 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 4, No. 2, August, 2004, pp. 119-124 Health-seeking behavior for malaria among child and adult headed households in Rakai district, Uganda Beatrice Amuge1, Fred Wabwire-Mangen2, Chilunga Puta4, G.W. Pariyo2, Nathan Bakyaita5, Sarah Staedke3, Moses Kamya3, Olico-Okui2. 1 P.O. Box 5171 Jinja, Code Number: hs04021 ABSTRACT Background Keywords: Health seeking behavior, child-headed households, adult-headed households, AIDS, Orphans, Rakai, Uganda. INTRODUCTION Human immunodeficiency virus (HIV)/Acquired immunodeficiency syndrome (AIDS) has resulted in large numbers of orphans worldwide1. Uganda’s 1991 population and housing census identified 1,037,228 children below the age of 18 years (12% of this age group) who had lost at least one parent to AIDS2. Like other parts of Uganda, Rakai District continued to be engulfed by premature deaths more significantly due to HIV/AIDS. By the year 2000, the Orphan Community Based Organization (OCBO) reported 34,902 (28%) orphaned children below the age of 18 years in Rakai district and about 11,324 live in child-headed households 3 . Orphans not accommodated within the family of adults have to look after themselves, their siblings, and, in some cases, their elder relatives4. Child-headed households are likely to have poor housing, sanitation hygiene and malnutrition4 . All the members in child-headed house-holds are vulnerable to such diseases as malaria. Malaria has been historically a very serious health problem in Uganda. Currently it accounts for 24-40% of all out patient visits at health facilities and 20% of hospital admissions5. In Rakai district malaria is currently the leading cause of morbidity contributing to 36.7% of Out Patients Department (OPD) attendance6. Using malaria as a tracer condition, we conducted a comparative cross-sectional study to describe the health-seeking behavior among childand adult-headed households. We also learned reasons for choosing where health care is sought from heads of households in the two categories. The objective of the study was to compare the knowledge of the child- and adult-headed households on signs and symptoms of simple and severe malaria in Rakai-Uganda, their health-seeking behavior when malaria is suspected and the reasons for choosing where health care is sought for malaria. METHODS
A comparative, cross-sectional study design was used to collect information on health-seeking behavior from sample of 300 households (150child- and 150 adult-headed households). Pocock’s formula for comparing two proportions was used to estimate the sample size7. Two of the four counties in the district (Kooki and Kakuuto) were purposively selected for inclusion on the basis of their high numbers of child-headed households. In the selected counties, 50% of the sub-counties were also selected purposively. Lists of child headed-households in the selected sub-counties were obtained from the Orphaned Community Based Organization (OCBO) and Lutheran World Federation (LWF) offices in the district where one combine list was created. Every third household on the list was systematically selected until 150 child-headed households were obtained. The closest neighborhood adult-headed household to each childheaded household was selected for comparison. The respondents in child-headed households were the household heads or any child who was found present and could answer the questions. In adult-headed households, the head or spouse was interviewed. Twenty-six key informant interviews and six focus group discussions were purposively selected and conducted. Informed consent was obtained from all respondents prior to inclusion in the study. A semistructured questionnaire was then administered to obtain each respondent’s socio demographic and behavioral data. The socio-demographic data included age, sex, tribe, religion, education level and occupation. The behavioral data included knowledge of signs and symptoms of simple and severe malaria, first action taken when malaria is suspected, time lag before first action is taken, first treatment given and reasons for choosing where health care is sought for malaria. Data was cleaned, coded and entered into EPIinfo version 6. It was checked for consistency, analyzed and associations were measured using Odds Ratio test at < 0.05 significance level. RESULTS Socio-demographic characteristics of respondents in child- and adult-headed households These results were generated from 150 respondents in each type of household. Of the respondents in childheaded households 63/150 (42%) were within the age range of 11-15 years. Out of 150 respondents, 99 (66%) were male. Majority of the respondents 128/150 (85%) were Baganda which is the dominant tribe in Rakai district. By religion, 145/150 (97%) were both Catholics and protestants. Of 150, 114 (76%) who formed the majority had primary education and only 7/150 (5%) had no formal education. By occupation, 77/150 (51%) were pupils and students, and 73/150 (49%) were peasants. Of the respondents in adult-headed households, 73/150 (49%) were within the age of 19-35 years. Out of 150 respondents, 62 (41%) were male, The dominant tribe 112/150 (75%) was Baganda. Majority 139/150 (93%) of the respondents were both Catholics and protestants. Of 150, 82 (55%) had primary education and 46/150 (31%) had no formal education. By occupation 66/150 (44%) were peasants and 65/150 (43%) were housewives. Respondents knowledge of the signs and symptoms of malaria
