 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 4, No. 2, August, 2004, pp. 131-135 Effect of the ferrule on fracture resistance of teeth restored with prefabricted posts and composite cores Annet Kutesa-Mutebi1, Yusuf I Osman2 1 Makerere University, Faculty of Medicine, Department of Dentistry. ABSTRACT Background: The ferrule effect in root treated teeth requiring cast posts and cores has been shown to greatly improve fracture resistance. Studies have also shown that in the case of a cast post and core, the longer the ferrule, the greater the fracture resistance. However few studies have considered the effect of different ferrule designs on prefabricated post and composite core systems. Key Words: Endodontically treated teeth, Fracture resistance, Preformed Post, Composite core, Ferrule design, Ferrule effect, Ferrule length, Shoulder, Bevel, Contra-bevel. INTRODUCTION The use of prefabricated posts with amalgam, composite resin or reinforced glass ionomer core build-ups has become very popular 1 . In-vitro, and clinical studies have shown that prefabricated post systems perform as well as or even better than the cast post and core 2,3,4 . Factors that may affect these restorations include crown design5 . Crowns have been shown to alter the distribution of forces to the roots and provide a bracing or casing action to the tooth referred to as the ferrule 6 . A ferrule has been defined as a metal ring or cap intended for strengthening the end of a stick or tube7 . Sorensen and Engelman 8 suggested that this “ferrule effect” be defined by a 360-degree metal crown collar surrounding parallel walls of dentine and extending coronal to the shoulder of the preparation. Libman and Nicholls 9 defined it as a metal band or ring used to fit the root or crown of a tooth. The ferrule or encircling band of cast metal around the coronal surface has been suggested to reinforce the coronal aspect of the dowel preparation and acts as an antirotatory device6. It has also been shown to greatly improve fracture resistance 10, 9, 11, 12, 13 . Loney14 found that the collar had a significant effect on stress distribution. He suggested that the ferrule may help to unite different portions of the tooth. It has also been suggested to act as an antirotatory device6 , and to maintain the cement seal. Libman & Nicholls9 suggested that to achieve the full benefits of the ferrule effect it should be a minimum of 1.5 mm in height and have parallel dentine walls, totally encircle the tooth, end on sound tooth structure and avoid invasion of the attachment apparatus of the tooth. Most of the studies investigating the ferrule effect have used cast posts and cores, few studies have considered a ferrule effect or design on prefabricated posts and composite core systems15, 4,16 . The aim of this study was to investigate the effects of different ferrule designs on the fracture resistance of teeth incorporating prefabricated posts and composite cores. In addition the teeth were also be compared to teeth having a composite core without any post. MATERIALS AND METHODS
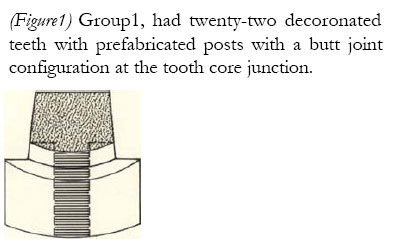
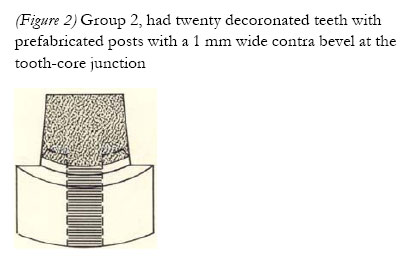
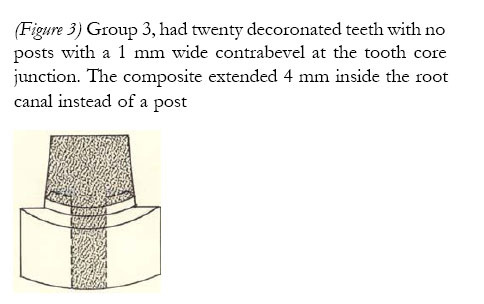
Sixty-two extracted maxillary incisors (centrals & laterals) and canines were collected. The teeth were visibly inspected and only those with minimal caries were included in the study. Teeth with fractures or cracks were excluded. The teeth were stored in a thymol solution at room temperature to prevent bacterial growth. The endodontic treatment was completed for all the teeth using the standardised technique17. Each tooth was instrumented according to clinical guidelines in relation to its size, using reamers and K files. During instrumentation, copious irrigation was performed with saline. The canals were dried with air and absorbent paper points. They were obturated using gutta percha points by lateral condensation with the aid of a finger spreader. Tubliseal (De trey/ Dentsply) was used as the cement for obturation with gutta percha. The teeth were decoronated 2mm (proximal surface) above the cemento-enamel junction perpendicular to their long axis using a model trimmer with a continuous water coolant. All teeth had a crown preparation with a 900 shoulder 0.5mm in width following the cemento-enamel junction. The shoulder margin was prepared using a conventional high-speed handpiece with a flat-ended fissure diamond bur. The teeth were distributed into three groups (figures 1, 2, & 3) (Figure 1) Group1, had twenty-two decoronated teeth with prefabricated posts with a butt joint configuration at the tooth core junction. (Figure 2) Group 2, had twenty decoronated teeth with prefabricated posts with a 1 mm wide contra bevel at the tooth-core junction (Figure 3) Group 3, had twenty decoronated teeth with no posts with a 1 mm wide contrabevel at the tooth core junction. The composite extended 4 mm inside the root canal instead of a post (Diagrams adapted8)
Using a Gates Glidden bur, the gutta percha was removed from groups 1 and 2 leaving at least 4-5mm to create an apical seal. Teeth in group 3 had only 4mm of gutta percha removed from the coronal part of the canal. The ferrule in the case of groups 2 and 3 was prepared by making a 1mm wide contrabevel at the root-core junction using a conventional hand-piece with a chamfer diamond bur. Post spaces were prepared for groups 1 & 2 using the para post system (Coltene/ Whaledent Inc, USA). The posts were cemented using Dyract Cem (Caulk/ Dentsply) a dual-cure acid resin modified cement. All the cores were prepared by free hand to a 7mm height using a composite resin (TPH, Dentsply/ L.D. Caulk). All posts were completely covered by the composite. Metal copings of 0.5 mm thickness and 8mm height were fabricated in the laboratory and used to simulate final restoration. They were luted onto the teeth using Dyract Cem (Caulk/ Dentsply). The teeth were embedded in autopolymerising acrlylic resin blocks upto 2 mm below the cemento-enamel junction. The Zwick testing instrument (Zwick GmbH and Co., postf. 4350, D-7900u/m, Germany) was used to apply compressive loads progressively on the restored teeth until failure occurred. The load was applied at an angle of 135 degrees to the long axis of the tooth. This angle simulates the average angle of occlusion between maxillary and mandibular incisors in a class I occlusion. RESULTS
