 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 4, No. 2, August, 2004, pp. 94-101 Total lymphocyte count of 1200 is not a sensitive predictor of CD4 lymphocyte count among patients with HIV disease in Kampala, Uganda Moses R. Kamya1, 2*, Fred C. Semitala2, Thomas C Quinn2, 3, Allan Ronald2, Denise Njama-Meya1,Harriet Mayanja-Kizza1, 2, Elly T. Katabira1, 2, and Lisa A. Spacek3 1Makerere University Medical School, Kampala, Uganda ABSTRACT Introduction: Total Lymphocyte Count (TLC) has been found to be an inexpensive and useful marker for staging disease, predicting progression to AIDS and death and monitoring response to ART. However, the correlation between TLC and CD4 has not been consistent. Access to HAART is expanding in Kampala, Uganda, yet there are no published data evaluating the utility of TLC as inexpensive surrogate marker of CD4 cell count to help guide therapeutic decisions. Key words: CD4 cell count, total lymphocyte count, clinical algorithm, antiretroviral therapy, resource limited settings. Short title: Lymphocyte count as a predictor for CD4 levels INTRODUCTION
Some of the critical barriers to increased access to antiretroviral therapy (ART) in Uganda are the high cost of the medications and the associated laboratory monitoring to ensure safe and effective use of these drugs. Over the last few years, the prices of antiretroviral drugs have decreased in Ugandathrough negotiation and generic price competition. In addition, there is optimism that new sources of funds, such as the Global Fund for HIV/AIDS, Tuberculosis, and Malaria, are becoming available to support care [www.aidspan.org/globalfund]. Currently, the cost of monitoring ART far exceeds the price of non-nucleoside reverse transcriptase inhibitor-based ART and remains a critical barrier to HIV care. The cost of CD4 lymphocyte count (CD4) varying between US $15 - 30 is comparable to the cost of a one-month supply of the commonly used generic combination pill, Triomune (d4T, 3TC& nevirapine). There is urgent need to evaluate alternative, inexpensive markers to initiate HIV therapy in Uganda. In areas where resources are available, decisions to initiate treatment for HIV disease are routinely based on algorithms that combine CD4, HIV viral load, and clinical illness. In April 2002, WHO released guidelines intended to expand access to ART to 3 million people with HIV/AIDS by 2005 in resourcelimited settings1. The guidelines recommend that if CD4 testing is unavailable, ART is indicated for patients in WHO clinical stage 4 irrespective of total lymphocyte count (TLC) and for patients in WHO clinical stage 2 or 3 with a TLC below 1200 cells/ mm3 . Prior studies have shown a correlation between TLC and CD4 in HIV-infected patients in the United Kingdom2, and the United States3. Moreover, TLC has been found to be an inexpensive and useful marker for staging disease, predicting progression to AIDS and death and monitoring response to ART4. The use of TLC below 1250 cells/mm3as a predictor of HIV disease progression as compared to CD4 below 200 cells/mm3 was evaluated in South Africa5. The results suggested that TLC of 1250 cells/mm3 is equivalent to CD4 of 200, and that TLC above versus below 1250 cells/ mm3 is associated with significantly different rates of HIV disease progression. In 405 HIV infected patients seen in Chennai, India, Kumarasamy and colleagues advocated using TLC below 1400 cells/ mm3 to predict CD4 below 200 cells/mm3 6 . Given the greater availability and markedly lower cost of TLC, there is a clear argument to proceed with HIV disease treatment and prophylaxis of opportunistic infection based on the TLC level. However, the correlation between TLC and CD4 has not been consistent. A large study from South Africa demonstrated that TLC was not a good predictor of the CD4 in their population7. A smaller study in Nigeria using manual counts for CD4 and TLC found a weak correlation among patients monitored on ART8. Clinical algorithms that combine clinical illness related to HIV infection with inexpensive laboratory tests may allow HIV treatment providers to predict CD4. Combining TLC measurement and