees are engaged in agriculture than either the Ugandans or the Sudanese nationals. The influence of occupation was minimal with those with salaried jobs having a smaller probability of suffering from PTSD symptoms. This group consisted mainly of those in privileged positions such as politicians and village leaders who might be protected from stressors that affect the rest of the population. Sex, age, and education also proved to have significant associations with symptoms of PTSD. The finding that being female and being less educated increased the risk for symptoms is similar to observations made in North American populations.18 In addition, being older increased risk of being symptomatic. This could be attributed to loss of family members and social support, subsequent to war and forced migration. There are significant differences in violent and traumatic events experienced by the three population groups. As expected, the Sudanese, refugees followed by nationals, reported the highest exposure. The respondents who continued to live in southern Sudan experienced a relatively safe year as the front line in the war between the northern government and the southern armed groups had moved elsewhere. Refugees, on the other hand, continue to experience a high level of insecurity in their country of exile, although under the protection of the Government of Uganda (GoU) and the United Nations High Commissioner for Refugees (UNHCR). They have been threatened and attacked by Ugandan as well as Sudanese rebels during their stay in Uganda. Refugees also face considerable threats from within the settlements.24 25 44 Reported high on the list were robberies, extortions, beatings, torture and harassment by officials and armed personnel. This data set highlights the need for better protection guarantees for refugees in settlements as they continue to be targets of violence. The most relevant predictor for the development of symptoms of PTSD in the three West Nile population groups is the witnessing of a traumatic event (particularly of a recent one). Regression analyses show that traumatic events experienced in the preceding year were more predictive than traumatic events ever experienced. Contrary to our expectations, witnessed events turned out to be more significant in predicting symptoms of PTSD than experienced events. An explanation could be that the refugees continue to be in an insecure state and that witnessing increases anxiety levels and the expectation that the same could happen to them. Whereas, having survived a violent act may have a limiting effect on levels of anxiety in some of the survivors. On the other hand, it could also be that respondents were unwilling to admit being a victim of a worst type of traumatic experiences like sexual violence. These survivors may inaccurately report having witnessed, rather than experience the traumatic event. The sex distribution of symptoms of PTSD varied among Sudanese nationals and refugees. While Sudanese national and refugee populations showed similar prevalence, there is a significant difference in how the disorder affected males and females. Significantly higher numbers of refugee females suffer from symptoms of PTSD than their male counterparts. This resembles the pattern observed in Ugandan nationals and other populations.18 However, there is a marked reversal of this sex differential in the Sudanese national population. This could be because women who are most at risk are more likely to seek refuge or because men who stay behind are more likely to be recruited by rebel forces and actively participate in the conflict, therefore experiencing, witnessing or committing more violence. Researchers recognize that study results do not fully explain the relationship between war, forced migration and PTSD. There may be additional variables not explored in the study that may contribute to the high levels of mental health morbidity in refugee populations. When initial reception by host government authorities and humanitarian agencies are impersonal and threatening, refugees may assume roles of dependency and helplessness.45 While developments of social networks, family reunions and permanent settlements46 do occur, harsh living conditions, continued anxiety about forced repatriation and uncertainties regarding resettlement can cause considerable stress for the refugees. Host country refugee policies are also dictated by domestic concerns and not necessarily determined by security and protection concerns or by the wishes of host communities in receiving countries.47 A limitation of this study is that the only mental health variable considered by this study is PTSD. In populations that suffer from war, a high level of depression,17 18 anxiety, psychosocial dysfunction, and unexplained somatic symptoms can be expected in addition to PTSD, resulting in a considerable mental health burden. A previous study in a similar Sudanese refugee population19 showed high levels of depression and its correlation with PTSD. This study has also not explored the relationship between symptoms of PTSD and the ability of those affected to cope and function as members of a household and a community. The extent to which communities can remain functional when burdened with large numbers of individuals living with severe mental impairments also needs to be researched. CONCLUSIONThis study highlights the association between high exposure to violent events and the development of PTSD symptoms in populations that have been exposed to war and forced migration. Sudanese refugees in Uganda continue to experience traumatic events and as a consequence present with high levels of symptoms of PTSD, in spite of being under the protection of UNHCR and the GoU. This underlines the need for secure settlements with effective camp or settlement policing and justice system that will help reduce the number of stressors in the life of a refugee. Moreover, humanitarian organisations should pay equal attention to physical as well as mental health problems faced by populations affected by war and forced migration. ACKNOWLEDGEMENTJohns Hopkins University (Center for International Emergency, Disasters and Refugee Studies, Hopkins Population Center), Makerere University (Department of Population Studies, Makerere Institute for Social Research), Universität Konstanz (Department of Psychology) and Médecins sans Frontières – Holland collaborated to make this study possible. The authors would like to thank Dr. Ayiga Natal, Prof. John Ssekematte-Ssebuliba, the community leaders, the research team, and the respondents in Uganda and the Sudan for their support and participation in the Demography of Forced Migration Project. We also thank Prof. Ray Langsten for reviewing survey methodology and training the research team. We would like to thank Prof. Barbara Harrell-Bond for her unstinting support as well as invaluable theoretical and methodological contributions to the study. Funding / Support: This study was supported by a USAID Grant HRN-A-00-96-90006-00 through the Linking Complex Emergencies and Relief Transition Initiative (CERTI), funds from the Andrew W Mellon Foundation and the Deutsche Forschungsgemeinschaft. Unni Karunakara did much of the work for this paper as a Visiting Study Fellow at the Refugee Studies Centre, University of Oxford supported by a Population Council Social Sciences Fellowship. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04016f2.jpg] [hs04016f1.jpg] [hs04016t3.jpg] [hs04016t4.jpg] [hs04016t2.jpg] [hs04016t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}