The failure threshold was defined as the maximum load a sample could withstand until fracture. Failure loads, modes of failure, and tooth preparation (ferrule design) were recorded and statistically analysed for significant correlations between design and failure loads. The data was analysed using the SPSS system. The one-way analysis of variance (ANOVA) was used to determine whether the fracture resistance differed significantly among the three groups, and whether differences in the other variables were significant. Results from four specimens were discarded due to errors caused by the testing machine (Zwick machine) and the laboratory technicians. The analysis of variance (ANOVA, table II) showed that there was no significant difference amongst the three groups as regards fracture resistance, although teeth (table I) with ferrule andno post (group 3) required a much higher mean force (1036N, std ±269) to fracture when compared to teeth in the other two groups. Teeth with a butt joint (group 1) required a mean force of (931N, std ±283) and teeth with a ferrule and a post (group 2) required a mean force of (931N, Std ±242) as presented in table I.
DISCUSSION Thymol solution has been used by many researchers16 as a storage agent because of its antifungal activity. It was used in this study because the teeth had to be stored for an extended period as collection of the specimens proceeded. The Parapost system was used because it has a long record of clinical success3 and has been known to represent the industry standard for prefabricated posts. It satisfies the general criteria of a good post system being parallel, serrated and vented 18. Acid modified resin cement (Dyract cem) was used in this study because it has been found to enhance the retention of the parallel-sided posts and increases fracture resistance19. This may be due to the dentine bonding provided by these cements. Composite resin was chosen as the core material in this study because composite cores have been found to have a high fracture resistance 20, 21. Aquaviva 5 suggested that laboratory studies must have some degree of clinical correlation in order to be practically applicable. Therefore the teeth in this study were restored with laboratory made crowns so as to simulate the clinical situation as far as possible. The coronal dentine extension used for all the groups was 2mm because it has been recommended as the minimum length, which can compensate for the difficulties of intraoral tooth preparations22. Posts in some parts of the mouth are subjected to rotational forces. Anti rotational features are placed to counteract these forces. These features can be placed in tooth roots by slotting the most coronal internal position of the post channel or by placing pothole channels or retentive pins in the dentine mesially and distally to the post channel. The most important anti rotatory feature for posts and cores is the placement of a ferrule effect11 circumferentially around the build-up and remaining root stump by extending the crown preparation margins at least 1-2 mm apically to the composite tooth structure interface. In-vitro studies have shown that the ferrule effect significantly reduces the incidence of fracture in non-vital teeth by reinforcing the tooth at its external surface and redistributing applied forces14. However, this study showed no significant difference in the forces needed to break teeth with or without the ferrule (table I). This finding is in agreement with other researchers 16, 23. The mean failure load values of this study and of the two studies mentioned above were high compared to findings by previous studies; Volwiler15 21.6 kg (212 N), and Sorensen and Engelman8 65.3 kg (640 N). The high forces in this study are probably due to the use of the duo cured resin modified cement (Dyract cem, Dentsply) and the cements ability to chemically bond to the dentine and micro-mechanically bond to the post. The results further showed no statistically significant (table II) difference regarding the amount of force needed to fracture teeth with and without posts in this study. These findings are related to another study3 in which a retrospective study was carried out and found that there was no significant increase in fracture resistance gained with intracoronal reinforcement. However, in this study teeth without posts required (1036 N) a higher amount of force to fracture than the teeth that had posts (931 N). This suggests that the use of posts should be avoided when they are not required to provide retention for the core. Table II. ANOVA tables for the force needed to break teeth between the different groups
The relatively lower values (table I) required to break teeth restored with posts in this study were probably due to weakening of the tooth structure during post channel preparation. Therefore when insufficient tooth structure exists to prepare for coronal coverage, a composite resin coronalradicular core may be appropriate as a post and core build-up in the restoration of anterior teeth, if there is sufficient dentinal wall to act as a ferrule. However when evaluating the results of this investigation, it should be noted that there may be limitations to the direct application of in-vitro results to clinical situations. Some of the limitations encountered included; variations among the specimens within the groups, which is inherent with these types of studies because of the natural variation among the teeth that are used. Lack of a periodontal ligament such that the teeth were embedded in acrylic resin, which showed resilience. The number of teeth used in this study were limited such that no conclusions could be drawn from some variables. CONCLUSIONS The two major conclusions from this study are;
ACKNOWLEDGEMENTS
This work was supported by the University of the Western Cape. The authors are gratefull to Dr. Laloo for assisting with the statistics, and the laboratory technicians; Tanya, Valentine and Dr. Rossouw. REFERENCES
Copyright © 2004 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs04023f2.jpg] [hs04023t2.jpg] [hs04023t1.jpg] [hs04023f1.jpg] [hs04023f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}