clinical characteristics with additional basic laboratory data such as hemoglobin has been shown to increase sensitivity and thereby decrease the risk of false-negative results. In a recent study9, Spacek et al. developed an algorithm to combine TLC and hemoglobin to predict CD4<200 cells/mm3 based on a retrospective analysis of HIV-infected individuals followed in the Johns Hopkins HIV Cohort. Such a clinical algorithm may be useful in settings where laboratory resources are limited to a complete blood count. Access to HAART is expanding in Kampala, Uganda, yet there are no published data evaluating the utility of TLC as an inexpensive marker of CD4 cell count to help guide therapeutic decisions. The primary objective of this study was to evaluate clinical illnesses and total lymphocyte count (TLC) as surrogate markers of the CD4 cell count in HIV infected persons being considered for ART. We examined the relationship between TLC and CD4 and assessed clinical illnesses and TLC dichotomized at various cut-point values to determine the sensitivity, specificity, and predictive values for the diagnosis of a CD4 count <200 cells/mm3. PATIENTS AND METHODS Study site: In March 2002, the Academic Alliance for AIDS Care and Prevention in Africa, Infectious Disease Clinic (IDC) was opened. By February 2003, over 1400 new patients had been registered. Over 200 patients are seen each week and approximately 20% of the clinic visitors are new patients. The majority of patients have advanced AIDS. The clinic provides free HIV care including counseling, treatment of opportunistic infections and other HIV related complications and lab tests (excluding viral load and viral resistance testing). The clinic provides information to patients concerning the benefit of ART and how to access the drugs. Clinic patients who wish to initiate ART are offered free complete blood count and CD4 lymphocyte count tests. Those who are eligible with CD4 <200 cells/mm3 or WHO clinical stage 4 are given a prescription for purchase of the drugs. Currently, these medications are obtained through out of pocket financing, as free antiretroviral medications are not available in the clinic. Patients pay for ART based on a sliding scale and costs are supplemented by cash donations from individual donors and corporate sponsorships. Study subjects and measurements:
From June 2002 to February 2003, one hundred and thirty seven consecutive patients seen at the IDC at Mulago hospital in Kampala, Uganda, who had obtained CBC and CD4 measurements on the same blood sample, were eligible for the study. These study subjects were assessed for clinical illnesses on the same day as the lab test measurements. A standardized data collection form was completed for each patient. Patient data on enrollment included demographics, clinical and laboratory data. The data set was de-identified and no addresses, unique identifiers or patient visit dates were included. The study was reviewed and exempted from consent by the Johns Hopkins Medicine and the Makerere University Faculty IRBs. Clinical data included both past history of and current illness with oral thrush, herpes zoster, pulmonary tuberculosis, chronic diarrhea, pruritic dermatitis, Kaposi’s sarcoma, and cryptococcal meningitis. Two study physicians determined the WHO clinical stage10 . Laboratory data included CD4 measured by a FACS Counter (Becton Dickinson, San Jose, CA, USA) and complete blood counts by coulter (Beckman Coulter ACT diff 2) including hemoglobin (Hb), white blood cell count (WBC), total lymphocyte count (TLC), and absolute neutrophil count (ANC). All blood indices were done on the same sample for each patient. The lab tests were done at the Makerere University-Johns Hopkins University Core Lab at Mulago Hospital in Kampala, Uganda. The CoreLab follows GCP and GLP guidelines and Quality Control is monitored by internal controls and external proficiency programs. Quality Assurance and Quality Improvement Programs are in place. This lab has recently been accredited by the College of American Pathologists. Statistical methods:
The data were entered in Epi info and analyzed in SAS. Correlations between CD4 laboratory values of interest (Hb, WBC, TLC, and ANC) were evaluated using Spearman rank correlation. Clinical illnesses and TLC dichotomized at various cut-point values were used to determine the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for the diagnosis of a CD4 cell count less than 200 cells/mm3. The correlation between CD4 and the number of reported illnesses was evaluated using the Kruskal-Wallis test. Receiver operating characteristic (ROC) curves were generated to predict CD4 < 200 cells/mm3 for 100 patients in WHO clinical stage 2 or 3. RESULTS:
During the study period, a total of 137 patients were tested for CD4 and TLC on the same blood sample. One hundred and thirty one were enrolled in this study. Six patients were excluded due to incomplete data. In 110 of 131 enrolled patients, both CD4 and TLC were measured as baseline investigation prior to initiation of ART, whereas in 21 patients the tests were done to monitor ART. CD4, TLC and WHO clinical stage in the IDC population
Table 1 shows the participant characteristics and lab data by gender. The majority of the patient population had advanced HIV disease. The mean CD4 count was 123.6 cells/mm3 (SD, 141.6) and the median CD4 was 66.0 cells/mm3 (IQR, 10-192). Of 131 patients, 57 (43.5%) patients had a CD4 cell count of <50 cells/mm3, 46 (35.1%) had counts between 50 and 200 cells/mm3, and 28 (21.4%) had counts of >= 200 cells/mm3. Despite the low CD4 counts in our study patients (median, 66 cells/ mm3), TLC values in this population were high (median, 1500/mm3). Table 1. Participants’ characteristics and laboratory data by gender
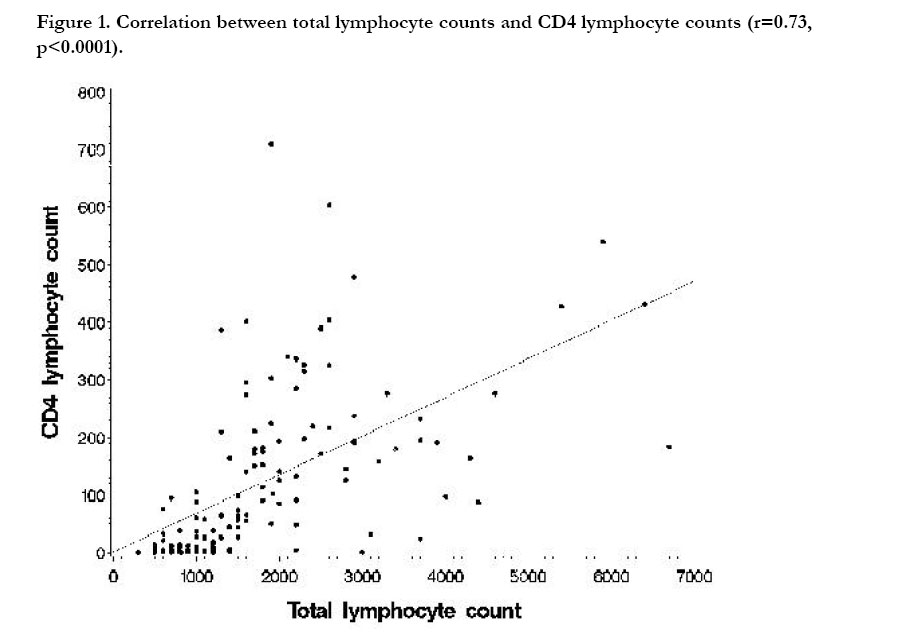
Table 2 shows the median CD4 cell count and median total lymphocyte count by WHO clinical stage. Median CD4 declined with advancing WHO stage (p=0.04). 2 participants were WHO stage 1 (median CD4, 518), 20 were WHO stage 2 (median CD4, 158), 80 were WHO stage 3 (median CD4, 71), and 29 were WHO stage 4 (median CD4, 32). A strong correlation was observed between TLC and CD4 (r = 0.73, p<0.0001, Fig. 1). ANC, Hb levels and total WBC count were not correlated with CD4 count (data not shown). Table 2. Median CD4 cell count and total lymphocyte count by WHO clinical stage
Clinical illness to predict CD4 Table 3 shows the current and past illnesses that were identified in our study subjects and lists the sensitivity, specificity, PPV and NPV of current or past illness to predict CD4 below 200 cells/mm3. The common illnesses included oral thrush, herpes zoster, pulmonary tuberculosis, and pruritic dermatitis. For all clinical syndromes, except pulmonary tuberculosis, the PPV to predict CD4 <200 cells/mm3 were high (>80%) but the sensitivities and NPV were low. Therefore, the presence of clinical illness was associated with low CD4. Yet due to poor sensitivity, lack of clinical illness does not rule out low CD4. The median CD4 count by illness showed a significant correlation. For current illness the median CD4 of patients without any current illness (n=46) was 188 cells/mm3, with one reported illness (n=67), the median CD4 count was 48 cells/mm3, and with two or more reported illnesses (n=18), the median CD4 count was 9 cells/mm3 (Kruskal-Wallis test, p=0.0001). Table 3. PPV, NPV, sensitivity, and specificity to predict CD4 below 200 cells/mm3
TLC to predict CD4 (WHO stages 2 and 3)
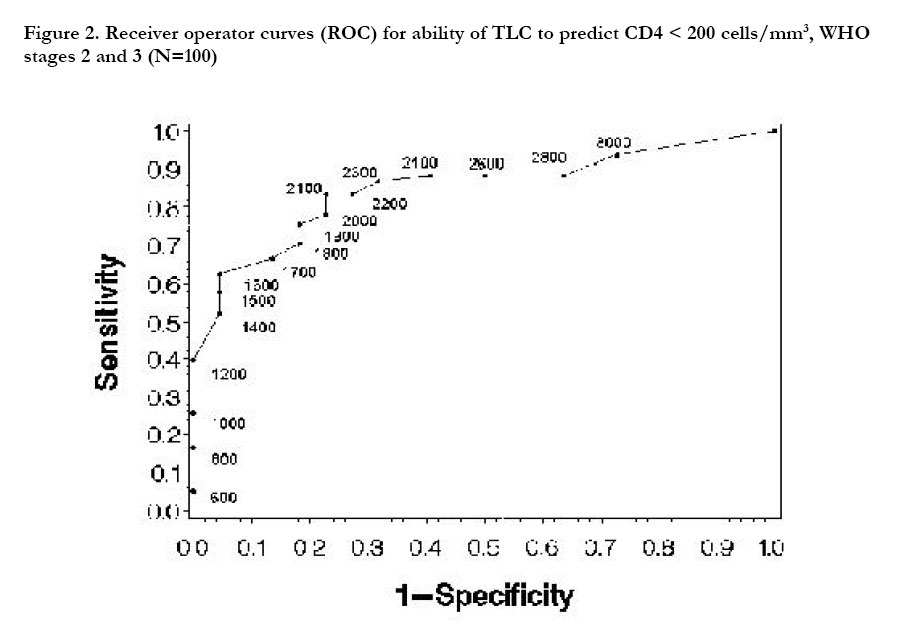
Table 4 shows the sensitivities, specificities, and positive and negative predictive values for various cut-offs of TLC, to predict CD4 cell count below 200 cells/mm3. Based on WHO guidelines, whereby patients in clinical stage 1 are not treated and those in clinical stage 4 are treated without further testing, this analysis was limited to 100 participants in WHO clinical stage 2 and 3. Mean age was 37.1 years (SD 8.8) and 62.0% of participants were women. Sensitivities and specificities were used to construct receiver-operator characteristics (ROC) curves (Figure 2). Sensitivities, specificities, and predictive values depended greatly upon TLC cut-offs. There was an increase in sensitivity and a decrease in specificity as the cut-off for the TLC increased. A TLC cut-off of 1800-1900/mm3 best predicted CD4 < 200 cells/mm3. Table 4. Sensitivity, Specificity, and Predictive Values of Varying Cut-offs for TLC, in identifying CD4 Counts of < 200 Cells/mm3