The common sign and symptom of simple malaria, which was mentioned by the respondents in both child- and adultheaded households, was fever (Table 1). There was a significant difference (OR=0.43, CI=0.25-0.75, p-Value=0.001) between the respondents in child- and adultheaded households on the knowledge of fever as the major sign and symptom of simple malaria. There was also a significant difference in mentioning headache, joint pains, muscle ache, sweating, vomiting and loss of appetite as signs and symptoms of simple malaria. There was no significant difference in knowledge concerning nausea and shivering between the two types of households. Table 1. Comparison of respondents’ knowledge of the signs and symptoms of simple malaria
* Statistically significant association (P=<0.05) between the type of household and knowledge of the signs and symptoms of simple malaria. On signs and symptoms of severe malaria, the respondents in child-headed households were less likely to mention convulsions, fast breathing, jaundice and pallor as signs and symptoms of severe malaria than the adult heads of households (Table 2). The respondents in child-headed households were 2 times more likely not to know any sign and symptom of severe malaria than the adult heads of households. Table 2. Comparison of respondents’ knowledge of the signs and symptoms of severe malaria
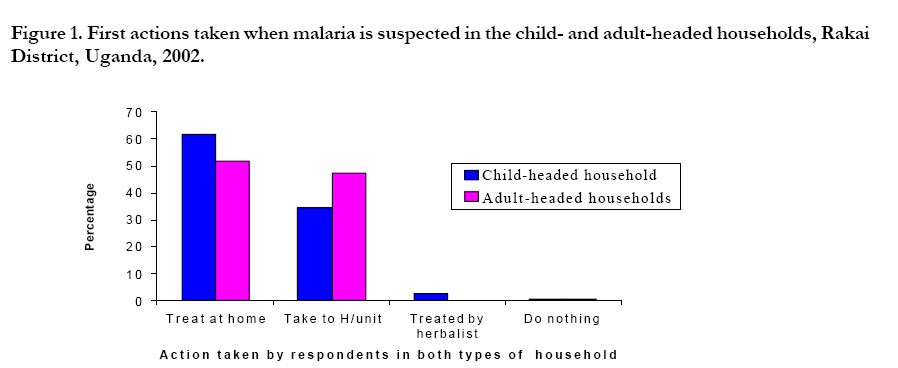
* Statistically significant association (P=<0.05) between the two types of households and knowledge of the signs and symptoms of severe malaria. First action taken when malaria is suspected The first actions taken included (a) treating the sick person at home, (b) taking the sick person to health unit, (c) taking the sick person to a herbalist, and (d) taking no action (Figure 1). The respondents in child-headed households were less likely than the adult heads of households (OR=0.59, CI=0.36-0.97, P value=0.028) to seek care at health units. During focus group discussion and key informant interview, it was commonly reported that the majority of people take home treatment and health facilities are used incase of failure. (Figure 1). The respondents in child-headed households treatment and health facilities are used incase of failure. Time lag before first action is taken Of the respondents in child headed household, 95/ 146 (65%) while adult heads of household 106/147 (72%) reported taking action within two days after suspecting malaria. The difference in time lag before first action is taken for malaria among respondents in child- and adult-headed households was not statistically significant (OR=0.72, CI=0.42-1.22, P value = 0.194). First treatment given when malaria is suspected
Out of 95 respondents in child-headed households who reported taking action within two days 46 (48.4%) reported using local herbs as first treatment while in adult heads of households 15/106 (14%) reported using herbs as first treatment. The respondents in child-headed households were six times more likely to mention the use of local herbs than the adult heads of households (OR=5.70,CI=2.75-11.91, P value<0.001). The common local herbs mentioned by respondents in both types of households as being used for treatment of malaria were Mululuza” (Vernonia amygodalina), “Neem-tree” (Azedaract indica) and “Nyambala butonya” (Callistemon citranatus). Reasons for choosing where health care is sought for malaria Various reasons were mentioned for choosing where health care is sought for malaria in the child- and adult-headed households. The most common reasons mentioned were (a) distance to source of health care, (b) free/cheap treatment, (c) availability of drugs, and (d) quick attention to patients in the health-care facility. The respondents in child-headed households were less likely to mention distance to the source of health care (OR=0.55, CI=0.33-0.92, P value=0.014) and receiving quick attention (OR=0.41, CI=0.20-0.83, P value=0.007) as reasons for choosing where health care is sought than the adult heads of households (Table 3). Table 3. Reasons for choosing where health care is sought for malaria in child-and adult- headed households, Rakai District, Uganda, 2002
* Statistically significant association (P=< 0.05) between the two types of households and reasons for choosing where health care is thought for malaria. DISCUSSION Malaria remains a big health problem in Rakai district Uganda. The success of health intervention in malaria control needs the knowledge of the community’s perception of the illness and their health-seeking behavior. In this study, the common sign and symptom of malaria mentioned by respondents in both type of households was fever. Likewise a study done in Mali revealed that, fever, vomiting and dark urine/yellow eyes/jaundice were there most common signs mentioned by mothers whose children had uncomplicated malaria in the last rainy season8. This similarity is because malaria is currently one of the major health problems in Africa and people commonly present with fever. However, the respondents in child-headed households were less likely to mention fever, headache, joint pains, loss of appetite, muscle ache, sweating and vomiting as the signs and symptoms of malaria than the adult heads of households (Table 1). The respondents in child-headed households were three times more likely to know other signs and symptoms (cough, skin rash, weakness and diarrhea) which were not typical of malaria than adult heads of households. This shows that the respondents in child-headed households have less knowledge of the signs and symptoms of malaria, likewise the knowledge of signs and symptoms of severe malaria was found to be low among the respondents in child-headed households compared to the adult heads of households. This could be