For TLC of 1200 cells/mm3, sensitivity was 39.7%, specificity was 100%, PPV was 100%, and NPV was 31.9%. Therefore, use of the cutoff of 1200 cells/mm3 or less will identify only 39.7% of individuals with a CD4 less than 200 cells/mm3 resulting in a high risk of false negative results. However, the specificity at this point is 100%, indicating that all individuals with a TLC less than 1200 cells/mm3 will have a CD4 count less than 200 cells/mm3. To predict CD4 less than 200 cells/ mm3, TLC cut-point of 1800 cells/mm3 would result in sensitivity of 70.5% with 29.5% false negative results. TLC of 1900 cells/mm3 would result in a sensitivity of 75.6%, and 24.4% false negative tests. In order to increase sensitivity, a higher TLC cut-off is required but would sacrifice specificity. DISCUSSION: Uganda is at the verge of increasing access to ART but the decision when to start treatment among patients in WHO clinical stage 2 & 3 in the absence of a CD4 count determination is still unclear. In this study, we were particularly interested in the use of clinical findings and TLC to predict CD4 count in a routine clinical setting in a resource-poor setting. Importantly, we found that TLC in our population w as high (m edian TLC, 1500 cells/mm 3) and yet patients had advanced HIV disease (median CD4, 66 cells/mm3). The normal TLC in adult Ugandans ranges between 1300 and 4200 cells/mm3 11 and is similar to normal values from western countries. However, given advanced HIV disease and low median CD4, the median TLC in this population was considerably higher than that seen in other studies2,5,6. In advanced HIV infection, the TLC is expected to decline as a result of progressive depletion of CD4+ T-lymphocytes, CD8+ Tlymphocytes and B-lymphocytes12. Further evaluation is needed to examine the observed elevated lymphocyte count in advanced HIV infected patients. Possibilities that might be associated with elevated lymphocytes include tuberculosis, viral and or parasitic infections, which are more frequent in our population, compared to other populations. Our findings show a strong correlation between TLC and CD4 (r = 0.73, p<0.0001). Similar correlations between TLC and CD4 have been reported in North America13, England2 and India6. Despite this strong correlation, our data show that in this population, the WHO guideline of TLC 1200 cells/mm3 is not a sensitive predictor of CD4 below 200 cells/mm3. Using TLC below 1200 cells/mm3 in the group of patients included in the present study, sensitivity was only 39.7%, specificity and PPV were 100%, and NPV was 31.9%. Therefore, use of the cutoff of 1200 cells/ mm3 or less will identify only four of ten individuals with a CD4 below 200 cells/mm3 (as an indication to start ART among patients with stage 2 and 3 disease), resulting in a high risk of false negative results. However, owing to the high specificity (and PPV), patients who have CD4 counts >200 are unlikely to be treated. A more sensitive cut-off would require a higher TLC cutoff and sacrifice specificity. Studies show variable levels of sensitivity of TLC to predict CD4 count3. Some studies have found TLC as a useful indicator of significant immunosuppression as measured by a CD4 cell count of <200 cells/mm3. In one study5, a TLC of 1250 was equivalent to a CD4 count of 200 and the presence of a TLC above or below 1250 is associated with a significant difference in rates of progression of HIV infection. Other studies have not found TLC to be a good predictor of CD47 and low predictive values have been observed among patients with relatively early HIV disease3,13. Even in studies where the correlation is strong (r=0.7), maximizing sensitivity (sensitivity is maximized at the highest TLC values) and identifying most people with the disease, results in lowering of positive predictive values (maximized at the lowest TLC ranges)6. Thus one TLC cut off may not necessarily apply to