either due to less experienced or have no access to health messages or are too young to interpret health messages correctly. It implies that the respondents in child-headed households do not correctly recognize malaria and are therefore liable to practice inappropriate health seeking behavior. In response to severe malaria the child-headed households may not appreciate the need for urgent action, which leads to a delay in seeking appropriate health care and avoid preventable death. To create awareness in the child-headed households, they should be recognized and specifically targeted for health education programs. Such programs could be implemented in the skills training centers for orphans in collaboration with Non-Governmental Organizations, which support the child-headed households in Rakai district. The initial action taken by respondents in both types of households include taking home treatment, seeking health care from health units, going to herbalists, and at times doing nothing. The respondents in child-headed households were less likely (OR=0.59, CI=0.36-0.97, P-value=0.028) to seek health care from health facilities than the adult heads of households. This could be because the respondents in childheaded households less knowledge on signs and symptoms of malaria. It also implies that the child-headed households are likely to stay in the village without treatment or seek health care from informal health care systems and to take treatment without consulting the adults, this leads to mismanagement of illness and probably death. A study done in western Kenya among Luo school children showed that they used self-treatment for common illness, and that only 28% sought advice about health care from available adult10. Likewise the study conducted in Lusaka, revealed that there was a high degree of unmet needs for health services and many people were self medicating due to lack of funds rather than that they perceived their illness as minor or uniimportant9. These studies all point out issue of self-medication, which is probably cheap and within reach, reducing the consequence of cost and distance. The respondents in both types of households had no significant difference in time lag before first action taken after malaria is suspected, but the type of action taken varied. The respondents in child-headed households were mainly using home treatment, which may be easily available and affordable. Both respondents in child- and adultheaded households mentioned using Western medicines and local herbs in treatment of malaria. However, the respondents in child-headed households were six times more likely to mention the use of local herbs than the adult heads of households. This is likely to reflect the much lower level of financial capacity in child-headed households to purchase drugs. Locally available herbs can probably be gathered at no cost. The use of local herbs may not be effective for treatment of malaria and may result in serious illness, and ultimately death, it also causes delay in obtaining effective treatment. The respondents in child-headed households may also not know how these local herbs should be used, their doses, and the actual efficacy of most of these herbs has not been determined. A study conducted in Mulago revealed that mothers were treating children for malaria with herbs11. This demonstrates further that the use of herbs is still common in many areas in Uganda. It is important to sensitize the community about use of local medicines and it’s dangers. The major reasons mentioned for choosing where health care is sought was distance to source of health care, free and cheap treatment. The respondents in child-headed households were less likely to mention distance to source of health care than adult heads of households. This prob-ably reflects the more common practice in childheaded households of relaying on home treatment involving self-medication and could not think of distance as a problem. The community tends to use nearby places to eliminate transport costs. Implementation of the Ministry of Health, Uganda, policy on household (home) management of malaria and supply of home pack program should target the child-headed households. Study limitations
Selection of the counties and sub-counties basing on their high numbers of child-headed households in the district could have created selection bias. The counties and sub-counties with low numbers of the child-headed households may have different characteristics. This study catered for only children who are registered by Non-governmental organizations (NGOs) in Rakai district. Other child heads of household may exhibit a different health-seeking behavior pattern and may have different reasons to account for that behavior pattern. ACKNOWLEDGEMENTS
I acknowledge the Rockefeller Foundation, for financial support throughout the course of training and initial funding of this study. Sincere thanks go to the Uganda Malaria Surveillance Project (CDC Award No: S1932-021/21 entitled; “Malaria Surveillance and Control in Uganda”), which is a collaboration between the Makerere University Institute of Public health, the School of Public Health at University of California-Berkeley and the Ministry of Health Uganda for the financial support towards completion of this study. I must thank the Rakai District Health Team, various Non-Governmental Organizations in Rakai districts, field guides and respondents for their maximum co-operation throughout data collection. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04021t1.jpg] [hs04021t3.jpg] [hs04021t2.jpg] [hs04021f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}