populations from different parts of the world. In our patient population, the most frequently reported illnesses included a history of oral thrush or tuberculosis and current illness with oral thrush or pruritic dermatitis. A majority of patients were in WHO stage 3. Among patients with WHO stage 2 or 3 disease, Current or past symptoms had a high positive predictive value (with the exception of TB, all PPV were >80%) but low sensitivity of identifying patients with CD4 less than 200 cells/mm3. Patients reporting any AIDS related illness had median CD4 counts well below 100 cells/mm3. Moreover, we found that a report of more than one illness was significantly associated with greater immunosuppression. Our results show that symptomatic HIV infected patients should be considered for starting HAART irrespective of their TLC levels. Yet due to low sensitivity, lack of clinical illness does not rule out low CD4. In particular, pruritic dermatitis strongly predicted CD4 count of less than 100 and less than 200 cells/mm3. The correlation of AIDS related clinical features with the degree of immunosuppression as measured by CD4 count was evaluated in a longitudinal study of the Masaka, Uganda natural history cohort 14,15. The median CD4 lymphocyte count at the time of developing AIDS was 150 cells per cubic millimeter. Wasting syndrome, esophageal candidiasis, and Kaposi’s sarcoma were associated with median CD4 cell counts of 150, 101, and 208 cells per cubic millimeter, respectively and median survival time of less than 3.5 months. Our results indicate that the WHO recommended TLC cut off of 1200 should be used with caution in some patient populations. If CD4 count is not available, informed decision making, incorporating clinical conditions, should be applied. Following TLC sequentially may have a role in staging of HIV positive patients but not to determine eligibility for HAART. A more rational use of TLC counts is to treat all patients with WHO stage 2 and 3 who have a TLC <1200 and to limit CD4 counts to patients who are symptomatic but have TLC of >1200. Alternatively, patients with multiple AIDS related illnesses should be treated if CD4 count testing is not available. Using a TLC count will cut back on the number of patients requiring a CD4 cell count. The current technology for measuring CD4 counts is too costly to perform and requires flow cytometry; these constraints severely limit the number of laboratories which can perform counts in resource constrained settings. One of the most crucial needs in the developing world is universal access to affordable and locally usable CD4 testing technology. This development is an urgent priority which should be pursued in parallel with the planned massive scale-up of ART. As a worldwide effort, simpler and less expensive CD4 testing such as the use of Dynabeads (16) and PanLeucogating are being developed (17, 18). PanLeukogating is cheaper because it leaves out the redundant use of monoclonal antibodies. Diagbouga et.al in West Africa reported the successful implementation of a low-cost alternative technique to flow cytometry (FC) for enumerating CD4 T cells. They used epifluorescent microscopy following CD4 T cell isolation using anti-CD4 monoclonal antibodycoated magnetic beads. Nevertheless, these inexpensive CD4 tests are not yet widely available. Our study had limited power to use a combination of WHO stage, clinical features and TLC and other lab parameters to develop predictive models for CD4 cell count. For example, only 28 (21.4%) patients in our study had CD4 counts of >= 200 cells/mm3. A clinical algorithm using TLC and clinical features to predict CD4 cell count in Uganda is warranted. Investigation of additional markers that are also inexpensive and widely available is needed. Conflict of interest statement None declared. ACKNOWLEDGEMENTS
We are indebted to the staff of the Infectious Disease Clinic and all patients who participated in the study. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04017t2.jpg] [hs04017f1.jpg] [hs04017f2.jpg] [hs04017t4.jpg] [hs04017t3.jpg] [hs04017t1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}